As readers of this blog will know I am a big fan of anything that challenges my practice. It’s something that I think in general is a good practice to live by. For many years now when a preterm infant in particular is hypotensive it has been our practice to draw a serum cortisol level and then determine whether the stress response is adequate before starting hydrocortisone for blood pressure support. Having said that, sometimes we start the hydrocortisone and then use the level afterwards to determine if we need to continue. is this approach right though?
Evidence That Shakes Up Our Approach
It turns out the evidence that preterm infants may not be able to produce a robust cortisol response after birth has been around for sometime. In 1994 Hingre et al published Adrenal steroidogenesis in very low birth weight preterm infants. In this paper they documented the diminished ability of infants born < 30 weeks gestational age to produce cortisol finding preterm newborns had low basal cortisol levels “(mean +/- SEM, 207.4 +/- 23.5 nmol/L), and their levels were similar to basal levels reported for healthy full-term newborns (170.7 +/- 26.8 nmol/L; P = 0.31”. It is worth noting here that commonly held beliefs have been that an adequate adrenal response is in the range of 400 – 450 nmol/L or about 15 microgram/dL and these levels are lower than that. Moreover, when the authors measaured precursors of cortisol and found elevations consistent with a deficiency of decreased activity of 11 beta-hydroxylase (11 beta OH). Knowing this then, the use of a baseline cortisol to determine if an appropriate stress response is present before starting hydrocortisone is questionable. Having said that the practice has been that when it is low we assist with hydrocortisone and when it is high we can ease off the support. A new study that has just come out though I think may turn that thinking on its head!
High Cortisol Levels Are Concerning. Not the Lows!
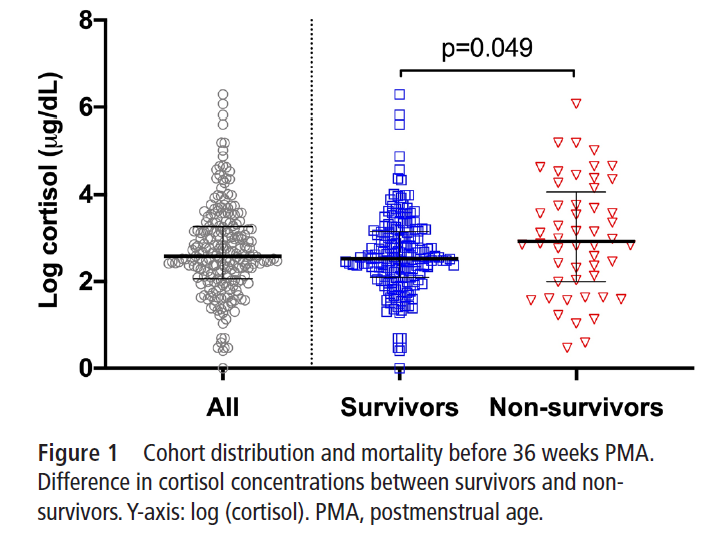
Absence of relationship between serum cortisol and critical illness in premature infants by Prelipcean I et al was just published and looked at 224 infants at the University of Florida who were born under 30 weeks and had baseline cortisol levels drawn for clinical indications prior to 36 weeks PMA. Like many centres the baseline cortisol was done prior to starting hydrocortisone for hypotension. A baseline level under 15 mcg/dL was considered low which equates to about 413 nmol/L for those using those units (like my own hospital). The Simplified Score for Neonatal Acute Physiology II SNAP-II score , neonatal Sequential Organ Failure Assessment (nSOFA) and Vasoactive-Inotrope Score (VIS) were calculated and used as measures of illness severity against the the cortisol levels obtained in a retrospective fashion. Cortisol levels were taken at a median of 3.8 days with an IQR of 1.2 to 14 days). Hydrocortisone was givne to 71% of patients in the study as well.
What emerged from these results might be counterintuitive. From the figure below it was found that those infants with higher baseline cortisol levels were less likely to survive. This result just reached statistical significance. Thinking about this for a moment, we have traditionally worried about the infants with low cortisol and rushed to supplement them. The babies at real risk though here are the ones with a robust pituitary adrenal axis response. Notably another factor that leads to lower cortisol levels in the first few days of life is provision of antenatal steroids so it may be at least in part that the higher baseline levels might be seen in those without the benefit of antenatal steroids and therefore are at higher risk of adverse outcome. Bottom line though, a robust cortisol level would not necessarily appear to be marker of a good thing.
