I couldn’t think of a better topic for World Prematurity Day 2021 than what constitutes the edge of viability. Thinking back over my career, when I was a resident and fellow infants born at 25 and 26 weeks were deemed about as low as “we should” go but we certainly resuscitated infants at 24 weeks but this was considered heroic. Jump ahead to the last decade and we began caring for infants at birth at 23 weeks so commonly that the thought of offering comfort care only to infants at 24 weeks became almost unthinkable for many health care providers. Before I get jumped on, let me say that I am not saying I agree or disagree with that sentiment but it is something that is felt by many.
The Shared Decision Model
In the last few years a rethink again has occurred whereby the concept of the treating team knowing best has been replaced by the “shared decision model”. In this line of thinking, it is not up to us as health care providers to “tell the parents” what to do but rather come to a shared decision based on an assessment of the wishes and values of the parents in conjunction with hearing about both short and long term problems their infants may face if resuscitated. This concept was central to the statement by the Canadian Pediatric Society that I am proud to have been part of with respect to its development. The statement for those that are interested is Counselling and management for anticipated extremely preterm birth
What’s next? Going below 22 weeks?
The challenge of the shared decision model is that there comes a point where the answer is simply “no”. If for example a family at 19 weeks gestation demanded an attempt at resuscitation I would have to inform them that survival is not possible (assuming ultrasound confirmed anthropometric measurements consistent with that age). The question though becomes a little more difficult to answer at 21 weeks and was the subject of a recent article in the New York Times about a survivor at 21 weeks gestation.
Even with the best gestational age dating the estimate can be off by up to 5 days so it’s possible that the infant in this story was closer to 22 weeks or even midpoint between 22 and 23 weeks in reality. Regardless it does raise the question about what to do at 21 weeks and I suspect we will begin to see more stories about this now that the glass ceiling of 22 weeks has been breached. What about below 21 weeks? Sounds impossible I know but with research that remains at the stage of animal studies this may become possible. Maybe not in the next 5-10 years but it could happen in my lifetime in this chosen field.
The Artificial Placenta
This made headlines a few years ago with the news that the Children’s Hospital of Philadelphia had successfully kept a lamb alive for a period of 4 weeks using an artificial placenta and amniotic fluid.
You might think that this was a one-off experiment that will never see the light of day but similar work is being done in Toronto, Canada where they have been able to do similar work with preterm piglets in their paper Achieving sustained extrauterine life: Challenges of an artificial placenta in fetal pigs as a model of the preterm human fetus. Incidentally as my colleague Dr. Ayman Sheta worked on this project while in Toronto I am particularly pleased to share this research. Similar to the experience in CHOP the team in Toronto has been able to keep piglets alive for progressively longer durations. My understanding is that despite the best efforts infectious complications over arise limiting how long one can sustain such animals.
This leads me to my final thoughts on where we might be able to go. I see a future where we apply such technology to humans but not in the way that people might have thought. Keeping a fetus after delivery at 21 or 20 weeks on an artificial placenta for many weeks is not likely a realistic goal. What if we could get 1 or 2 weeks though and allow the fetus to be oxygenated without using positive pressure on their developing lungs and transition them at 23 or 24 weeks gestation? We may in this way be able to allow for postnatal maturation in a artificial uterine environment and give babies a chance who would otherwise never had the opportunity for a shared decision with medical staff.
Sound like science fiction? Well the beauty of the internet as my friend told me today is that once it’s out there it out there for good. Let’s see how this post stands the test of time and to all the babies out there in NICUs and to their families I wish you all a good and uneventful World Prematurity Day wherever you may be!
