I spend a bit of time on social media and when I do I come across the argument that vaccines aren’t needed in pregnancy if you have already had COVID. The concept from the vaccine hesitant is based on the notion of trying to avoid any perceived risk of vaccination when the body is already making antibodies against the virus. The literature has been fairly scant on newborns in terms of protective antibodies and limited to case reports/series that I have shared from time to time on either twitter or facebook. As you might expect something might have changed as I am writing a piece on this topic again. The change is related to a recent paper entitled Titers of SARS CoV-2 antibodies in cord blood of neonates whose mothers contracted SARS CoV-2 (COVID-19) during pregnancy and in those whose mothers were vaccinated with mRNA to SARS CoV-2 during pregnancy by Kashani-Legumsky et al in J Perinatol.
Setting The Stage
Before getting in to what they did it is important to understand how the mRNA vaccines work as the antibodies that one can look at in mothers and babies are of two types. The mRNA vaccines instruct the body to make anti-bodies against the spike protein (S antibodies) which forms the basis of how the vaccine helps our bodies identify the virus and then destroy it. For those who have actually been exposed to the virus and are not vaccinated, they develop a second antibody to the nucelocapsid protein (N antibody) which is within the viral core so this type will only be present in people who have been infected with the virus and their immune systems have dealt with it on their own. This is an important distinction as it allows you to create pure samples of people who have had the virus as a true infection and those who have been vaccinated and finally those who are neither.
Comparing Three Groups
So the authors here decided to compare three groups of women. Eighty three cord blood samples were divided into three groups (from the paper quoted) based on IgG antibody titres.
Group 1 included 29 samples (37%) from women who were infected with SARS-CoV-2 during pregnancy. Twelve had RT-PCR confirmed Covid-19 infection: three were infected in the first trimester, three in the second trimester and six in the third trimester. The other 17 had no clinical signs of SARS-CoV-2 infection during pregnancy and had a positive serologic test on admission. None of the 17 women had active SARS-CoV-2 infection at the time of delivery. Group 2 included 29 samples (37%) from women who were vaccinated against SARS-CoV-2 in the 3rd trimester.
Group 3 included 21 women (34%) and served as controls.
Looking at antibody levels in Group 1&2, 100% were positive for S antibodies. Interestingly, in group 1, 4 women did not test positive for the N antibody (3 were asymptomatic and one infected in the 1st trimester). In group 3 none of the women tested positive for any antibodies confirming they were neither vaccinated or had the infection previously.
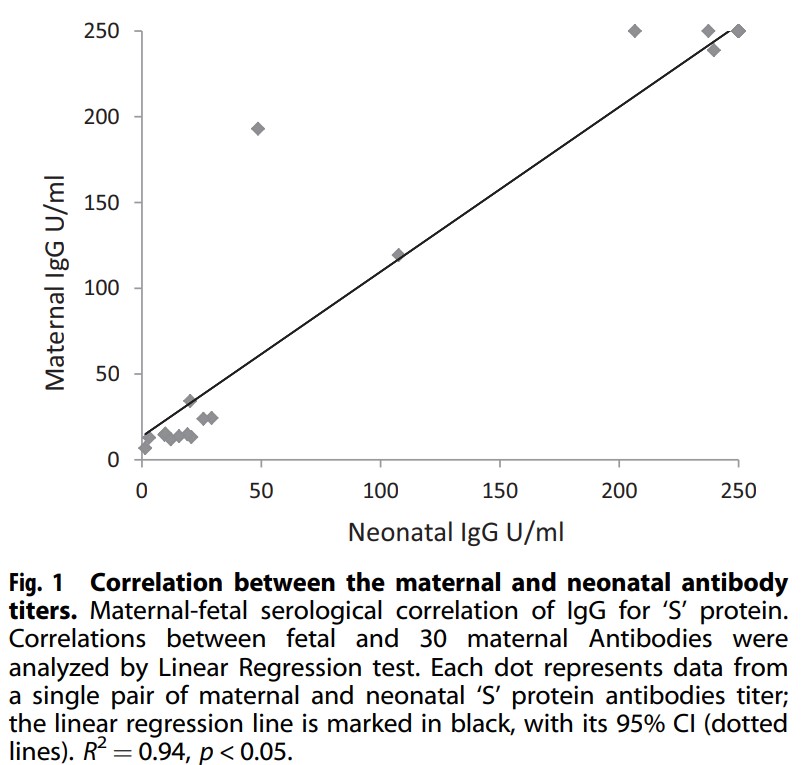
Looking at mean antibody S titres there was a significant difference found in that Group 1 had a mean of 83.7 U/mL vs 225.5 U/mL for the newborns whose mothers were vaccinated. Also notable was the relationship (not surprisingly between antibody levels in the mother at the time of delivery and newborn cord blood titres.