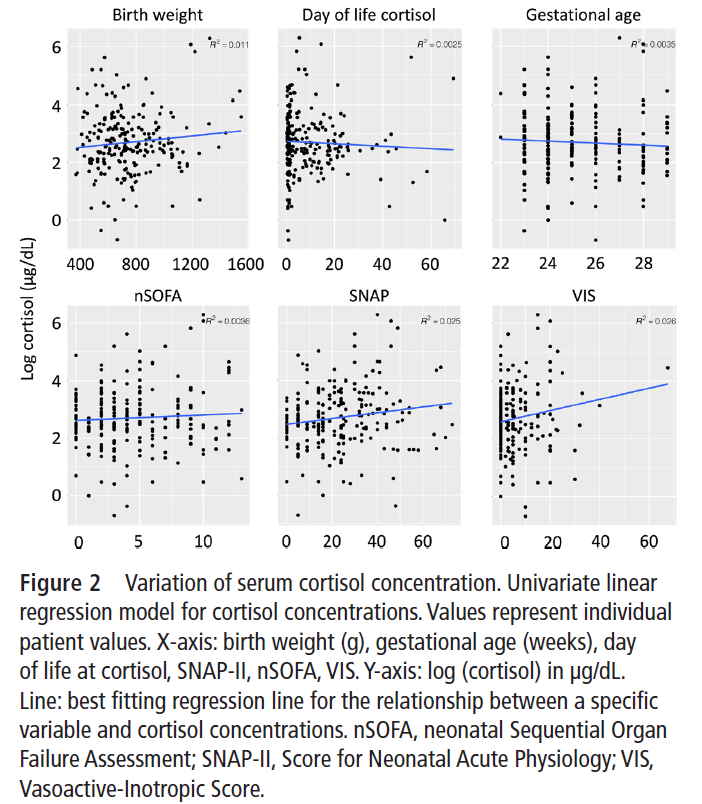
The second thing to be identified is the scatter of results for these infants across birth weight, day of life and gestational age. The authors discovered using a multivariable model that birth weight was the only statistically significant variable to explain cortisol variation. Interestingly for every 100g increase in birth weight cortisol increased an average of 10%.
Additionally, differences in average cortisol level were affected by chorioamnionitis and antenatal steroids. The presence of chorioamnionitis as a variable is not surprising I suppose given the results from the prophylactic steroid trials for BPD that have consistently found chorio predicts a higher rate of BPD.
Where things get really interesting is in the bottom half of the figure below. While weak linear associations with SNAP-II, nSOFA were found ,no correlation between serum cortisol concentration and concurrent critical illness severity objectively measured by SNAP-II and nSOFA scores at time points beyond the first day of life and prior to 36 weeks PMA in these infants were found. Most intriguing was the complete lack of relationship between the VIS and cortisol levels.
This presents a predicament about what to do with these levels. Based on this research the degree of illness and the amount of inotrope one is on (VIS takes into account doses of dopamine, dobutamine, vasopressin, milrinone, epinephrine and norepinephrine) has no relationship to cortisol level. If you are like our centre though you have been considering whether to use hydrocortisone based on the level of cortisol at baseline. Based on this research the message would be that if one wants to know a baseline cortisol it might be useful as a tool to determine how concerned one should be with an infant as risk of mortality is higher if baseline levels are above 413 nmol/L. In terms of determining whether one should support with hydrocortisone though in the face of a sick preterm infant and more specifically a hypotensive one the utility of the baseline measurement I would question. Adding to this the research from 1994 and one has to question if the level is low is that simply because the infant doesn’t have the metabolic machinery yet to produce enough rather than has an abnormal response to stress.
Some qualifiers as with any study like this need to be acknowledged. It is not a study of 1000 patients so the individual numbers of patients at different weight levels will be lower and therefore there could be unusual patients here influencing the results. Having said that, when you combine this information in this study with what is known from before about these preterm infants should we be surprised that there is no relationship between baseline cortisol and illness. If you don’t have the capacity to make it except when exceptionally stressed it would appear that all these baseline cortisols may in fact be good for telling ourselves how stressed we should be about the patient.