I spend a bit of time on social media and when I do I come across the argument that vaccines aren’t needed in pregnancy if you have already had COVID. The concept from the vaccine hesitant is based on the notion of trying to avoid any perceived risk of vaccination when the body is already making antibodies against the virus. The literature has been fairly scant on newborns in terms of protective antibodies and limited to case reports/series that I have shared from time to time on either twitter or facebook. As you might expect something might have changed as I am writing a piece on this topic again. The change is related to a recent paper entitled Titers of SARS CoV-2 antibodies in cord blood of neonates whose mothers contracted SARS CoV-2 (COVID-19) during pregnancy and in those whose mothers were vaccinated with mRNA to SARS CoV-2 during pregnancy by Kashani-Legumsky et al in J Perinatol.
Setting The Stage
Before getting in to what they did it is important to understand how the mRNA vaccines work as the antibodies that one can look at in mothers and babies are of two types. The mRNA vaccines instruct the body to make anti-bodies against the spike protein (S antibodies) which forms the basis of how the vaccine helps our bodies identify the virus and then destroy it. For those who have actually been exposed to the virus and are not vaccinated, they develop a second antibody to the nucelocapsid protein (N antibody) which is within the viral core so this type will only be present in people who have been infected with the virus and their immune systems have dealt with it on their own. This is an important distinction as it allows you to create pure samples of people who have had the virus as a true infection and those who have been vaccinated and finally those who are neither.
Comparing Three Groups
So the authors here decided to compare three groups of women. Eighty three cord blood samples were divided into three groups (from the paper quoted) based on IgG antibody titres.
Group 1 included 29 samples (37%) from women who were infected with SARS-CoV-2 during pregnancy. Twelve had RT-PCR confirmed Covid-19 infection: three were infected in the first trimester, three in the second trimester and six in the third trimester. The other 17 had no clinical signs of SARS-CoV-2 infection during pregnancy and had a positive serologic test on admission. None of the 17 women had active SARS-CoV-2 infection at the time of delivery. Group 2 included 29 samples (37%) from women who were vaccinated against SARS-CoV-2 in the 3rd trimester.
Group 3 included 21 women (34%) and served as controls.
Looking at antibody levels in Group 1&2, 100% were positive for S antibodies. Interestingly, in group 1, 4 women did not test positive for the N antibody (3 were asymptomatic and one infected in the 1st trimester). In group 3 none of the women tested positive for any antibodies confirming they were neither vaccinated or had the infection previously.
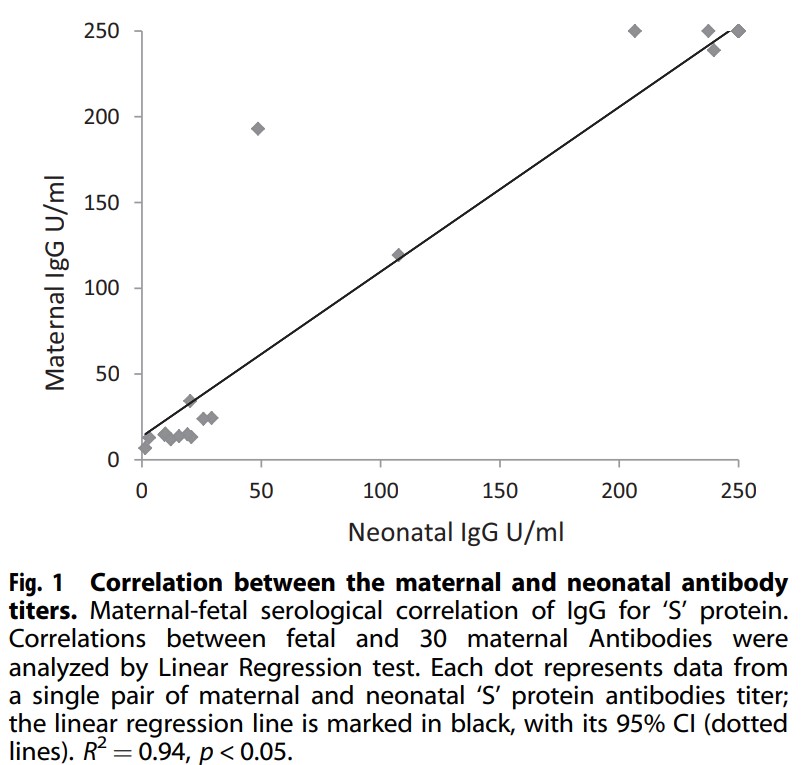
Looking at mean antibody S titres there was a significant difference found in that Group 1 had a mean of 83.7 U/mL vs 225.5 U/mL for the newborns whose mothers were vaccinated. Also notable was the relationship (not surprisingly between antibody levels in the mother at the time of delivery and newborn cord blood titres.
