What can I say? I have had a love affair with research on hypoglycemia. I suppose ever since my colleague and I began the quest of rewriting the Canadian Pediatric Society statement The screening and management of newborns at risk for low blood glucose it has become an interest. Embedded in the statement is commentary on the use of glucose gels for management of neonatal hypoglycemia and based on the sugar babies trial that found treatment of hypoglycemia with dextrose gel reduced admission for hypoglycemia and improved rates of breastfeeding after discharge I have been a proponent. A new approach has arisen in a large study in neonates that warrants some discussion. It tackles hypoglycemia from a preventative approach rather than as a treatment per se and is presented below.
The hPOD Study
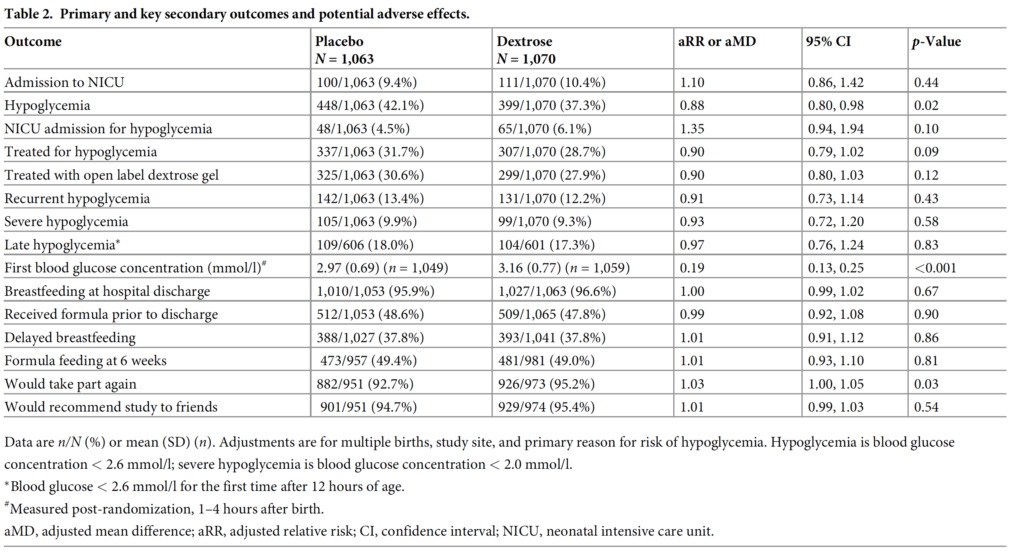
The same group from Auckland led by Jane Harding published a preventative trial in January entitled Evaluation of oral dextrose gel for prevention of neonatal hypoglycemia (hPOD): Amulticenter, double-blind randomized controlled trial. The study approached the problem of hypoglycemia by looking at whether provision of dextrose gel at 1 hour of age along with a breastfeed could reduce admission to NICU. The targeted population were babies with risk factors for hypoglcyemia such as maternal diabetes, late preterms and SGA or LGA infants. Remarkably this multicentre study managed to randomize 2149 infants into dextrose (1078) and placebo 1071) arms which for a neonatal study is pretty big! Blood glucose levels were analyzed on all at risk infants at 2 hours of age and were then followed up every 2-4 hours for the first 12 hours of age and until there were 3 consecutive measurements greater than or equal to 2.6 mmol/L. Given the size of the study it should come as no surprise that the two groups were similar in terms of baseline characteristics. The most common risk factor for hypoglycemia in each group was maternal diabetes at 81% in each group.
In the end the only thing that was different between the two groups was a diagnosis of hypoglycemia with about a 5% reduction in the outcome. Admission to NICU was no different whether it was for any reason or hypoglycemia alone. Treatment with IV therapy was also no different between groups and in addition breastfeeding rates were exceptionally high at discharge at about 96% for both groups. So the conclusion here is that prophylactic glucose gel doesn’t matter much but I have a few thoughts despite this being a VERY large trial and the authors really doing a good job of answering an important question.
My Thoughts on the Outcomes
The study demonstrates that one dose of glucose gel does not affect admission for any reason or for hypoglycemia. I can’t help but wonder if allowing the dextrose gel group to receive one or two more doses could have changed that outcome.
No difference in admission is not surprising since there are many reasons that a baby could be admitted with those underlying risk factors. Low birth weight, TTN, RDS etc would be some reasons and I wouldn’t think would be any different. It might have been better to power the study for admission for hypoglycemia as that to me is the only reason for admission that could be impacted by such prophylaxis.
When your breastfeeding rate in the placebo arm is at 95.9% there really isn’t much room for improvement so not sure a lack of improvement with dextrose gels can really be called here. There really wasn’t anywhere to go but down and previous work suggested that rates can go up. As the saying goes, can you apply the results of the study to my population. I can only wonder what would have happened if the authors were to replicate this study in a population with breastfeeding rates of 80%.