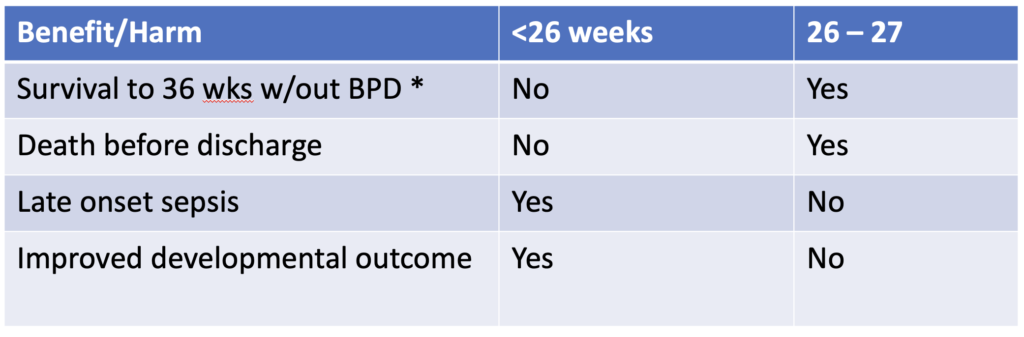
Precision medicine is a growing field in which genetic factors, environment, metabolism and even lifestyle are taken into account when deciding who should receive a treatment or not. When it comes to bronchopulmonary dysplasia I believe anyone who works in Neonatal care can attest it is a mystery why some infants go on to develop BPD while others don’t. We do know that certain treatment strategies may increase risk such as using excessive volumes or pressure to ventilate and in the last 25 years the notion that your level of cortisol in the blood may make a difference as well. I have written about prophylactic hydrocortisone use before in Hydrocortisone after birth may benefit the smallest preemies the most! When looking at the literature thus far and taking into account the results of the individual patient meta-analysis the following table can be generated highlighting a summary of benefits.
The question thus becomes if there is benefit for some infants under 26 weeks and then for some that are 26 and 27 weeks but there is also risk of harm, is there a way to select out those who are most likely to benefit with the least risk of harm.
A baby’s initial cortisol level may be the answer
The PREMILOC study was a double-blond multicentred trial of 523 infants randomly assigned to either prophylactic hydrocortisone in the first 24 hours of life or placebo. All infants were under 28 weeks at birth and received 1 mg/kg/d of hydrocortisone 1 mg/kg/d for 7 days followed by 3 days of 0.5 mg/kg/d for three days. In a pre-planned study coming out of the PREMILOC study, researchers looked at the role of baseline cortisol in predicting response to treatment or risk of adverse outcomes.
What they found in examining baseline levels for both treatment and placebo groups was that a relationship exists between the baseline level and such outcomes.
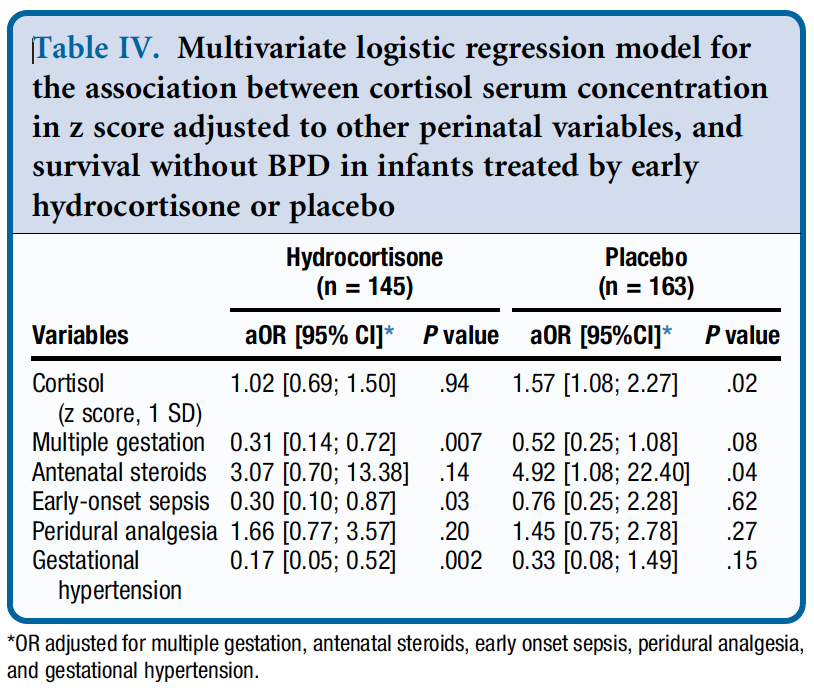
From Table 4 they found a relationship between survival without BPD and a higher initial level of cortisol but found no such relationship in the treatment arm. The threshold of what was considered high was 880 nmol/L although the mean cortisol was in the 400-500 nmol/L range. in other words, if having adequate physiologic levels of cortisol is the goal and a baby already has that, giving more non-antiinflammatory dosing of hydrocortisone doesn’t yield benefit.
