As a health care provider, I am pulled in many different directions when caring for babies in the intensive care unit. Our front line staff doing the day to day or moment to moment care and procedures are often pulled to an even greater degree and need to make choices continually as to priorities for care. As the saying goes there are only 24 hours in a day or in this case a call shift although many institutions have shortened shifts to more humane 8, 10 or 12 hour days. When you are faced with so many different calls for assistance it does leave one in a predicament as to how all of the work will get done.
A Baby With Hypoglycemia
When it comes to hypoglycemia it is a common problem in those at risk. As per the Canadian Pediatric Society statement “Some 12% to 14% of well, AGA, breastfed newborns have a blood glucose level of <2.6 mmol/L in the first 72 hours after birth”. Add to this infants who are IUGR or SGA and you have the potential to see this again and again if you work in our field. Fortunately, most infants have one or two low blood sugars and then normalize but certainly not all. I recall a situation in which a physician had a terrible night on call. When I say they were busy it was the understatement of the century. They were managing multiple sick patients overnight and fielding several calls overnight about a baby who was well aside from a pesky problem of repeated episodes of hypoglycemia. When I arrived in the morning and was reviewing the charts of the patients I noted something both peculiar and concerning. The babies with complicated and high acuity care had ample documentation of the night’s events but the baby with low blood sugars had no notes at all. Now based on my conversation with the physician it sounded like he managed the patient extremely well and followed our guidelines but there was nothing to document that this had been done. All told there were 5 or 6 low blood glucoses overnight. Before leaving for his shift, I called him and insisted he return to document what happened with the “straightforward” baby with hypoglycemia. As per the title of this post my concern was that to not document was at his peril!
Litigation Risk
If most physicians are being honest, the knowledge that we could one day face litigation for something we did or didn’t do is something that is in the back of our minds. In Canada, after a personal injury there is a general limitation of 2 years to file a statement of claim for a personal injury. In the case of a newborn this means that after a period of persistent hypoglycemia a family has up to two years to file a claim. Imagine for a moment that after hundreds of patients later you were asked at a year out for the details of that one “innocuous” baby with low blood sugars. Would you remember? I doubt it. Now of course there would need to be an injury such as cerebral palsy, developmental delay or seizure disorder to sue. This is one reason why the story gets even more challenging in the medicolegal space. Since one needs to have injury to incur compensation you may not hear about a lawsuit until the former newborn is well into their mid to late teens. In terms of determining the true impact on a child’s life, questions about school performance and ability to live independently won’t be known for many years. So let’s ask the question again. What would you remember about a baby with hypoglycemia and your thoughts about them 15 years after the fact and 1000s of patients later. Not much if anything. Now you could perhaps fall back on the nursing records but they too might be faulty or if you actually deviated from the protocol in your unit even slightly you would have nothing to fall back on to jog your memory.
Why Don’t We Document?
We know we should but here are some reasons it doesn’t happen.