Is the outcome of reduced hypoglycemia a good enough outcome alone to adopt prophylactic dextrose gel? I don’t think so as there was no difference in groups between recurrent or severe hypoglycemia which is what likely matters most to neurodevelopmental outcome. Curiously the mean initial blood glucose was 2.97 and 3.16 in the placebo and glucose gel arms respectively so I am not sure how hypoglycemic this population really was. Yes there were about 40% in each arm that were hypoglycemic but only 10% were severe and almost 90% never had another episode. It’s possible that just by chance these children were on a very mild spectrum and therefore prophylaxis had little effect since they really were only going to have transient hypoglycemia.
In spite of my comments above I believe the authors did a fine job trying to answer an important question which to be honest others have wondered about before. For now I won’t be recommending this in my own institution but I do wonder what project will come next from this group that keeps on producing great work in the area of neonatal hypoglycemia.
This post is special to me. A redemption of sorts. When I was a fellow in Edmonton in the early 2000s my fellowship project was to see whether heliox (helium/oxygen) given to piglets with meconium aspiration syndrome (MAS) would improve ventilation and measures of pulmonary hypertension vs controls. Why heliox? There had been work done with this gas for other conditions and the lower viscosity of the gas (who hasn’t sucked on a helium balloon to see the effect of helium) means that the flow of the gas in a tube is more linear that regular air. Turbulent flow as with air/oxygen mixtures creates more resistance to flow than linear flow with heliox. Imagine if you will this linear flow slipping more easily past particles of meconium partially blocking airways and you get the idea of why heliox might work. One thing to bear in mind though is that as your FiO2 goes up the percentage of helium drops so the properties described work best at low FiO2 so flow is more linear.
I collected meconium from diapers in the NICU and created a NS slurry of meconium and then instilled it into the trachea’s of these piglets through a tracheostomy (they were too small to intubate for me at least). A flow probe was put around the pulmonary artery to look for evidence of pulmonary hypertension. We saw some interesting trends but the paper never saw the light of day for a variety of reasons that I won’t go in to here. Originally I had wanted to do the study as a small RCT in humans but I was advised that although heliox is an inert gas I should do the animal study first. That was the end of the heliox story as far as I was concerned as I hadn’t thought much about it since that time. I will admit though that anytime I had a baby with bad meconium aspiration syndrome though the thought did pop into my head.
The Study Has Arrived
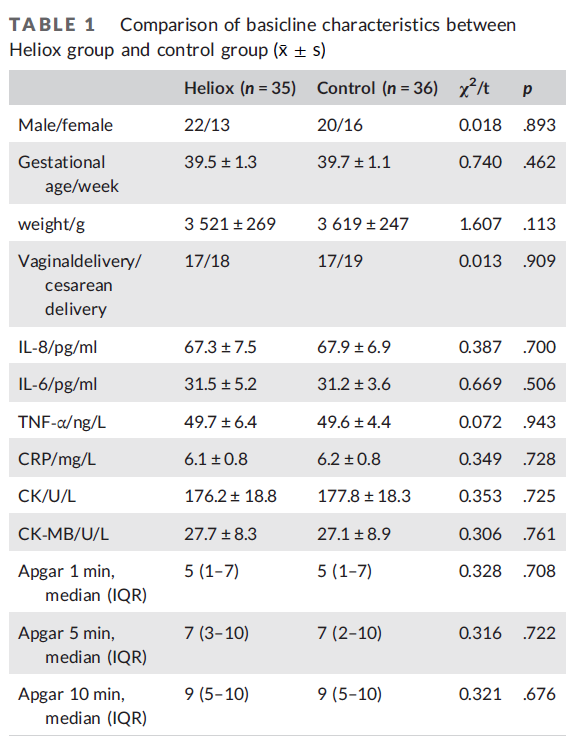
Imagine my surprise when this week an RCT from China entitled A randomized single‐center controlled trial of synchronized intermittent mandatory ventilation with heliox in newborn infants with meconium aspiration syndrome came across my inbox. The authors used a power calculation based on some previous work in RDS using heliox to determine they needed 28 neonates in each arm to show a difference. In the end they managed 71 total with 35 in the heliox and 36 in the control arm. Inclusion criteria were a diagnosis of MAS on x-ray, GA ≥37 weeks and ≤42 weeks, need for intubation due to a pH <7.2/PCO2 >60 mmHg. The study could not be blinded as one would not be able to hide the large tanks for heliox so for any study like this it would be unavoidable. One thing that differs in terms of management from my own practice is that the authors in this study used SIMV pressure limited ventilation as the ventilatory strategy as opposed to AC/VG that my unit would typically use. Initial ventilator PIP of 15–28 cmH2O, PEEP of 4–10 cmH2O, and RR of 15–45 breaths/min; FiO2 of 0.21 to 1 to reach the target oxygen saturation (SpO2) of 90%–95%. The intervention group received heliox for 6 hours and then switched over to air/oxygen while the control group was ventilated with air/oxygen from the start. The extubation criteria included PIP ≤15 cmH2O, gradually enhanced effective spontaneous breathing, a ventilator breathing frequency ≤10/min, and normal blood gas analysis results. The main outcomes were PaO2/FiO2 (P/F), the extubation time and the hospital length of stay in the NICU. Aside from measuring the ventilatory responses and time of extubation the authors also examined the effect of heliox as an anti-inflammatory agent based on previous results demonstrating markers of inflammation can be attenuated by use of the gas.