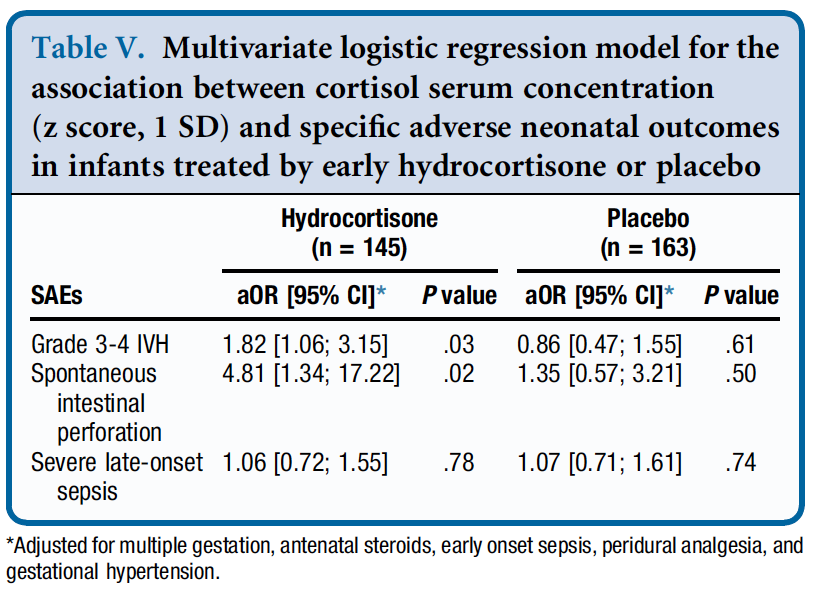
Similarly, when looking at side effects a positive correlation was found between higher baseline levels of cortisol and risk of grade III/IV IVH and spontaneous intestinal perforation. It would seem therefore that if a baby has the level of cortisol that they would normally have from a physiologic perspective they are no different than a placebo arm patient when given hydrocortisone as you bring them to where they need to be. When you double the dose however that they should have, side effects begin to rear their ugly head.
How can you use this information?
From personal conversations I know that many centres are struggling with what to do about giving hydrocortisone. On the one hand there isn’t much benefit (if at all) for BPD in the 24 and 25 week infants but they do better from a neurodevelopmental standpoint. On the other hand there is a benefit in the 26 and 27 week infants but you may predispose them to side effects as well.
This is where precision medicine comes in. One option for centers unsure of who to provide this to (if at all) could be to use a threshold of 880 nmol/L and if the initial level is above this you would not treat but if below offer treatment. This level while found in the study to be predictive of side effects in particular if high does seem very high to me. I would think most babies would qualify which is not necessarily a bad thing but in our center we have typically used levels above 400 or 500 as an adequate stress response. Regardless of the level picked one would be using physiologic data to determine who to give hydrocortisone to as a way to try and maximize benefit and minimize harm for the individual patient.
Make no mistake. Regardless of whether you decide to try this for your patients I don’t believe this is a magic bullet. The best chances for our patients come from having bundles of evidence based based practices and applying them to the patient population if we hope to reduce BPD and minimize risk from any side effects of our treatments. The question is whether prophylactic hydrocortisone should be part of this bundle.
I feel like this has been a story in the making for some time. Next to caffeine, the story of prophylactic hydrocortisone must be one of my more popular topics and has been covered more than once before as in A Shocking Change in Position. Postnatal steroids for ALL microprems or Early Hydrocortisone: Short term gain without long term pain. and the last post Hydrocortisone after birth may benefit the smallest preemies the most! After reporting on this topic about once a year, a recent paper may wrap it all up in a bow for the holidays and present to us the conclusion after all this work on the topic. I was extremely interested in this topic not just because I believe this therapy may have a future in the standard approach to neonatal care for VLBWs but because I have served on the CPS Fetus and Newborn committee with two of the authors of the paper. Dr. Lacaze and Dr. Watterberg have an exceptional understanding of this topic and so when they band together with other experts in the field I take notice.