There was a linear correlation between the level in the mother and the level found in the newborn with higher levels presumably better for protecting the infant. Having said that, no infants in this study had neonatal COVID infection. Detractors would be quick to point out that this indicates it doesn’t matter if you get the vaccine since all babies were ok but remember although this may be the biggest study looking at antibodies in cord blood it remains a very small sample and neonatal infection although reported, remains a very rare occurrence.
The Other Side
If you have followed my coverage of the COVID saga from the start you would know that I am in favour of vaccination and in pregnancy as well. The results of this study are encouraging but we need to compare apples to apples. This study compared women who were vaccinated in the 3rd trimester to women who were infected at earlier time points and may have been sick or asymptomatic. The lower antibody levels found in group 1 could represent declining titres as the infection becomes more remote. What we also don’t know is what they antibody levels would have looked like in group 2 if the mothers were vaccinated in the 1st or 2nd trimester as this is now happening. Would the levels be similar? They just might be as the antibody levels do decline with time. We rely on memory cells to reactivate our antibody producing cells if the virus comes along again.
I am not saying this study is meaningless but be prepared if you quote this study for vaccine hesitant to point out that you are comparing recent vaccination to potentially mild cases or remote infections. What is clear and hopeful though is that your newborn is protected by antibodies you make in pregnancy from vaccination at very good levels and until we can vaccinate babies this is the greatest protection we can offer.
As awful as COVID19 has been over the last year and a half one thing has continued to perplex myself and others. Why do babies whethe term or preterm so rarely acquire the virus? Numerous studies have been able to document placental changes and infection of these tissues. On rare occasions reports have come out with evidence of neonatal infection but fortunately most are mild.
These findings have in large part contributed to the Canadian Pediatric Society practice points on three topics.
In this post an argument was made that the reason these infants are resistant is due to low levels of ACE-2 receptors in the nasal mucosa of children. In this study children as young as 4 years of age were found to have very low levels of this receptor (portal of entry for SARS-CoV-2) into the host. I speculated at the time that if one carried forward the findings to younger children and infants you might find there were hardly any receptors at all.
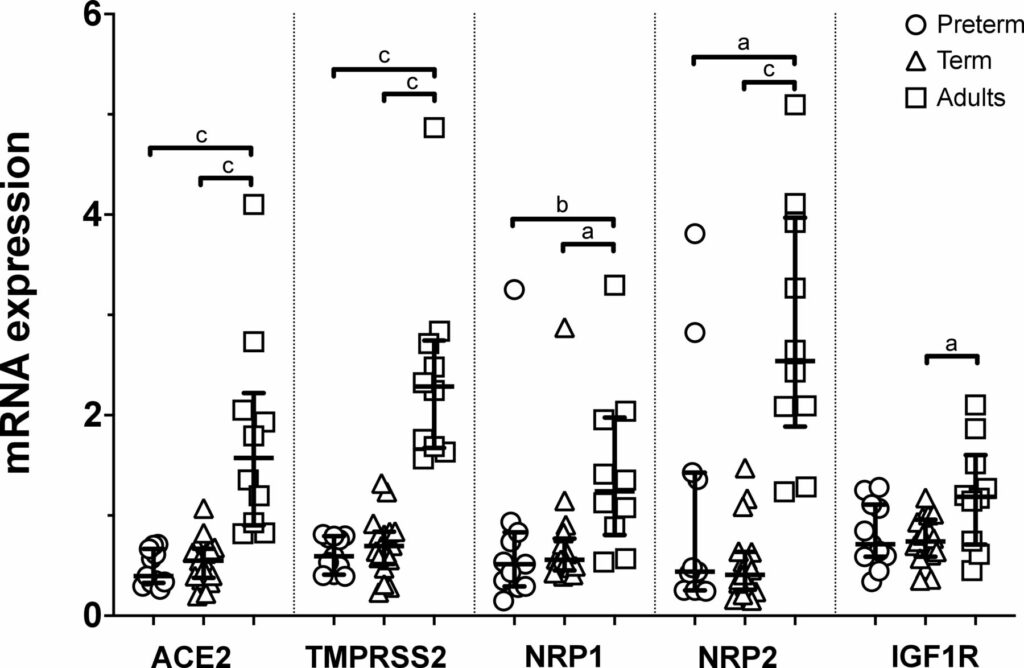
Well, someone finally did the study and confirmed what I suspected. The study report is entitled Nasal expression of SARS-CoV-2 entry receptors in newborns by Heinonen S et al. It’s not a big study but the results are consistent across 28 newborns (17 term and 11 preterm) and 10 adults. In each newborn whether term or preterm a nasal mucosal scraping was performed at 24 hours of age and used to measure by reverse-transcription quantitative PCR mRNA expression of ACE2, transmembrane serine protease 2 (TMPRSS2), neuropilin 1 (NRP1) and neuropilin 2 (NRP2) and insulin-like growth factor 1 receptor (IGF1R).