The Results
To start with, the babies in both arms were equivalent at the start of the study in terms of inflammatory markers and some clinical variables.
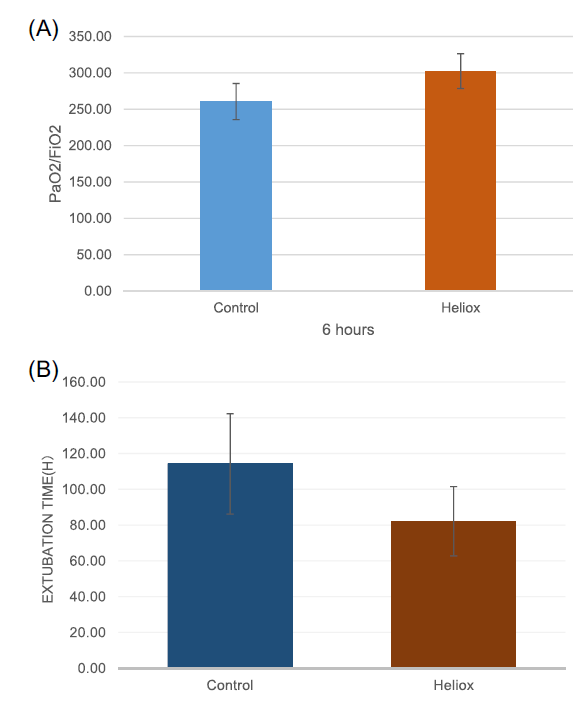
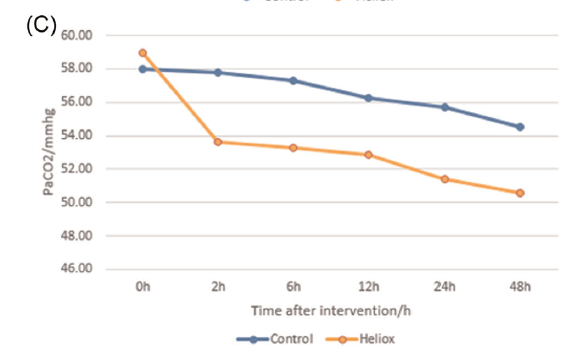
As you will see from the following figures a number of important findings are noted. The main marker of oxygenation used for this study was the PaO2/FiO2 ratio and this was statistically different (301 ± 22 vs. 260.64 ± 24.83, p < .001). Secondly, extubation time (78 ± 30 vs. 114 ± 28.07, p < .001 and length of hospital stay in days were also shorter 15.3 ± 4.2 vs. 19.11 ± 4.01, p < .001.
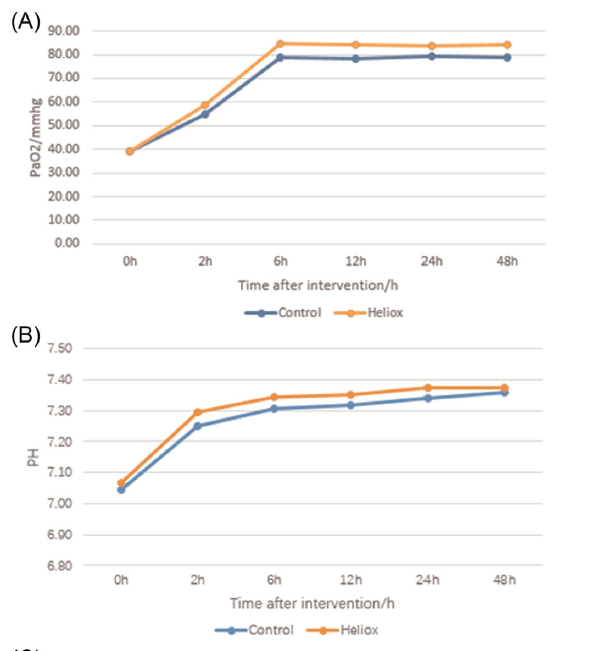
The authors state that the following markers of pO2, pH and pCO2 shown in the graphs were all significantly improved in the heliox group but looking at the first two I find that hard to believe as the curves look almost superimposed. pCO2 however could be different in particular given the linear flow described above so ventilation might be improved.
Finally, across the board, markers of inflammation were noted to improve with administration of heliox as well as markers of myocardial injury. The gas may have done what it was supposed to do.
I wish the conclusions were that easy
I want to like this paper so badly. Sadly, I have some pretty significant reservations. It is helpful to see that the two groups began at a similar PaO2/FiO2 ratio. What is missing though is the ventilatory requirements to get to that point. There is no information provided as to the mean airway pressures or PIP/PEEP for each group over time to get a sense of whether the two groups in terms of severity of illness were the same. Yes we know that the inflammatory markers at the start were similar but could the difference in changes of inflammation relate to a progressive rise in the control group that were just sicker rather than a protective effect of heliox to reduce inflammation? Also when one looks at the change in pCO2 how do you interpret that without knowing the minute ventilation to achieve those data points? It is really unfortunate that the authors did not use oxygenation index (MAP X FiO2/PaO2) as this would have taken the ventilation component at least into account. Would be helpful as well to know the weaning strategy in each group as without blinding might the authors have reacted more aggresively with weaning of the ventilator to get to extubatable settings knowing that the babies were receiving the intervention. As there was no weaning strategy planned out from the start we can only guess. Lastly, one could have possibly gotten around the inability to hide the heliox tanks by having a Neonatologist not on service take each blood gas data and sight unseen suggest changes to ventilation without being able to see which arm a baby was in.