An Individual Patient Data Meta-Analysis
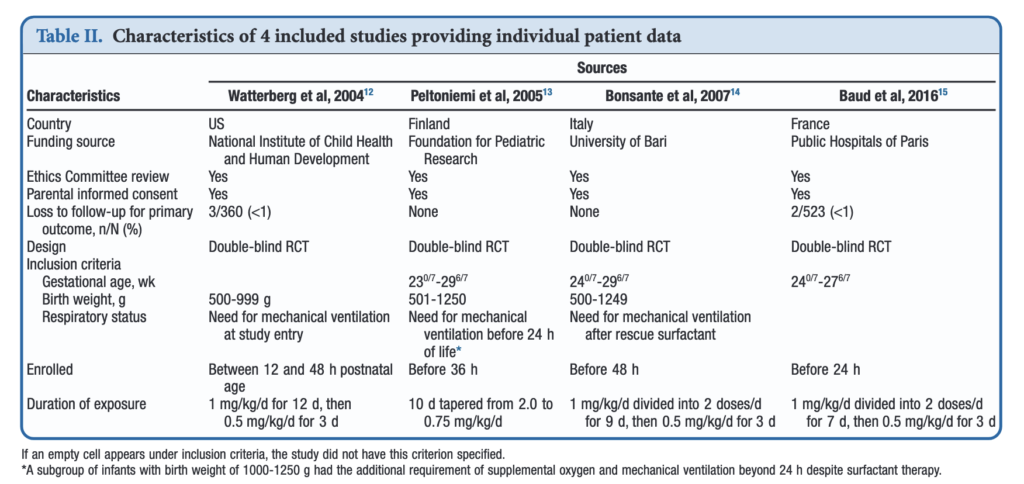
If you have read my previous posts then you know the story of why hydrocortisone given over the first 10-12 days of life might help those born before 30 weeks or < 1250g. In essence the concept is that it has been shown previously that many infants with relative adrenal insufficiency may go on to develop BPD. If you treat all such infants at risk you could theoretically reduce BPD. Typically after a few studies examining a similar topic come out, one can combine them in a meta-analysis using aggregate data (averages of effect sizes for the individual studies) and see what the larger sample shows. Another way to do it though is to go back to the original data and examine the infants at a more granular level allowing a greater identification and control of variables that might influence outcomes. This is what the authors led my Michele Shaffer did here in the paper Effect of Prophylaxis for Early Adrenal Insufficiency Using Low-Dose Hydrocortisone in Very Preterm Infants: An Individual Patient Data Meta-Analysis. There were a total of 5 studies on this topic but one study of 40 patients no longer had individual data so was excluded from analysis leaving 4 to look at. The details of the four studies are shown below. You can see that the inclusion criteria differed slightly but in general these were all infants up to 27 – 29 completed weeks and 500 – 1250g maximum who were treated with regimens as shown in the table.
What were the results?
Treatment with early low-dose hydrocortisone was associated with greater odds of survival without BPD at 36 weeks PMA after adjustment for sex, gestational age, and antenatal steroid use (aOR, 1.45; 95% CI, 1.11-1.90; I 2 = 0%). Also found were lower individual odds of BPD (aOR, 0.73; 95% CI, 0.54-0.98; I 2 = 0%), but not with a significant decrease in death before 36 weeks PMA (aOR, 0.76; 95% CI, 0.54-1.07; I 2 = 0%). Importantly although death by 36 weeks was not different, a decrease in death before discharge (aOR, 0.70; 95% CI, 0.51-0.97; I 2 = 0%) was found. Also noted and important was a reduction in medical treatment for PDA OR 0.72 (0.56-0.93)
All of these outcomes sound important but in a subgroup analysis other interesting findings emerged.
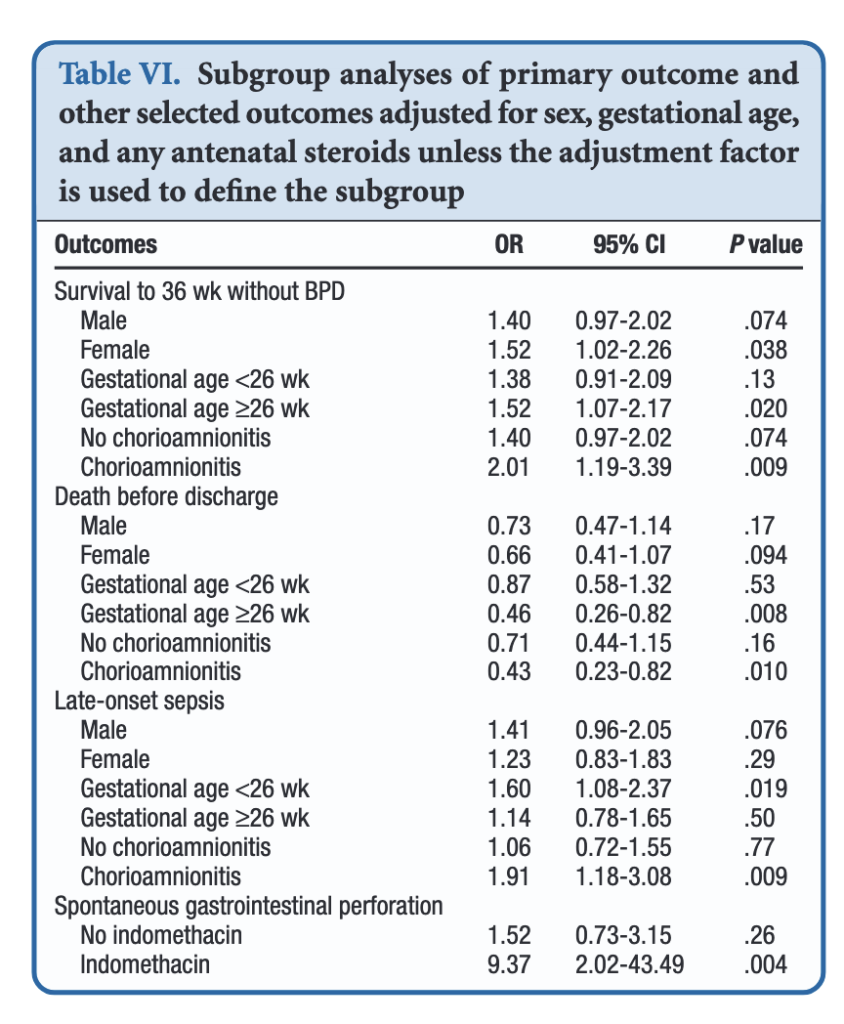
When dividing the patients into those less then 26 weeks and those at or greater than that gestational age, the benefits appear to be limited to those in the latter group. Levels of significance are high once you reach that GA suggesting that issues affecting those at younger gestational ages are less amenable to treatment. On the other hand one could say that the benefits seen at 26 – 29 weeks GA are relatively strong using a glass is half full approach. An important outcome worth noting is that while spontaneous intestinal perforation is noted to be a risk with prophylactic hydrocortisone, when you remove indomethacin from the equation the risk disappears. For those units using prophylactic hydrocortisone one would likely need to choose between the two but if you are like our unit where we don’t have that option this may be one strategy to consider.
In terms of risk to giving such therapy the big one noted in the paper was an increase in risk for late onset sepsis. Interestingly, this was limited though to the group under 26 weeks GA. In essence then the messaging would appear to be that under 26 weeks there may be less benefit to such treatment and therefore the increased risk of late onset sepsis without such benefits on BPD would suggest not using it in this GA group.