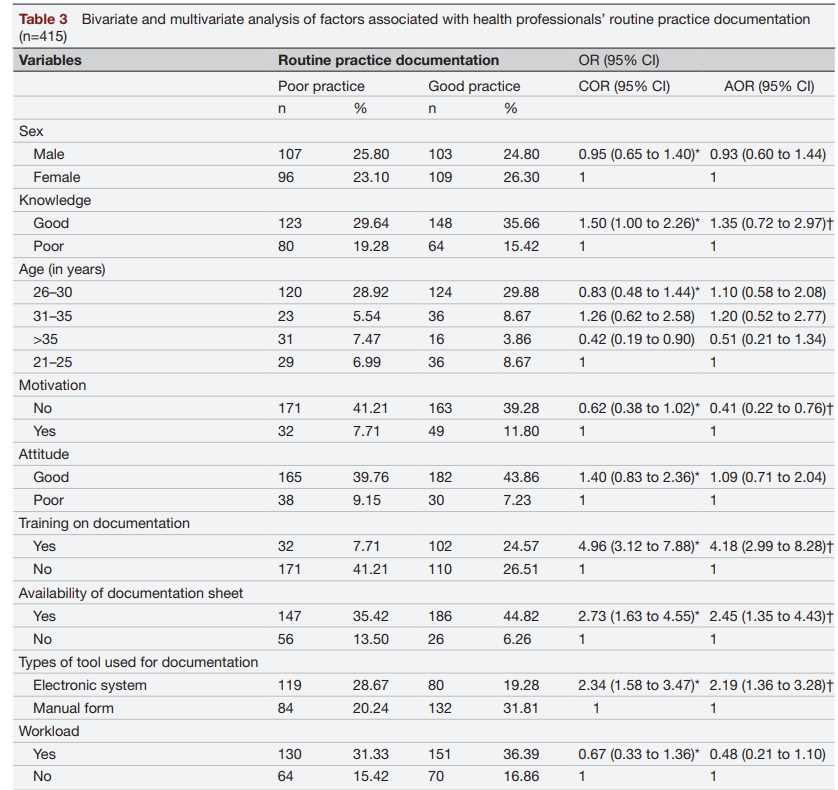
We are too busy. This is probably the most common thing that you hear when asked why it didn’t happen. This is often followed by “I know I should though” There is research in the field of documentation which suggests that this actually may not be a universal factor especially in a non-intensive care environment. An institutional survey in Ethiopia revealed some interesting findings in an attempt to answer this question. They looked at 415 respondents in the paper Health professionals’ routine practice documentation and its associated factors in a resource-limited setting: a cross-sectional study. Here is a summary of the findings.
Looking at the final column representing the adjusted odds ratios what you see is that at least in this institution workload did not statistically bear out as an issue. Training on how to document carried a strong risk with the presence of specific training on how to document carrying a fourfold impact on good documentation. Having a formal documentation sheet for those using paper and using an electronic medical record also increased the chances of regular documentation. One thing that stands out though is motivation. Feeling unmotivated decreased the chance of documentation. As we have come out of the pandemic news stories abound of physician burnout. I can’t help but think that the lack of motivation for many physicians which goes against their background fear of litigation stems from burnout.
“The things that influence whether you can or not, are the busyness of the shift. And look, you know, we’ve all got days– whether we have good days where we document everybody, and when you get complaint, you start documenting everything left, right and centre, but that wears off after two days because you can’t get your job done.”
“Flow pressures, I think, impact significantly … if there’s a drive to move patients on …that compromises the quality of the notes.”
“I think putting it down helps you to make the decision about what to do better. I don’t know that I could make a decision without that, but I guess it makes me more confident in that decision. It doesn’t mean I have to write everything down, it means I need to just think about the relevant points for the decision that I’m involved in making. I just think it makes youmore confident in the decision that you’re making.”
The first quote speaks to human nature. We know we should be documenting, and we know that failure to do so is risky but time heals all wounds. Our brains lose that sense of concern, and we move on to the next patient. The second addresses the realities of working in a busy practice. The needs of the system and hospital are to achieve good patient flow which allows more patients to be seen, shorter wait times etc but the risk to this is that it leaves physicians with little time to document the patient journey. Lastly, the final quote brings an important concept to the discussion. The simple act of documentation may lead to improved care. As you lay out your thoughts other ideas or differential diagnoses or treatment options may spring forth.
Solving the Issue
I don’t want to disappoint but I don’t have a one size fits all solution to this. Working in intensive care my whole career I can see the barriers in my own field but how this compares to an office-based practice as a family doctor or in a psychiatrists office I don’t know. I suspect we all have some barriers in common and others completely foreign to one another. Electronic medical health records may help to increase efficiency in documentation but there are papers out there suggesting in some cases they can also slow people down (especially if you aren’t that tech savvy).