What the results show you is that babies are not just small adults. They are different yet preterm do not seem to be that different than term infants in terms of receptors. While ACE2 has garnered most of the attention when it comes to receptors for SARS-CoV-2 the others also play a role and are in general expressed to a lesser degree in neonates than adults.
Conclusions
In the previous post I argued what was in your nose makes a difference to your risk of contracting SARS-CoV-2. Really the point is what is not in your nose. Thankfully neonates do not have good expression of these receptors and that may be the biggest reason for the general protection they have from this pandemic. It has certainly a good time to be in the “have not” group!
This post is a written as a tribute to John Minski RRT who taught me much about ventilation over the years and has been a champion for innovation in our unit. As he prepares to move on to the next phase of his life I thought it would be a nice send off to talk about something that he has been passionate about for some time. That passion is inhaled nitric oxide for more than just pulmonary hypertension.
Prior Evidence
This is actually nothing really new. For a review on the background behind the theory you can read The potential of nitric oxide releasing therapies as antimicrobial agents. While we think of iNO as being a drug for pulmonary hypertension it has other capabilities. It can diffuse across cell membranes and damage pathogens by causing nitrosative and oxidative damage. The amount of iNO needed though to accomplish this bactericidal action is much higher than the typical levels of 20 – 40 ppm that we use. Last year in August Bogdanovski et al published Antibacterial activity of high-dose nitric oxide against pulmonary Mycobacterium abscessus disease. They describe a protocol of providing 30 minute doses of 160 ppm for 21 days in a 24 year old patient with cystic fibrosis who was infected with mycobacterium abscessus. While they were not able to eradicate the organism, they were able to demonstrate functional improvement in the patient. Also notable was the absence of adverse effects in terms of methemoglobin levels. Other prior research in-vitro has shown iNO at high levels to be truly bacteriocidal as per the review above.
In this paper they describe the use of iNO at 160 ppm in 5 spontaneously breathing patients with confirmed COVID19 infection. This was provided as a rescue therapy in the absence of any high quality therapies for this disease. The protocol was to give them the same dose of 160 ppm for 30 minutes at a time until resolution of their symptoms with those that received multiple treatments getting anywhere from 5-9 courses. In each case after each 30 minute period the treating physicians measured levels of methemoglobin and nitrogen dioxide and found in each patient acceptable levels after these brief exposures.
Results
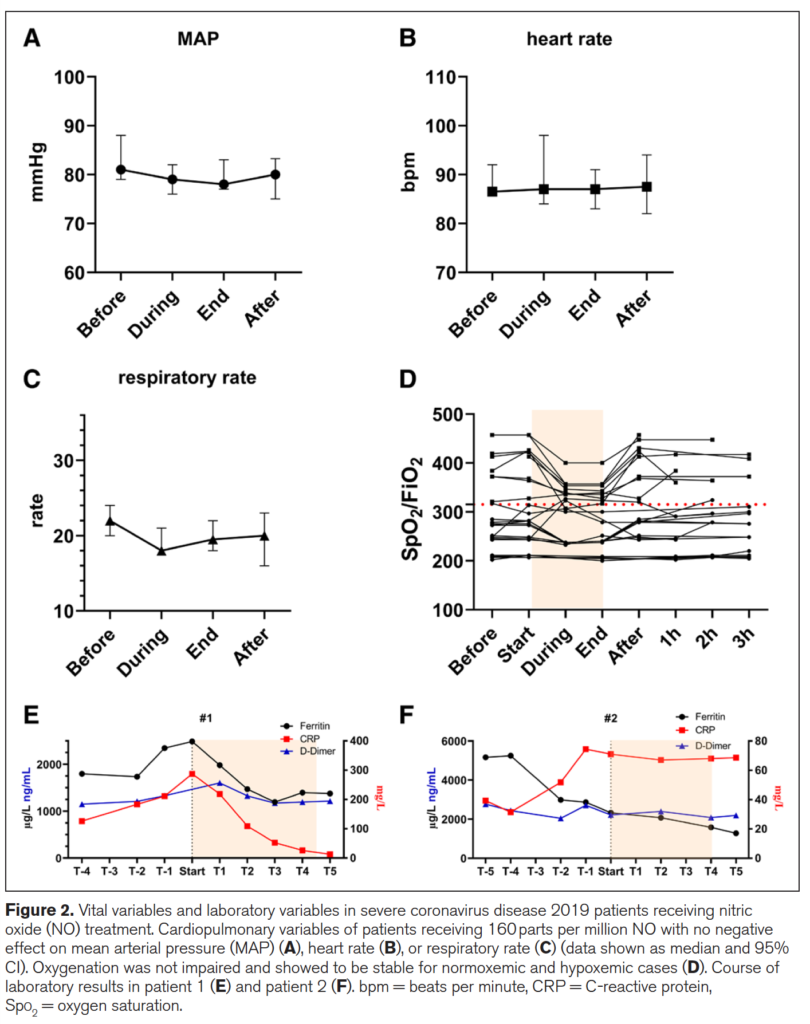
Of the 5 patients treated 2 died from COVID19 and three survived. The two patients who died interestingly were the ones who each only received one treatment each. The other three received 5, 8 and 9 treatments respectively. The authors recorded mean arterial pressure, heart rate, respiratory rate, SpO2/FiO2 and finally measurements of inflammatory markers in the two patients who died (E) and the 3 who survived in (F) in the figure below.