Where do we land then?
It would be easy to cast this aside I suppose as the group you are most worried about (22-25 weeks) doesn’t seem to really benefit but has a risk of late onset sepsis. That leaves us though with the group from 26-29 weeks. They do seem to benefit and may do so to a significant degree. They do develop BPD and to be honest we don’t have much outside of trying our best to use gentle ventilation to ameliorate their course in hospital. It is worth noting that the one group that does seem to show the greatest benefit are those exposed to chorioamnionitis. It is this group in particular that may be the best target for this intervention and I gather this has been discussed at a recent EPIQ meeting.
If one says no to trying this approach then the question that needs to be asked is whether doing nothing for this group is better than supporting them with hydrocortisone? If your centre’s rates of BPD are top notch then maybe you don’t want to add something in. If not though maybe it is time to rock the boat and try something different.
In our journey as Neonatologists and interdisciplinary teams we are forever seeking to rid or at least reduce the plague of BPD in the patients we care for. The PREMILOC trial was a double-blind, multicenter, randomized, placebo-controlled trial designed to test just that concept by introducing a low dose of hydrocortisone within 24 hours of birth. They enrolled infants born between 24 – 26+6 weeks of gestation and assigned them to receive either placebo or low-dose hydrocortisone 0.5mg/kg twice per day for 7 days, followed by 0.5 mg/kg per day for 3 days. The trial has been the subject of a previous post A Shocking Change in Position. Postnatal steroids for ALL microprems? Although the trial was stopped early due to financial concerns the authors demonstrated a 9% reduction in BPD using this strategy. The theory here in part is that the presence of hydrocortisone reduces inflammation and that this in turn may allow for better growth of lungs with time.
Why Not Adopt The Results Based on These Fantastic Results?
Steroids in preterm infants have a bad name. As discussed in previous posts on the topic the concern in all trials has been the potential impact of such medications on the developing brain. A nice summary of these concerns can be found in a paper in the CMAJ by the other “Canadian Neonatal Blogger” from 2001 in which he quoted the risk of cerebral palsy increasing from about 1 in 6 babies to 1 in 3 if babies born at < 28 weeks were exposed to postnatal steroids. Neurodevelopmental impairment overall would change from 1 in 4 to 1 in 3 if such exposure occurred. This paper and others expressing concerns over the effect of postnatal steroids led to a change in practice from more ubiquitous use to one restrained to only in those cases where the patient was nearing the end of all other options. This meant holding out for such therapy until such patients were at 90% or more O2 and on high mean airway pressures. Although not formally studied I was very concerned at the time with using this approach as I felt it was a “fait de complet” that they would either die or have significant developmental impairment should they survive due to the complications of having such severe BPD. It is critical to note though that the outcomes from these long term studies were in infants exposed to much longer courses of dexamethasone and at high doses that are used today.