I will end on a positive note though. It has been almost twenty years since I did the piglet study using heliox. I had always hoped that this research would see the light of day in a human model although my piglet data didn’t show much benefit however the intervention was shorter than this study. I think this study is worthy of being repeated using a different mode of ventilation that does not rely on manual changes to PIP but rather by using a VG mode the baby would be gradually weaned as compliance improves. Any further study needs to address differences that were missing from this paper as well. I don’t think this is the last we will see of heliox and I look forward to seeing another paper although if it takes another twenty years I may be out of this line of work.
I had the opportunity recently to give a talk on strategies to reduce BPD in our preemie population. For the talk, I used as a springboard the recommendations for reducing BPD as laid out by the Evidence Based Practice for Improving Quality (EPIQ) group. There are far too many recommendations for optimal care to go through but the point of this post is to highlight one strategy that I think is deserving of discussion.
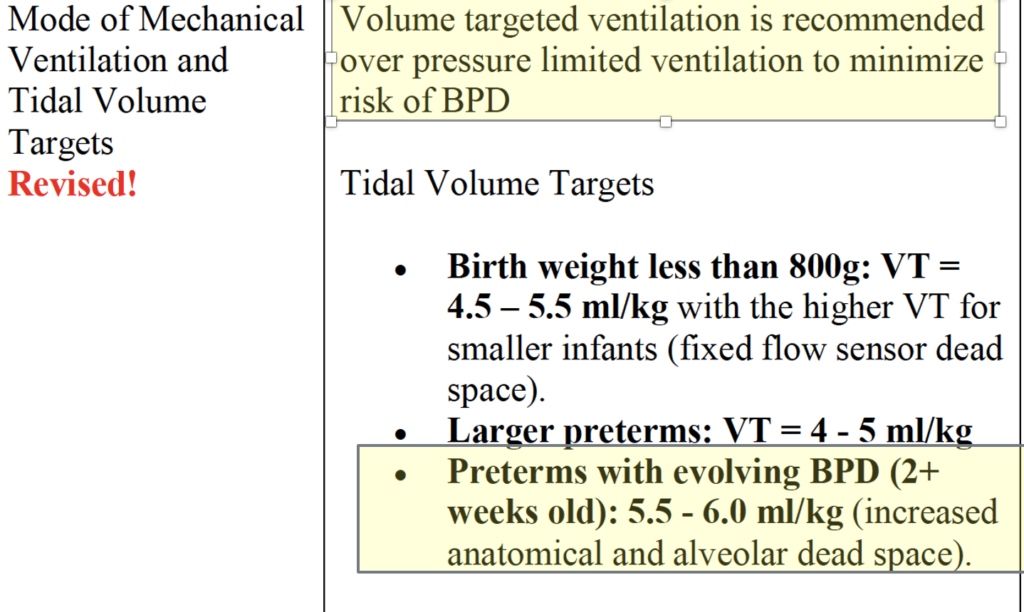
That volume targeted ventilation is recommended is no surprise. Setting a desired volume and allowing pressures to fluctuate rather than fixing a pressure and allowing volumes to fluctuate reduces the risk of both atelectotrauma and volutrauma. A recent paper Early volume targeted ventilation in preterm infants born at 22-25 weeks of gestational age has added further arguments in those at the smallest gestational ages by reducing episodes of hypocapnia and increasing likelihood of extubation by 24 hours compared to those on pressure limited ventilation.
Are Bigger Volumes Better With Time?
It is the second highlighted piece above that has left me scratching my head. Going way back to my residency I was taught that the ideal tidal volume is somewhere between 3.5 – 4.5 mL/kg and we should try and keep PIPs less than 35 cm H2O as an absolute maximum. In reality we typically would switch to the high frequency jet ventilator if pressures were increasing above 25 cm H2O in an effort to avoid volutrauma by increasing volumes further or barotrauma from excessive pressure. The main thrust of the argument was that big volumes hurt the lung so one is better off being gentle and inflating the lung with PEEP and then using the more gentle pulse of the HFJV after that. To be sure in the early stages of the neonatal course excessive volumes and pressure can commit the patient to a significant risk of BPD and meticulous attention to respiratory care is needed. The question for today is whether after 2 or 3 weeks of age, babies with developing lung injury need more volume on conventional ventilation or whether continuing on the HFJV is the way to go. I will let you in on a secret right away though. There is a systematic review on the subject.
The problem is it only includes one study from 1991 which is before antenatal steroids and surfactant as standards of care so not much to take from this paper.