One thing that I hope is motivating is the realization that especially in the newborn space, it may be years before you hear about a baby that did not do well after discharge. In Neonatology we rarely find out what happens in the long run to babies after they leave our units which leads to these infants being further and further away from our minds. Knowing this and I hope this is generalizable to all health care providers there is no time like the present to document your findings and management. One possible solution however if available to you is if your hospital provides an option for secure remote computer access to the electronic health record. Many of us have busy lives outside the hospital so staying the extra hour to catch up on documentation when the shift is over may not be possible. If you have the option to go home, have a cup of tea before falling asleep and jotting down some notes in the EMR from the comfort of your home that might be an option to consider. To not document an encounter at all is to do so at your peril!
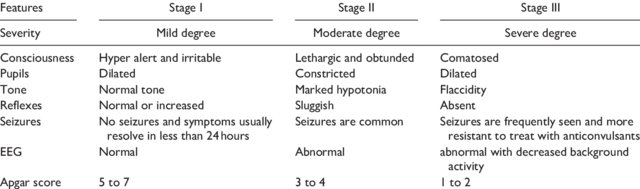
Hypoxic ischemic encephalopathy is a very scary condition for both families and health care providers. In my career as a Neonatologist one of the greatest accomplishments has been the recognition that 72 hours of moderate hypothermia can make a big difference to the outcomes of such children. In days gone by our best estimates of outcome relied on Sarnat staging of HIE.
Since the cooling approach was adopted widely however I have relied more on a wait and see approach when advising families on what to expect. On some occasions, is spite of cooling babies go on to develop significant cerebral palsy but in other cases babies who one would have predicted would have dismal outcomes have done quite well. Our best estimates at the moment are that cooling for HIE reduces the risk of death or moderate to severe disability by about 25% with a confidence interval of 17 – 32% around that estimate.
Why would pCO2 matter?
Carbon dioxide has a role to play in outcome and has been the subject of several papers. The theoretical point is that very low carbon dioxide levels lead to vasoconstriction of blood vessels. When it comes to HIE one would be quite worried about vasoconstriction of blood vessels such as the carotids carrying oxygenated blood to an injured brain. Once injured the brain is not going to tolerate further oxygen deprivation and in particular those areas that are teetering on the edge of survival could be tipped the wrong way if further hypoxia is experienced.
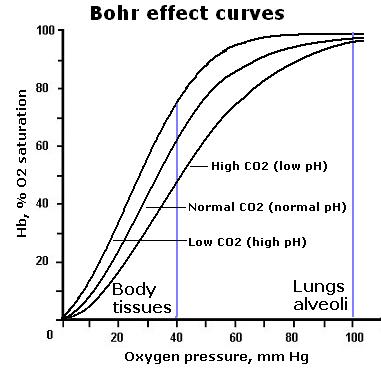
Another reason why CO2 matters is due to something called the Bohr effect. For those of you who are scratching your heads and recollecting this term from your training it has to do with the influence of pCO2 on hemoglobin oxygen saturation. The relationship is represented by the following figure.
In the presence of declining pCO2 there is a shift of the oxygen dissociation curve to the left. This means for that as PCO2 declines more of the circulating oxygen will be bound to hemoglobin. In most cases you want your hemoglobin to be great at carrying oxygen but when your tissues are starved of oxygen and injured that is not what you want. You want a selfless hemoglobin molecule that is more than happy to release its oxygen to the tissue. That is not what you get as pCO2 drops.
Why would pCO2 be low at all?
There are a few reasons for this. The first is that many infants born after an asphyxial event have a metabolic acidosis. Our bodies naturally like to maintain a normal pH. In order to do so if your HCO3 in the blood is low you need to blow off CO2 to compensate. The hypocarbia in this case is compensatory but the body in so doing could make matters worse for the brain.
