

This is becoming “all the rage” as they say. I first heard about the strategy of feeding while on CPAP from colleagues in Calgary. They had created the SINC * (Safe Individualized Feeding Competence) program to provide an approach to safely introducing feeding to those who were still requiring CPAP. As news of this approach spread a great deal of excitement ensued as one can only imagine that in these days when attainment of oral feeding is a common reason for delaying discharge, could getting an early start shorten hospital stay? I could describe what they found with the implementation of this strategy but I couldn’t do it the same justice as the presenter of the data did at a recent conference in Winnipeg. For the slide set you can find them here. As you can imagine, in this experience out of Calgary though they did indeed find that wonderful accomplishment of shorter hospital stays in the SINC group. We have been so impressed with the results and the sensibility of it all that we in fact have embraced the concept and introduced it here in both of our units. The protocol for providing this approach is the following.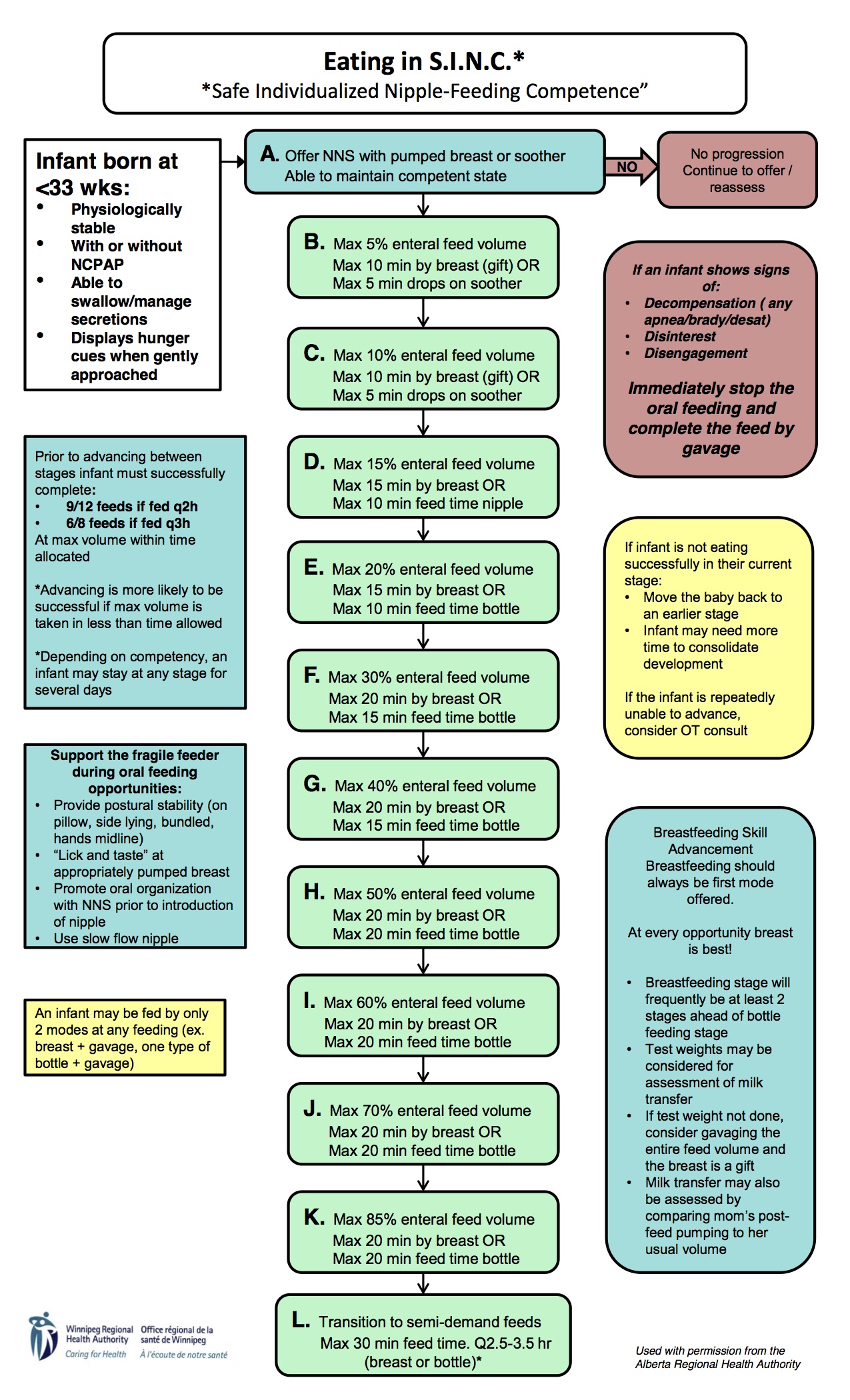
I have to admit, while I have only experienced this approach for a short time the results do seem to be impressive. Although anecdotal a parent even commented the other day that she felt that SINC was instrumental in getting her baby’s feeding going! With all this excitement around this technique I was thrown a little off kilter when a paper came out suggesting we should put a full stop to feeding on CPAP!