There was a linear correlation between the level in the mother and the level found in the newborn with higher levels presumably better for protecting the infant. Having said that, no infants in this study had neonatal COVID infection. Detractors would be quick to point out that this indicates it doesn’t matter if you get the vaccine since all babies were ok but remember although this may be the biggest study looking at antibodies in cord blood it remains a very small sample and neonatal infection although reported, remains a very rare occurrence.
The Other Side
If you have followed my coverage of the COVID saga from the start you would know that I am in favour of vaccination and in pregnancy as well. The results of this study are encouraging but we need to compare apples to apples. This study compared women who were vaccinated in the 3rd trimester to women who were infected at earlier time points and may have been sick or asymptomatic. The lower antibody levels found in group 1 could represent declining titres as the infection becomes more remote. What we also don’t know is what they antibody levels would have looked like in group 2 if the mothers were vaccinated in the 1st or 2nd trimester as this is now happening. Would the levels be similar? They just might be as the antibody levels do decline with time. We rely on memory cells to reactivate our antibody producing cells if the virus comes along again.
I am not saying this study is meaningless but be prepared if you quote this study for vaccine hesitant to point out that you are comparing recent vaccination to potentially mild cases or remote infections. What is clear and hopeful though is that your newborn is protected by antibodies you make in pregnancy from vaccination at very good levels and until we can vaccinate babies this is the greatest protection we can offer.
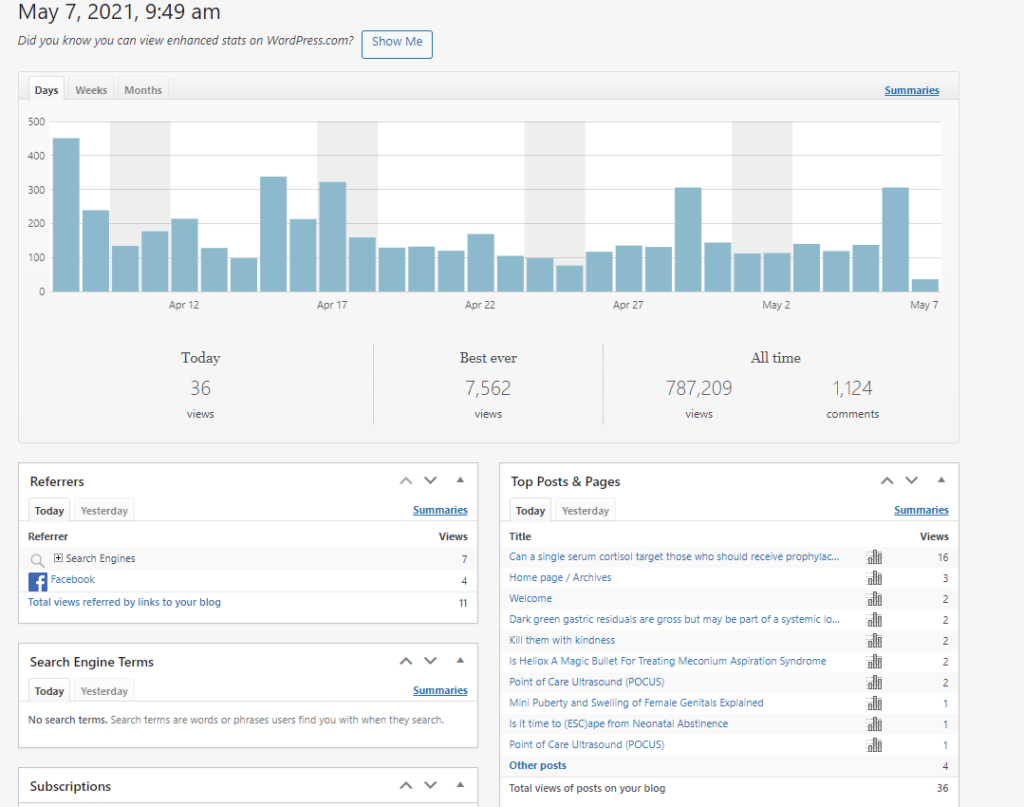
In medicine we learn a lot through feedback from our learners. The same prinicple I think can apply here on this blog. When I post a new blog post there are a few ways that it is shared. If you subscribe to this blog then you get a direct email about it. Others see the posts advertised on Facebook and Twitter or Linkedin and access the content from there. When you come through the latter route I am able to see that data and get a sense of whether a topic is of more or less interest to the readers as wordpress provides helpful statistics in this regard such as this from today.