The second reason has to do with both injured tissue and that which is cooled. As metabolic rate decreases the amount of CO2 generated will drop. If you remember the Krebs cycle (shudder) there is a fair bit of CO2 generated from aerobic (oxygen rich) metabolism. If this is reduced so to will the production of CO2. As cooling serves to reduce metabolic rate so the CO2 production would be expected to decrease.
So does it really matter?
The reason for all this preamble is that a “mini-systematic review” has found the CO2 matters to outcome. The review is entitled Hypocarbia is associated with adverse outcomes in hypoxic ischaemic encephalopathy (HIE) and included 9 studies on influence of pCO2 on outcome. Before we look at the results it is important to acknowledge that all of the included studies were retrospective so methodology in each study is not standardized. How one even defines severe hypocarbia varied from <20 mmHg to anything under 35 mm Hg. The other issue is that each study looked at a different period of exposure from the effect of a couple hours to the effect over the first three days of life. The included infants were all cooled so it gives us at least an idea of the effect in a modern cohort of cooled infants.
The summary of the results was that CO2 mattered. As little as a couple hours of very low CO2 levels were found to be associated with adverse outcomes.
The problem of course is the chicken and the egg argument. The most severe hypocarbia might be seen in those with the worst metabolic acidosis. As mentioned above the response to metabolic acidosis is to blow off CO2. Therefore, the worse the metabolic acidosis the greater that respiratory drive.
Strategies to control the pCO2 of course exist. In the presence of a critically low pCO2 one can intubate and control ventilation through sedation and paralysis. This can lead to other issues though as if you normalize the pCO2 in the presence of a significant metabolic acidosis the pH is likely to take a nosedive. The myocardium as it turns out doesn’t like low pH and in fact cardiac output in animal models begins to decrease the closer you get to a pH of 7 and becomes significantly worse as you go beyond that point.
At best then I think one can aim for converting severe hypocarbia to moderate until the HCO3 begins to recover. Based on theoretical issues of oxygen delivery to tissues and cerebral vasoconstriction, notwithstanding the retrospective nature of this review it does make sense to me that there would be a link between severe hypocarbia and outcome. We will likely never see an RCT targeting normalization of pCO2 vs tolerance of hypocarbia in this population so for the purists out there that don’t like this type of retrospective analysis I suspect outside of an animal model this is as good as its going to get.
Maybe avoiding anything with the word severe attached to it though is sensible when it comes to this population.
The newborn brain could be described as finicky at best. One of the most difficult things to treat are those things that we can’t see. When a baby is delivered and goes on to develop neurological manifestations, it remains a difficult puzzle to sort out as to what the cause is. Of course, we use all manner of technology to sort this out. The use of EEG, amplitude integrated EEG are helpful in this regard to give us a window into brain excitability but we use all manner of technology to sort this out. When it comes down to it, though we often rely on clinical signs to give us a best guess into whether or not hypoxic injury is at the root of the problem. This, of course, is not always easy as although we have criteria such as those written out by the Canadian paediatric Society to rely on, not all babies fit nicely into the box that provides an easy diagnosis.
For reference, these are the criteria that are recommended by the Canadian paediatric Society for determining who should receive therapeutic hypothermia.
In spite of these criteria, sometimes when babies have Apgar scores or cord blood gases that don’t meet criteria for therapeutic hypothermia, they may still go on to have a seizure. In some of these babies, it is likely that they still experienced a hypoxic injury at some point in time that they have recovered from. In these cases, having a super imposed, metabolic, derangement can tip the scales and cause an already excitable brain to manifest neurological manifestations.
The Brain Does Not Like Low Sodiums
One such abnormality that can tip the scales is a low serum sodium. Babies can develop such derangements from a hypoxic insult that leads to an acute kidney injury. The resultant damage leads to water retention from a poorly functioning, kidney and a dilutional effect on the bloodstream. This usually occurs over time and is not commonly present in the first few hours after birth. When this is seen though with sodium levels below 125 in the first few hours after birth, the likely cause is not renal injury. What is interesting about this phenomenon is that the etiology is most likely related to factors that occurred during labour.