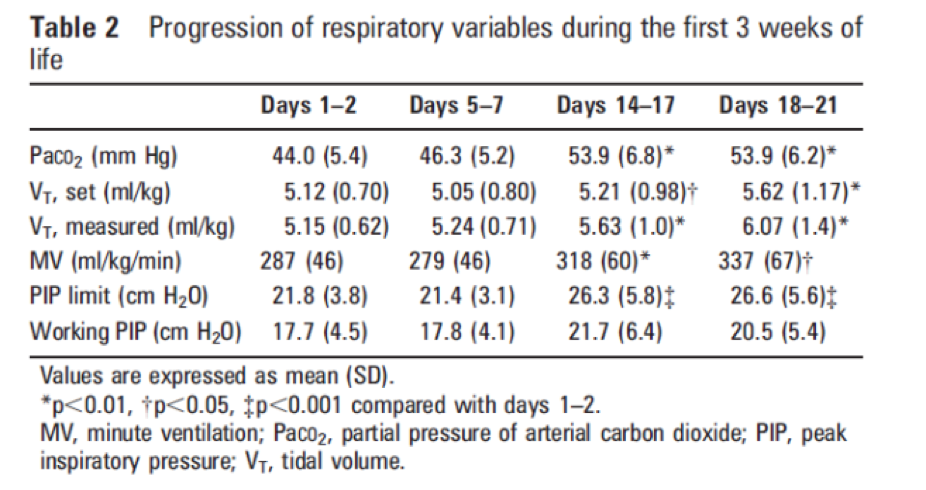
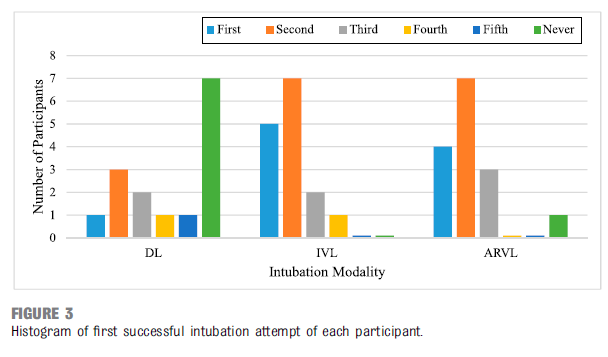
As shown in the table above the needed tidal volumes rise over time. The PIPs remain acceptable (below the set limits) but the volumes rise to close to 6 mL/kg by three weeks of age. If these results are generalizable to our own population this would mean that using our units current levels of 3.5 – 4.5 mL/kg would leave these older infants short. If so is it any wonder we see high pCO2 triggering a need for HFJV. The authors conclude here that the progressive dilation of the trachea and proximal bronchi over time from ventilation increase dead space and are responsible for the rise in needed Vt.
The next study Volume targeting levels and work of breathing in infants with evolving or established bronchopulmonary dysplasia was published in 2019 by Hunt et al. This study looked at 18 infants less than 32 weeks and randomly assigned them once older than one week of age and still ventilated to 20 minute periods on 4,5,6 and 7 mL/kg of Vt in random fashion. The median GA was 26 weeks and day of study 18 days. The outcome of interest was measurement of work of breathing using the Pressure-time product of the diaphragm (PTPdi). The findings are below.
One did not see a significant improvement in work of breathing until 7 mL/kg was reached and you can see a progressive rise in minute ventilation needed to maintain normocapnia over time. This study supports the previous one in suggesting that over time there is an increase in dead space and if we want to reduce air hunger which could be represented by work of breathing we need to consider higher volumes.
The Damage is Done
Its an imperfect science that we are looking at and there is no doubt there will be readers of this post that will cringe at the volumes being discussed. I think what this really comes down to is whether you think the damage is done by 2-3 weeks. We of course don’t officially classify babies as having BPD until 36 weeks but if we are being honest we often know or can predict which ones are destined to get it. Is it better for the babies to be put on high frequency ventilation for weeks or to be given some larger volumes on conventional ventilation? Hard to say based on the evidence as there really isn’t much to go by. One thing that does need to be considered is long term high frequency ventilation and the need for sedation. Many of our kids on weeks of such therapy need progressively more sedation and what effect does that have on the developing brain. On the other hand if excessive volumes even at 2-3 weeks lead to increased damage to the lungs are you risking a prolongation on the ventilator or increasing the need at some point for a tracheostomy?
In the end I don’t think at the moment anyone knows. If you move from one center to another though and see completely different approaches I hope that by reading this post you will at least understand where the differences in practice come from.
In the end we are all just trying to do what we believe is best for the baby.
Cool title for a post I think. If you have children or even if you are an adult who likes to play video games you would be aware of virtual reality headsets. These headsets take games to a new level by immersing you in the experience so all you see is the game in your field of vision. It is easy to get lost in this world and lose your sense of the outside world. It seems reasonable then that someone might think to adapt some of the principals of this type of gaming to use in medicine.
I am no stranger to posts on video laryngoscopy having written about it several times already. A search of this site should easily find posts on the topic if you are so inclined. In these posts I think I have made a compelling argument for the use of videolaryngoscopy over direct laryngoscopy to improve inubation success.