When you access the post by reading the email version this view is not counted in the statistics. As of today there are 1745 of you registered to receive emails with each new post! What I am looking for today is for you to take this very quick poll and help me better understand where views are coming from.
My goal on the blog of course is to try and find interesting concepts and studies to share with you and it would be very helpful to know in particular about email readership.
Thanks in advance and I hope you continue to enjoy the content!
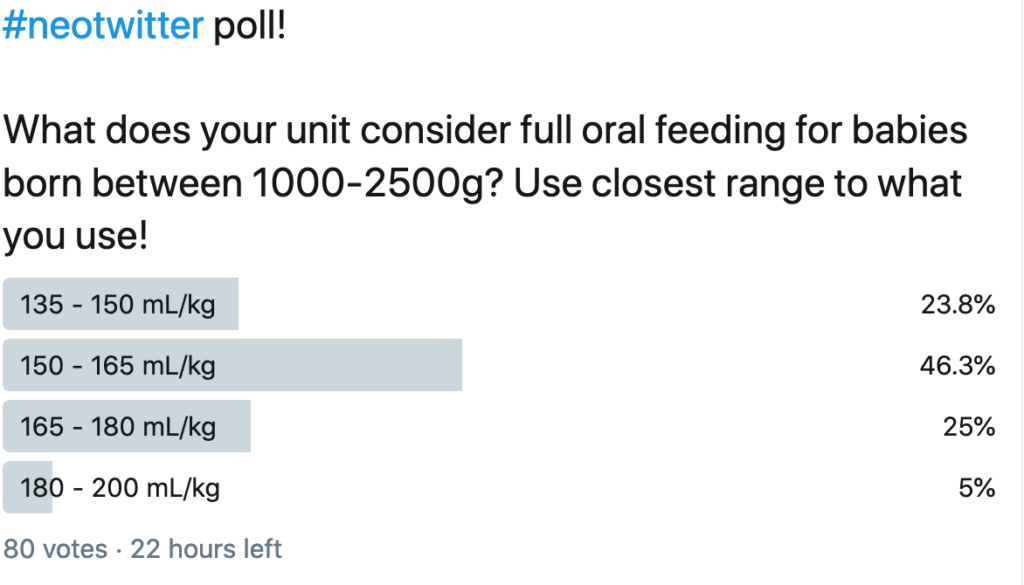
Since the dawn of my time in Neonatology there has been cibophobia! What is this you ask? It is the fear of food and with some flexibility in the definition I would apply this to large volumes of milk rather than the fear of food itself. Most units in the world seem to use a volume range of about 135 – 165 mL/kg/d as a range considered to mean “at full feeds”. As I was discussing this on rounds today I was quick to point out though that babies with neonatal opioid withdrawal syndrome (NOWS) frequently take in excess of 200 mL/kg/d and we don’t worry about it. The counter argument though is that these infants are “bigger” and should be able to tolerate a larger volume. As readers of this blog know I truly enjoy coming across papers that suggest a change to something considered dogma. Today is one of those days as I am choosing to explore in more depth an abstract that I posted to Twitter and Facebook last month.