Pregnancy its self has a tendency towards, maternal impairment of water excretion. There is a higher volume status in the pregnant woman and some degree of impairment of excretion of a water load. Maternal hyponatraemia has been described in situations of maternal water, intoxication or provision of excessive dilute fluids to the labouring mother. Add to this, that there is cross-reactivity between oxytocin and ADH receptors in the kidney, and you create a potential problem that a mother can become hyponatraemic simply from frequent administration of oxytocin or Syntocinon. It is possible therefore to have a mother in labour who receives an excessive amount of fluid whether by oral intake or IV and with oxytocin administration develop hyponatremia herself. What follows in terms of the fetus who is an innocent bystander is the eventual development of hyponatremia in utero. As the maternal sodium concentration declines this leads to a difference in maternal and fetal sodium levels. Water flows by osmosis to the fetus and begins to dilute out their blood and bring the sodium levels in line with maternal levels. What comes next can be troublesome to the fetus.
Resultant Seizures
Blake O et al published the paper Therapeutic hypothermia and outcome in hyponatraemic encephalopathy secondary to maternal water intoxication which describes this exact scenario in the setting of maternal water intoxication. The K-series describes three babies all whom developed seizures and had mild The case series describes three babies all whom developed seizures and had mild perinatal asphyxia yet went on to develop seizures. The laboratory results are shown below.
What is most remarkable from the table is the level of serum sodium in the newborns at 1 hour of age. Generally levels of sodium below 125 and certainly 120 can lead to neurological manifestations including seizures and these infants were certainly affected. Much like I explained at the outset of this piece children could be afflicted with a mild form of encephalopathy from hypoxia, and in these cases, each infant by 10 minutes of age had excellent Apgar scores. What I propose, though is that the brain after even a more mild degree of Perinatal asphyxia is more prone to neonatal seizures. I have to say over the years. I have often checked electrolytes after a baby presents with seizures and rarely are they sufficiently abnormal to explain the finding. What I am presenting to you. Here is a special circumstance, in which babies who might not otherwise have seizures, such as those with mild asphyxia go on to have significant convulsions due to the superimposed insult.
The goal of this post was to increase awareness of this phenomenon. Next time you are looking into the events leading up to seizures in a newborn, don’t forget to ask about what fluids a mother received during labour and specifically what her oral intake was like. Don’t forget to have a careful look as well at the amount of oxytocin she received during labour as the combination may be just enough to tip the scales and lied to Neonatal seizures in a baby, who otherwise would not have developed any of those manifestations! While you are at it, take the time to check a maternal sodium and if mother and baby match or at least are both hyponatremic to a similar level you likely have your answer as to what the ethology is.
A bigger question and one that we don’t have the answer to is whether in the presence of hyponatremia and mild asphyxia therapeutic hypothermia offers much benefit. Unfortunately this answer is going to be a tough one to come by as you can’t create an RCT since the numbers are so small but I suspect that most when in doubt will choose to get that temperature down!
When it comes to non-invasive ventilation the field has become a little more crowded in recent years at least in our institution. In the recent past if one decided to extubate an ELGAN the biggest decision was what CPAP pressure to use. These days we have the option of high frequency nasal ventilation (nHFOV) or non-invasive positive pressure ventilation (NIPPV) to choose from as additional options. Both of these modalities have their uses and I have written about nHFOV before as in Nasal High Frequency Oscillatory Ventilation For Preventing Intubation. On this post though I want to look at NIPPV which has actually been around longer as a modality. The gist of this mode is that one chooses a delta P, peep, Ti and rate much like you would on a conventional ventilator. When ventilating through a nasal interface the device provides ventilation although it is questionable I suppose how much of that is alveolar ventilation. The study we are going to talk about here caught my eye as the information gleaned from it gives me at least an idea of how this mode may work to help prevent reintubations.