A New Way of Doing Things
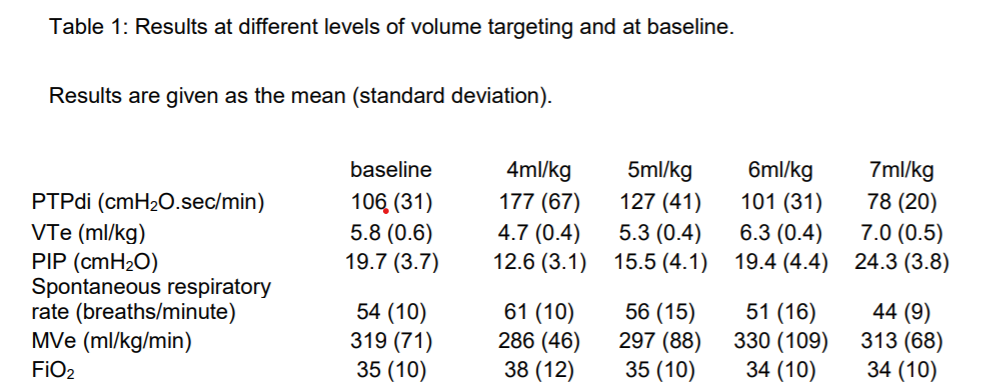
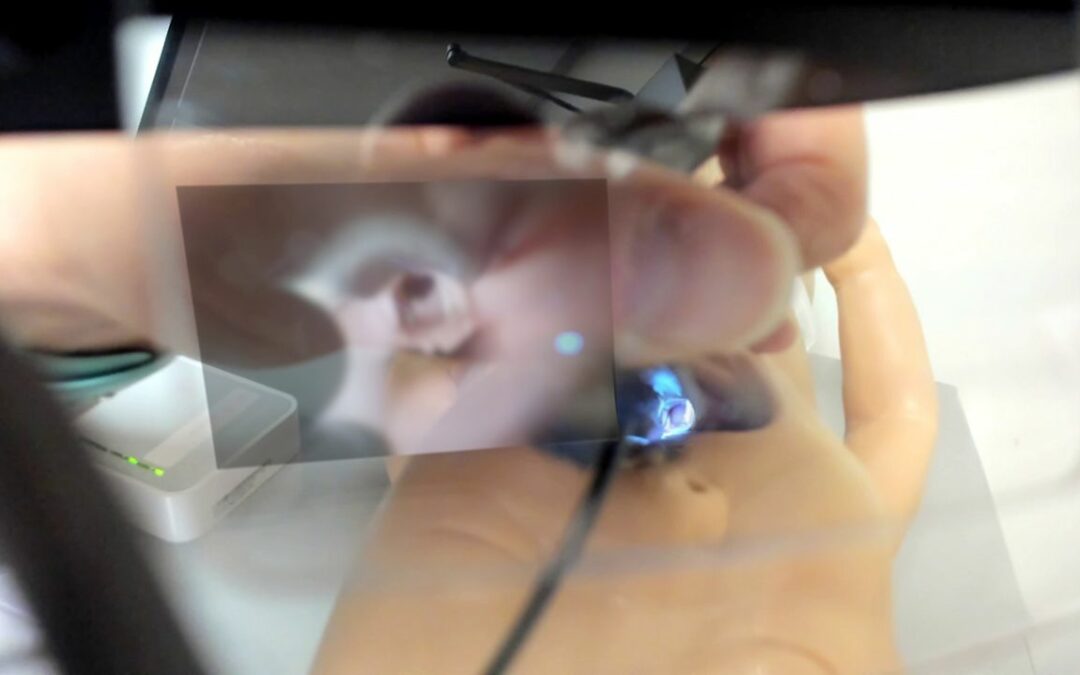
In each of those posts there has been a comparison of two groups in with one uses IVL in which the video image is generally off to the side of where the intubation is taking place and DL or direct layngoscopy with video aid. A new study entitled Augmented Reality–Assisted Video Laryngoscopy and Simulated Neonatal Intubations: A Pilot Study by Patricia L. Dias, et al compares a third method to the other two. The third method is to use a disposbale laryngoscope as shown below with a video camera attached that connects to a tablet. The video captured on the laptop is then sent to glasses the person intubating is wearing that is projected into the line of site as per the image below. In essence its like a car with heads up display. No need to take your eyes off the airway as you are seeing it directly in front of you. Where the tech becomes even more interesting is that the person on the tablet can make notations on the video that appear in the view of the person wearing the glasses. For example one could put an arrow showing where to put the ETT or label the esophagus as such.
In the study there were 45 nursing participants who were assigned to one of three different intubation strategies being DL, IVL and Augmented Reality VL (ARVL). As such there 15 participants in each arm. Each participant was read a script on how to intubate and then had 5 consecutive intubation attempts on a maniken using a miller 1 blade.