Effect of nasal continuous positive airway pressure on the pharyngeal swallow in neonates
What caused my spirits to dampen? This study enrolled preterm infants who were still on CPAP at ≥ 34 weeks PMA and were taking over 50% of required feeding volumes by NG feeding. The goal was to look at 15 patients who were being fed on CPAP +5 and with a mean FiO2 of 25% (21-37%) using video fluoroscopic swallowing studies to determine whether such patients aspirate when being fed. The researchers became concerned when each of the first seven patients demonstrated abnormalities of swallowing function indicating varying degrees of aspiration. As such they took each patient off CPAP in the radiology suite and replaced it with 1 l/min NP to achieve acceptable oxygen saturations and repeated the study again. The results of the two swallow studies showed remarkable differences in risk to the patient and as such the recruitment of further patients was stopped due to concerns of safety and a firm recommendation of avoiding feeding while on CPAP was made.
| Table 2. Percentage of all swallows identified with swallowing dysfunction | |||||
| on-nCPAP | off-nCPAP | ||||
| Variable Mean ± s.d. | Mean ± s.d. | Median (q1–q3) | Mean ± s.d. | Median (q1–q3) | P-value |
| Mild pen. % | 20.1±16 | 20 (4.5–35) | 15.4± 7.6 | 20 (9–20) | 0.656 |
| Deep pen. % | 43.7±15.4 | 38.5 (30–59) | 25.3± 8.8 | 25 (18.2–32) | 0.031 |
| Aspiration % | 33.5±9.4 | 30 (27.3–44.4) | 14.6± 7 | 15 (9.1–20) | 0.016 |
| Nasopharyngeal reflux % | 42.8±48.5 | 18.2 (0–100) | 44.2± 45.4 | 18.2 (5–92) | 0.875 |
Taking these results at face value it would seem that we should put an abrupt halt to feeding while on CPAP but as the saying goes the devil is in the details…
CPAP Using Ram Cannulae
Let me start off by saying that I don’t have any particular fight to pick with the RAM cannulae. They serve a purpose and that is they allow CPAP to be delivered with a very simple set of prongs and avoid the hats, straps and such of more traditional CPAP devices. We have used them as temporary CPAP delivery when moving a patient from one area to another. As the authors state the prongs are sized in order to ensure the presence of a leak. This has to do with the need to provide a way for the patient to exhale when nasal breathing. Prongs that are too loose have a large leak and may not deliver adequate pressure while those that are too tight may inadvertently deliver high pressure and therefore impose significant work of breathing on the patient. Even with appropriate sizing these prongs do not allow one to exhale against a low pressure or flow as is seen with the “fluidic flip” employed with the infant flow interface. With the fluidic flip, exhalation occurs against very little resistance thereby reducing work of breathing which is not present with the use of the RAM cannula.
A comparison of the often used “bubble CPAP” to a variable flow device also showed lower work of breathing when variable flow is used.