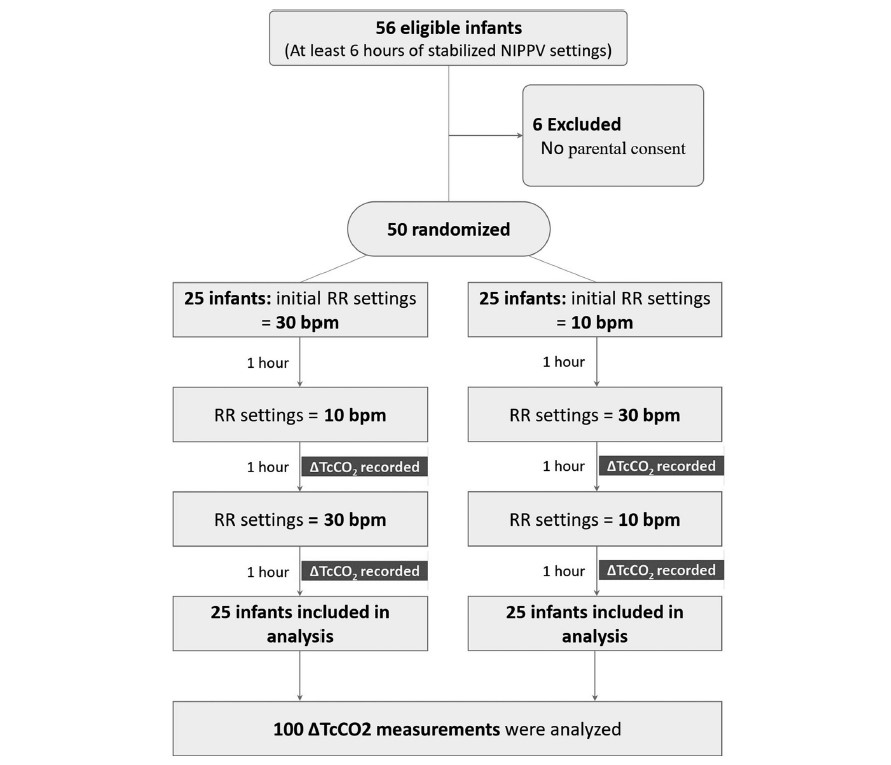
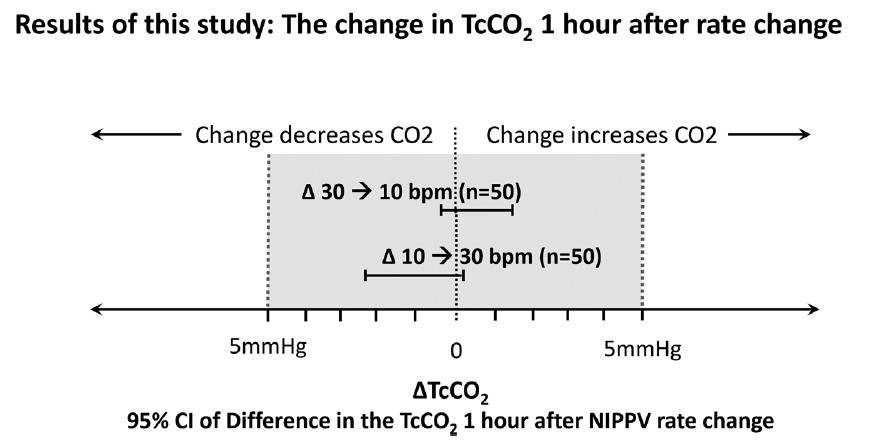
In this study each patient served as their own control and alternated between either a start of a rate of 10 BPM or a rate of 30 BPM as shown in the following diagram. The infants were all between 24 +0 and 32 +6 weeks gestation to be included in the study. Delivery of NIPPV was through the Leoni Ventilator using RAM cannulae and importantly the mode was non-synchronized. Each infant needed to be stable on their settings for at least 6 hours before being included. The authors hypothesis was that rate matters to clear carbon dioxide. To monitor CO2 levels they used transcutaneous CO2 measurements to allow for continuous measurement over each hour of the study. Given this belief, there was safety built into the protocol such that patients were excluded if on the set rate of 10 bpm the tcCO2-related pCO2 was <40 mmHg, or on NIPPV if the set rate of 30 bpm had a tcCO2-related-pCO2 is 60 mmHg, In other words, if rate matters and your tcCO2 was already less than 40 on a low rate then it would not be safe to blow off more CO2 and vice versa with high CO2 and low rates. To ensure that only rate affected the results “during the 3 h of the study no changes in PIP, PEEP or FiO2 were allowed with the following exceptions: if spO2 was <90% or >95% for more than 20 s, an increase or decrease in FiO2 were allowed to keep spO2 90–94%, and were documented”.