On the day of this blog release I also took a poll on Twitter and found some interesting results that make this post all the more important to share. Take a look!
Are Bigger Volumes Better?
Travers CP et al chose to challenge this long held practice in their recent paper Higher or Usual Volume Feedings in Very Preterm Infants: A Randomized Clinical Trial. It was a simple yet wonderful trial that asked the question of whether for infants < 32 weeks GA at birth with BW from 1000-2500g would higher volume feedings of 180-200 vs 140-160 ml/kg/d help increase growth velocity. Randomization occurred after infants had reached 120 mL/kg/d of oral feedings. In both arms advancements from this point were the same and fortification occurrred as per usual practrice but in each arm strategies targeted individual fortification to weight gain.
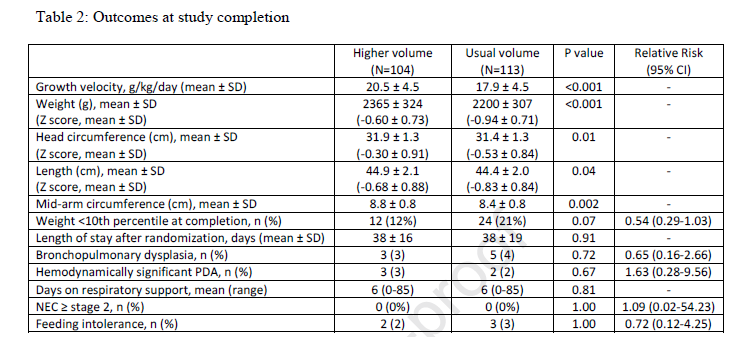
The authors were seeking a 3 g/kg/d difference in growth and needed 224 infants to demonstrate this difference. They enrolled the same at a mean GA of 30.5 weeks and a BW of 1445 grams. Birth characteristics including gestational age, weight, sex, race/ethnicity, Apgar scores, head circumference, length, and proportion of infants with a weight <10th percentile at birth did not differ between groups.
The outcomes showed differences as shown below.
Looking at the results
All in all I would say the results are a smashing success. Growth velocity was improved and not just in weight but in head circumference and length. What I find interesting is that if fortification of milk was targeted regardless of the volume used I am a bit baffled as to why the growth rate would still be better but it was. The difference in caloric intake received between groups was approximately 9 kcal/kg/day at day 7 after study entry (126 kcal/kg/day versus 117 kcal/kg/day) and 16 kcal/kg/day from day 14 after study entry onwards (139 kcal/kg/day versus 123 kcal/kg/day).
Blinding here would have been a challenge as nurses and other health care providers would have been able to calculate the expected volumes at different fluid administration levels. Nonetheless there was a difference.
The question though that many would ask is whether this better growth came at the expense of greater morbidity. Let’s be clear here that the study was not powered to look at adverse outcomes and the numbers in the above table are small but no difference was seen nonetheless. To appease the most cautious of Neonatologists I suspect a larger study powered to look at adverse outcomes will be needed. What this study does though is raise the question of whether we can and should try larger volumes. As the title suggests I wonder about getting bigger faster so one can go home. With this more rapid rate of growth can we expect a faster maturation as well? I doubt it but it is something to certainly question in a larger study!
After developing a community of over 23000 people unfortunately I had to close my Facebook site due to concerns over a hack. Not to worry as I have created a new independent site to share information daily in Neonatology. I look forward to building an audience at this site and working to continue the dialogue I have come to enjoy with all the followers.
Alternatively if you are on Facebook you can search for All Things Neonatal. Make sure you include the period in the search to take you to the new site.
I look forward to continuing the journey that we started five years ago and expanding the knowledge base for neonatology globally!