The Bottom Line
Trying to feed an infant who is working against a constant flow as delivered by the RAM cannulae is bound to cause problems. I don’t think it should be a surprise to find that trying to feed while struggling to breathe increases the risk of aspiration. Similarly, under treating a patient by placing them on nasal prongs would lead to increased work of breathing as while you may provide the needed O2 it is at lower lung volumes. Increasing work of breathing places infants at increased risk of aspiration. That is what I would take from this study. Interestingly, looking at the slide set from Calgary they did in fact use CPAP with the fluidic flip. Smart people they are. It would be too easy to embrace the results of this study and turn your nose to the SINC approach to feeding on CPAP. Perhaps somewhere out there someone will read this and think twice about abandoning the SINC approach and a baby will be better for it.
* SINC algorithm and picture of the fluidic flip courtesy of Stacey Dalgleish and the continued work of Alberta Health Services
Hello, thanks for writing this article. Are you able to share the name of the study that you mention in which they stopped recruiting patients because of safety concerns? thanks! Arielle
J Perinatol
. 2017 Apr;37(4):398-403. doi: 10.1038/jp.2016.229. Epub 2017 Jan 5.
Effect of Nasal Continuous Positive Airway Pressure on the Pharyngeal Swallow in Neonates
L Ferrara 1, A Bidiwala 2, I Sher 3, M Pirzada 4, D Barlev 3, S Islam 5, W Rosenfeld 6, C C Crowley 7, N Hanna 8
Affiliations expand
PMID: 28055023 DOI: 10.1038/jp.2016.229
Abstract
Objective: Feeding neonates orally while on nasal continuous positive airway pressure (nCPAP) is a common practice. We hypothesize that pressurized airflow provided by nCPAP will alter the swallowing mechanism in neonates, increasing the risk of aspiration during oral feeding.
Study design: Infants receiving nCPAP with a RAM cannula and tolerating at least 50% of their feeding orally were included in the study (one term; six preterm infants). Each participant underwent a videofluoroscopic swallow study while on nCPAP and off nCPAP. A non-parametric signed-rank test was used for paired data.
Result: The incidence of deep penetration (P=0.03) and aspiration (P=0.01) decreased significantly off-nCPAP compared with on-nCPAP. However, the incidence of mild penetration (P=0.65) and nasopharyngeal reflux (P=0.87) remained the same under both conditions.
Conclusion: Oral feeding while on-nCPAP significantly increases the risk of laryngeal penetration and tracheal aspiration events. We recommend caution when initiating oral feedings on nCPAP.
Similar articles
Swallowing function and medical diagnoses in infants suspected of Dysphagia.
Newman LA, Keckley C, Petersen MC, Hamner A.
Pediatrics. 2001 Dec;108(6):E106. doi: 10.1542/peds.108.6.e106.
PMID: 11731633
Absence of effect of nasal continuous positive airway pressure on the esophageal phase of nutritive swallowing in newborn lambs.
Djeddi D, Cantin D, Samson N, Tian H, Praud JP.
J Pediatr Gastroenterol Nutr. 2013 Aug;57(2):188-91. doi: 10.1097/MPG.0b013e318292b3b2.
PMID: 23535760
Effects of nasal continuous positive-airway pressure on nutritive swallowing in lambs.
Bernier A, Catelin C, Ahmed MA, Samson N, Bonneau P, Praud JP.
J Appl Physiol (1985). 2012 Jun;112(12):1984-91. doi: 10.1152/japplphysiol.01559.2011. Epub 2012 Apr 12.
PMID: 22500003
An integrative review of skin breakdown in the preterm infant associated with nasal continuous positive airway pressure.
Newnam KM, McGrath JM, Estes T, Jallo N, Salyer J, Bass WT.
J Obstet Gynecol Neonatal Nurs. 2013 Sep-Oct;42(5):508-16. doi: 10.1111/1552-6909.12233. Epub 2013 Sep 4.
PMID: 24020476 Review.
Nasal intermittent positive pressure ventilation (NIPPV) versus nasal continuous positive airway pressure (NCPAP) for preterm neonates after extubation.
Lemyre B, Davis PG, De Paoli AG, Kirpalani H.