How Did They Do
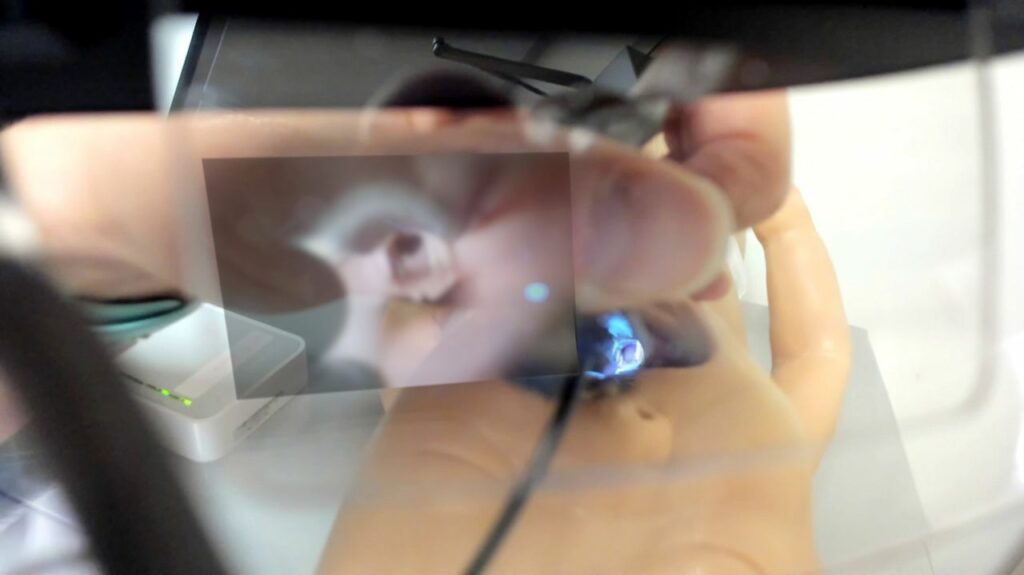
Interestingly there was no difference in success with the ARVL vs the IVL in terms of success on being able to get the ETT into the manequin successfully as shown below but both were better than the DL.
Looking at the details of the success and failure there was also no difference in the two types of videolaryngoscopy.
So Where Does That Leave Us
At the very least what we have seen is once again the ability to intubate is enhanced with VL. There was no difference seen in this group of nurses learning to intubate whether they used a indirect or augmented reality VL. This however is a small study and really to me is a proof of concept study. The authors created a novel method of doing VL although one could argue it is not that differrent that use of the CMAC with the small screen attached to the top of the laryngoscope
The difference though is in the ability of the instructor to write feedback on the tablet and have that show up in the line of sight of the intubator. I see this novel ability as a wonderful educational tool. There is not a learner out there who hasn’t had the experience of looking down at an airway and thinking “what am I looking at?” Sometimes with secretions it can be awfully hard to determine which structure is what. Having someone on a tablet seeing the image you are seeing and rather than having to describe to you what you seeing, they could draw it for you I think is a huge advance. Like many pilots I would suggest this is not the last we have heard of this technology. With this in the literature now I suspect there will be trials to come with more developed devices rather than those put together piecemeal. If these larger trials with less and more advanced intubators demonstrate increased rates of success I could see this becoming the new standard for video laryngoscopy.
This post is a written as a tribute to John Minski RRT who taught me much about ventilation over the years and has been a champion for innovation in our unit. As he prepares to move on to the next phase of his life I thought it would be a nice send off to talk about something that he has been passionate about for some time. That passion is inhaled nitric oxide for more than just pulmonary hypertension.
Prior Evidence
This is actually nothing really new. For a review on the background behind the theory you can read The potential of nitric oxide releasing therapies as antimicrobial agents. While we think of iNO as being a drug for pulmonary hypertension it has other capabilities. It can diffuse across cell membranes and damage pathogens by causing nitrosative and oxidative damage. The amount of iNO needed though to accomplish this bactericidal action is much higher than the typical levels of 20 – 40 ppm that we use. Last year in August Bogdanovski et al published Antibacterial activity of high-dose nitric oxide against pulmonary Mycobacterium abscessus disease. They describe a protocol of providing 30 minute doses of 160 ppm for 21 days in a 24 year old patient with cystic fibrosis who was infected with mycobacterium abscessus. While they were not able to eradicate the organism, they were able to demonstrate functional improvement in the patient. Also notable was the absence of adverse effects in terms of methemoglobin levels. Other prior research in-vitro has shown iNO at high levels to be truly bacteriocidal as per the review above.
In this paper they describe the use of iNO at 160 ppm in 5 spontaneously breathing patients with confirmed COVID19 infection. This was provided as a rescue therapy in the absence of any high quality therapies for this disease. The protocol was to give them the same dose of 160 ppm for 30 minutes at a time until resolution of their symptoms with those that received multiple treatments getting anywhere from 5-9 courses. In each case after each 30 minute period the treating physicians measured levels of methemoglobin and nitrogen dioxide and found in each patient acceptable levels after these brief exposures.