Over the years with the development of the DART protocol and other more gentle approaches to steroids we as a group relaxed and certainly rescue courses of lower dose steroids have crept into practice when patients seem to be “stuck” on the ventilator.
Drumroll Please…
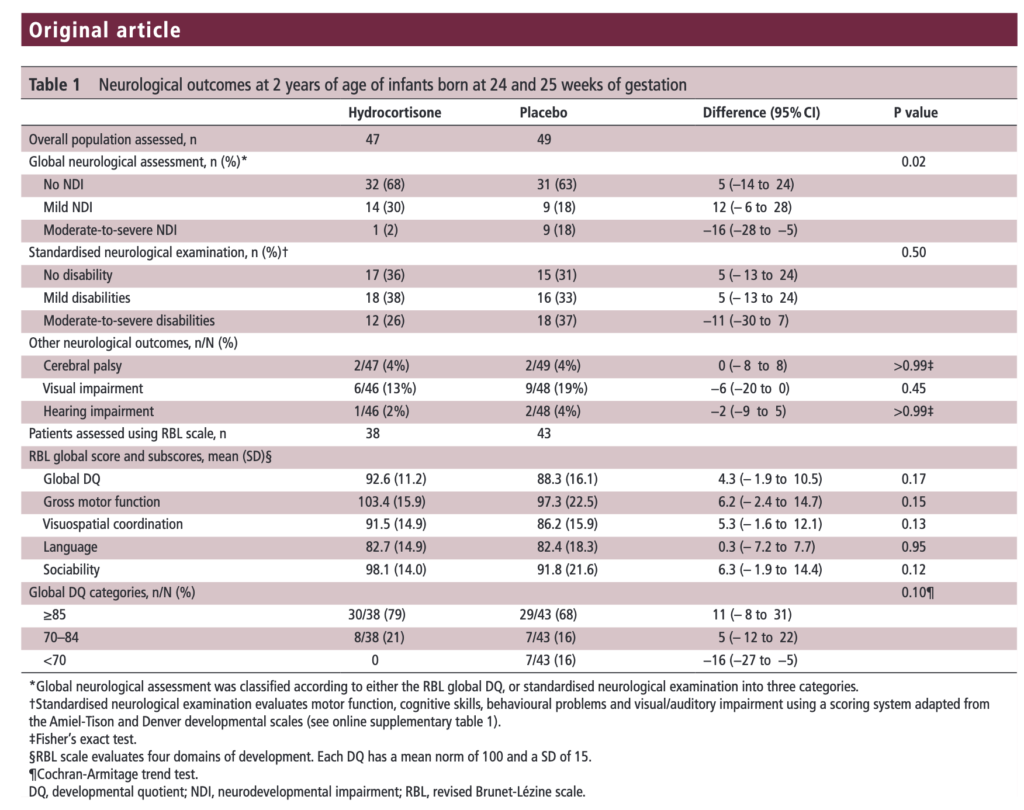
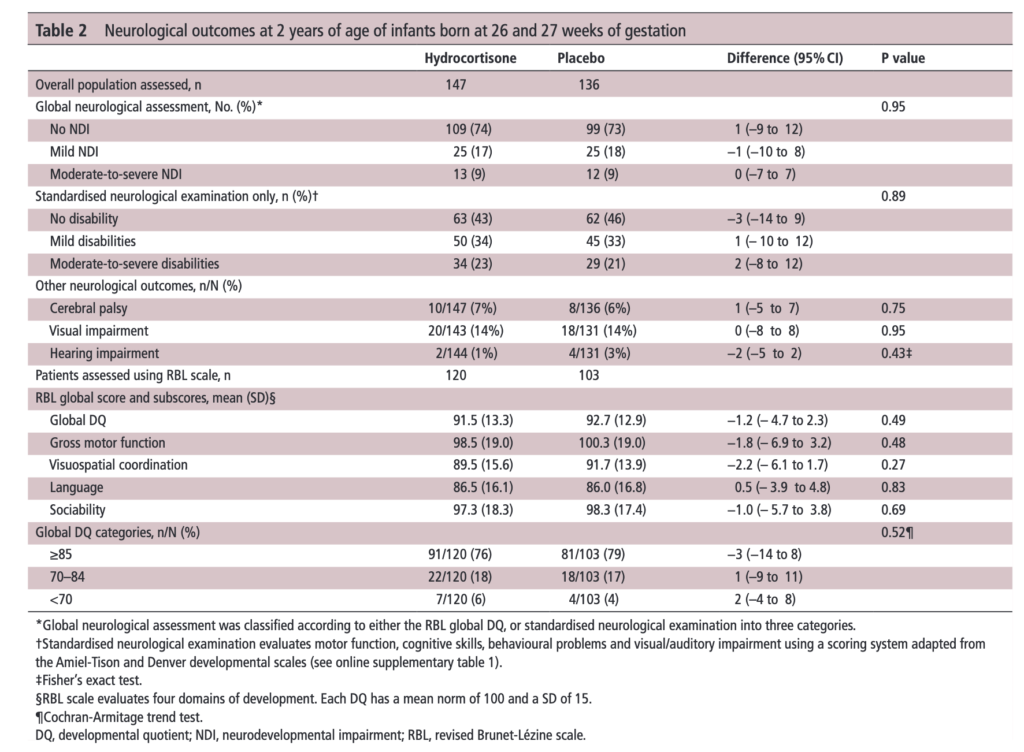
The results of the PREMILOC follow-up study are now here and in short they look good. Patients were followed up at an average age of 22 months and included a medical history, anthropometric measures, respiratory status, standardized neurological examination based on specific definitions of disabilities, and quantitative neurodevelopmental assessment using the revised Brunet-L.zine (RBL) scale. Follow-up was 93% in the hydrocortisone and 90% in the placebo arm which is important as we need not worry about the missed patients influencing the results to a significant degree if they had been included. Although some post-hoc analyses were done what I am most interested in is the primary outcome which is shown below.
There was no difference in either neurodevelopment overall or any of the subcategories. This provides a great deal of reassurance to those who provide steroids this way. There will be those however that argue the study is too small. While a larger study might be better able to address whether there is a small difference in outcome I don’t think we will see one anytime soon. It is one of the challenges we face in Neonatology. Unlike the adult world with studies of thousands of patients, due to the small number of patients born at <28 weeks it is always a challenge to recruit into such large volume trials. We can compare trials by doing meta analyses or systematic reviews and perhaps that is where we will head with this study although given that different steroids will have been used (thinking dexamethasone as in the DART study) this will always be left open to question.
Is it worth it?
I suppose the real question here is the following for a parent to consider. “Would you like your baby to receive hydrocortisone shortly after birth with a 7% reduction in the risk of BPD at 36 weeks bearing in mind that although we don’t think there is an impact on long term development we aren’t certain yet”.