So does rate matter?
It turns out the authors found no difference in CO2 levels based on rate changes alone.
This of course is contrary to what the authors expected to find. The question is why this might be. What follows now is just speculation on my part but given the finding of no difference I can offer a few thoughts. The first is that NIPPV does not involve a distal delivery of gas like the situation of an endotracheal tube near the carina. With an endotracheal tube in place the delta P or pressure above the set peep is delivered to the gas exchanging areas of the lung. With NIPPV you are delivering the pressure at the nose and therefore there is a fair amount of dead space in between the exit of the gas into the baby and the lung. Might you just be really ventilating dead space for the most part?
Secondly, depending on the fit of the mask or the degree that the mouth was open how do we know how much of the non-invasive ventilation reached the infant? Lastly, in our own centre we have not been impressed with the RAM cannulae as we have found that whether the prongs are in or out of the nose the pressure being detected as being delivered seems to stay the same at least as the ventilator sees it. If the prongs were not in the nose properly and the atmosphere was being ventilated would one really know that the pressures weren’t really getting into the nose?
Lastly, the Leoni ventilator is not capable of delivering synchronized NIPPV. Now that there is the availability of synchronization on ventilators such as on the Puritan Bennett 980 ventilator it would be interesting to see the same study done again. If you are delivering non-synchronized breaths which are not in sync with the patient should we expect a change in CO2? What if half the breaths for example by chance are delivered on exhalation? Not much effect on CO2 I would think.
I am not saying that rate doesn’t matter at all but I suppose I am saying within the context of this study it doesn’t matter to CO2. My best guess as to how NIPPV works to prevent reintubation may be secondary to two things. The first would be by irritating the baby with the puffs of delta P. Think of it like intermittent stimulation. The second possibility is that the same puffs of air help keep the pharynx open and minimizes the obstructive portion of apnea of prematurity. Whatever the reason NIPPV appears to work to prevent reintubation in some infants!
I have no doubt the group here will look at the effect of delta P on CO2 soon enough and I wonder if we will see much difference there either. It also will be important to look at the effect of rate in a synchronized fashion! Time will tell.
Hypoxic ischemic encephalopathy is a very scary condition for both families and health care providers. In my career as a Neonatologist one of the greatest accomplishments has been the recognition that 72 hours of moderate hypothermia can make a big difference to the outcomes of such children. In days gone by our best estimates of outcome relied on Sarnat staging of HIE.
Since the cooling approach was adopted widely however I have relied more on a wait and see approach when advising families on what to expect. On some occasions, is spite of cooling babies go on to develop significant cerebral palsy but in other cases babies who one would have predicted would have dismal outcomes have done quite well. Our best estimates at the moment are that cooling for HIE reduces the risk of death or moderate to severe disability by about 25% with a confidence interval of 17 – 32% around that estimate.
Why would pCO2 matter?