Results
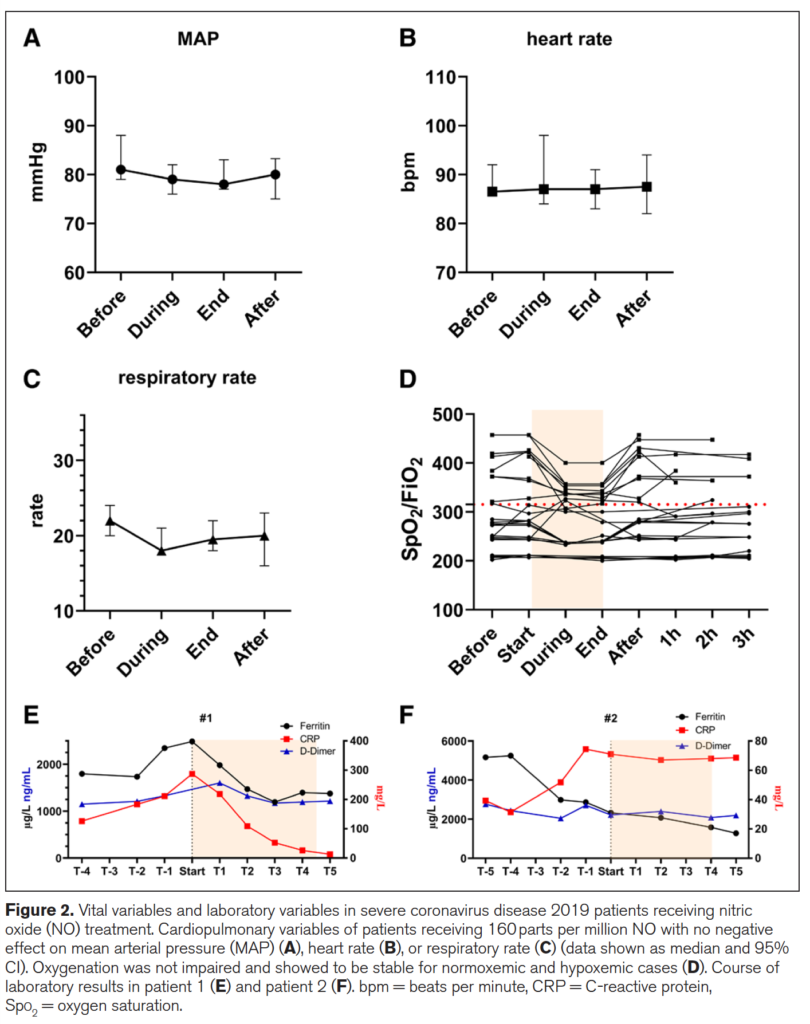
Of the 5 patients treated 2 died from COVID19 and three survived. The two patients who died interestingly were the ones who each only received one treatment each. The other three received 5, 8 and 9 treatments respectively. The authors recorded mean arterial pressure, heart rate, respiratory rate, SpO2/FiO2 and finally measurements of inflammatory markers in the two patients who died (E) and the 3 who survived in (F) in the figure below.
What is interesting from the figure above is the reduction in respiratory rate during treatment (certainly could be placebo from believing they will get better) but the oxygenation during the treatment improved as well. Could this be from a reduction in associated pulmonary hypertension? Certainly could be. Looking at the patients who died in (E) vs the ones in (F) who survived (patient 3 not shown) demonstrate that use of iNO stopped the rise in CRP and in the case of those who died reduced it significantly. There could be an argument made then that the changes in respiratory pattern observed during treatment are associated with a concomitant attenuation of inflammation. This treatment just might work but of course needs far more studies to be certain of that. On that note a review of iNO for this type of indication reveals there are currently 16 studies enrolling in this area of research so I imagine there will be more info to come with this story.
What about the neonate with pneumonia?
I sent this paper around to my colleagues and it generated some great discussion. I am no Ethicist but the question raised was could this be considered a “last ditch” treatment for the neonate succumbing to a pneumonia? I have no doubt if you are reading this that you will have seen in neonatal units around the world that there are infants who develop pneumonia unresponsive to traditional treatments such as iNO at regular doses, antibiotics, higher PEEP, surfactant etc. If we have this knowledge with respect to the potential use of iNO at high dose and a positive impact on pulmonary infective disease is this something that should be offered to parents?
We have no date to my knowledge in babies on the use of this type of dosing but it comes down to a question of what is the alternative? If a patient is dying on the ventilator are we at the point of knowledge here that it is worth offering the family this treatment? One could do so with full disclosure about the lack of neonatal data both for effectiveness and safety. Or do you fall on the side of it could be harmful and expedite death so should not be used. If you use it though and wait till the patient is in extremus on 100% oxygen might it be too late? Do parents have the right to know when they ask the question “is there anything else you can do?” For me I think the answer is that there should be a discussion with this evolving research out there. I am comfortable with it as long as the parents understand the potential for it to make things worse and shorten their time with their child. Alternatively if they choose not to that is their prerogative but should they have the choice when the competing outcome is death?
I can’t tell you whether you should or shouldn’t offer this in your institution but my suspicion is that you will be discussing this among colleagues before long. Who knows you might just one day say you saw it here first!
Thanks John M for the inspiration and keep sending those articles!