I guess to answer this question you need to think about the first part of the question. Is BPD at 36 weeks a good outcome to look at for benefit? The Canadian Neonatal Network has recently called for a rethink on this The New BPD That Matters. It turns out that it is 40 weeks and not 36 weeks that has the greatest prediction for respiratory morbidity after discharge. If you were to move the goal post to 40 weeks from 36 I strongly suspect one would see the 9% reduction in BPD as shown in the PREMILOC trial vanish. If that is the case, would a slightly earlier extubation time be enough to motivate families to take the plunge?
Although I often cringe at the expression “more trials are needed”, I think at least a combination of studies to achieve greater confidence in outcome may be needed. Barring that, we might just have to sit tight and accept that while there may be a little bit to be gained with the use of the PREMILOC protocol it may just not be enough to be clinically warranted at this time. May want to wait for the next big thing to tackle BPD…





 There was no difference in either neurodevelopment overall or any of the subcategories. This provides a great deal of reassurance to those who provide steroids this way. There will be those however that argue the study is too small. While a larger study might be better able to address whether there is a small difference in outcome I don’t think we will see one anytime soon. It is one of the challenges we face in Neonatology. Unlike the adult world with studies of thousands of patients, due to the small number of patients born at <28 weeks it is always a challenge to recruit into such large volume trials. We can compare trials by doing meta analyses or systematic reviews and perhaps that is where we will head with this study although given that different steroids will have been used (thinking dexamethasone as in the DART study) this will always be left open to question.
There was no difference in either neurodevelopment overall or any of the subcategories. This provides a great deal of reassurance to those who provide steroids this way. There will be those however that argue the study is too small. While a larger study might be better able to address whether there is a small difference in outcome I don’t think we will see one anytime soon. It is one of the challenges we face in Neonatology. Unlike the adult world with studies of thousands of patients, due to the small number of patients born at <28 weeks it is always a challenge to recruit into such large volume trials. We can compare trials by doing meta analyses or systematic reviews and perhaps that is where we will head with this study although given that different steroids will have been used (thinking dexamethasone as in the DART study) this will always be left open to question.