Carbon dioxide has a role to play in outcome and has been the subject of several papers. The theoretical point is that very low carbon dioxide levels lead to vasoconstriction of blood vessels. When it comes to HIE one would be quite worried about vasoconstriction of blood vessels such as the carotids carrying oxygenated blood to an injured brain. Once injured the brain is not going to tolerate further oxygen deprivation and in particular those areas that are teetering on the edge of survival could be tipped the wrong way if further hypoxia is experienced.
Another reason why CO2 matters is due to something called the Bohr effect. For those of you who are scratching your heads and recollecting this term from your training it has to do with the influence of pCO2 on hemoglobin oxygen saturation. The relationship is represented by the following figure.
In the presence of declining pCO2 there is a shift of the oxygen dissociation curve to the left. This means for that as PCO2 declines more of the circulating oxygen will be bound to hemoglobin. In most cases you want your hemoglobin to be great at carrying oxygen but when your tissues are starved of oxygen and injured that is not what you want. You want a selfless hemoglobin molecule that is more than happy to release its oxygen to the tissue. That is not what you get as pCO2 drops.
Why would pCO2 be low at all?
There are a few reasons for this. The first is that many infants born after an asphyxial event have a metabolic acidosis. Our bodies naturally like to maintain a normal pH. In order to do so if your HCO3 in the blood is low you need to blow off CO2 to compensate. The hypocarbia in this case is compensatory but the body in so doing could make matters worse for the brain.
The second reason has to do with both injured tissue and that which is cooled. As metabolic rate decreases the amount of CO2 generated will drop. If you remember the Krebs cycle (shudder) there is a fair bit of CO2 generated from aerobic (oxygen rich) metabolism. If this is reduced so to will the production of CO2. As cooling serves to reduce metabolic rate so the CO2 production would be expected to decrease.
So does it really matter?
The reason for all this preamble is that a “mini-systematic review” has found the CO2 matters to outcome. The review is entitled Hypocarbia is associated with adverse outcomes in hypoxic ischaemic encephalopathy (HIE) and included 9 studies on influence of pCO2 on outcome. Before we look at the results it is important to acknowledge that all of the included studies were retrospective so methodology in each study is not standardized. How one even defines severe hypocarbia varied from <20 mmHg to anything under 35 mm Hg. The other issue is that each study looked at a different period of exposure from the effect of a couple hours to the effect over the first three days of life. The included infants were all cooled so it gives us at least an idea of the effect in a modern cohort of cooled infants.
The summary of the results was that CO2 mattered. As little as a couple hours of very low CO2 levels were found to be associated with adverse outcomes.
The problem of course is the chicken and the egg argument. The most severe hypocarbia might be seen in those with the worst metabolic acidosis. As mentioned above the response to metabolic acidosis is to blow off CO2. Therefore, the worse the metabolic acidosis the greater that respiratory drive.
Strategies to control the pCO2 of course exist. In the presence of a critically low pCO2 one can intubate and control ventilation through sedation and paralysis. This can lead to other issues though as if you normalize the pCO2 in the presence of a significant metabolic acidosis the pH is likely to take a nosedive. The myocardium as it turns out doesn’t like low pH and in fact cardiac output in animal models begins to decrease the closer you get to a pH of 7 and becomes significantly worse as you go beyond that point.
At best then I think one can aim for converting severe hypocarbia to moderate until the HCO3 begins to recover. Based on theoretical issues of oxygen delivery to tissues and cerebral vasoconstriction, notwithstanding the retrospective nature of this review it does make sense to me that there would be a link between severe hypocarbia and outcome. We will likely never see an RCT targeting normalization of pCO2 vs tolerance of hypocarbia in this population so for the purists out there that don’t like this type of retrospective analysis I suspect outside of an animal model this is as good as its going to get.
Maybe avoiding anything with the word severe attached to it though is sensible when it comes to this population.