What is interesting from the figure above is the reduction in respiratory rate during treatment (certainly could be placebo from believing they will get better) but the oxygenation during the treatment improved as well. Could this be from a reduction in associated pulmonary hypertension? Certainly could be. Looking at the patients who died in (E) vs the ones in (F) who survived (patient 3 not shown) demonstrate that use of iNO stopped the rise in CRP and in the case of those who died reduced it significantly. There could be an argument made then that the changes in respiratory pattern observed during treatment are associated with a concomitant attenuation of inflammation. This treatment just might work but of course needs far more studies to be certain of that. On that note a review of iNO for this type of indication reveals there are currently 16 studies enrolling in this area of research so I imagine there will be more info to come with this story.
What about the neonate with pneumonia?
I sent this paper around to my colleagues and it generated some great discussion. I am no Ethicist but the question raised was could this be considered a “last ditch” treatment for the neonate succumbing to a pneumonia? I have no doubt if you are reading this that you will have seen in neonatal units around the world that there are infants who develop pneumonia unresponsive to traditional treatments such as iNO at regular doses, antibiotics, higher PEEP, surfactant etc. If we have this knowledge with respect to the potential use of iNO at high dose and a positive impact on pulmonary infective disease is this something that should be offered to parents?
We have no date to my knowledge in babies on the use of this type of dosing but it comes down to a question of what is the alternative? If a patient is dying on the ventilator are we at the point of knowledge here that it is worth offering the family this treatment? One could do so with full disclosure about the lack of neonatal data both for effectiveness and safety. Or do you fall on the side of it could be harmful and expedite death so should not be used. If you use it though and wait till the patient is in extremus on 100% oxygen might it be too late? Do parents have the right to know when they ask the question “is there anything else you can do?” For me I think the answer is that there should be a discussion with this evolving research out there. I am comfortable with it as long as the parents understand the potential for it to make things worse and shorten their time with their child. Alternatively if they choose not to that is their prerogative but should they have the choice when the competing outcome is death?
I can’t tell you whether you should or shouldn’t offer this in your institution but my suspicion is that you will be discussing this among colleagues before long. Who knows you might just one day say you saw it here first!
Thanks John M for the inspiration and keep sending those articles!
Testing for COVID19 has become so much the norm in society that in casual conversation you might ask someone if they have been tested. Chances are you know someone who has and even more likely that it is many people at this point. If you have been following this blog for awhile you would know that one of the issues with testing is that it is extremely sensitive. The RT-PCR test can pick up even trace viral particles whether alive or dead and therefore a test in and of itself tells you one thing. There is virus present but whether it is alive or dead is another matter. Virus can be shed for weeks after symptoms develop so what information can we obtain that might tell us whether the patient is at risk of infecting another person. Moreover, when can we relax precautions around the patient themselves and no longer worry that they are a risk to others?
Winnipeg Researchers May Have the Answer
Given that I know many of the authors of the paper personally that I will discuss and the quality of the work they do I am delighted to cover this important work. The paper Predicting Infectious Severe Acute Respiratory Syndrome Coronavirus 2 From Diagnostic Samples by Bullard J et al tackles the question above using cycle times and times to positivity after initial symptoms. First off it is important to understand the concept of cycle time. When you use RT-PCR to amplify pieces of RNA there are 40 cycles of amplification that a sample is put through. The lower the number of cycles required to detect the RNA the more viral material was present to begin with. As the cycle times get well into the 30s the possibility of there being just trace amounts of virus exists or that the patient themselves had no virus present but the sample was contaminated with a very small quantity of virus. The time to positivity is the amount of hours/ days it takes after initial symptoms develop until an RT-PCR test becomes positive.
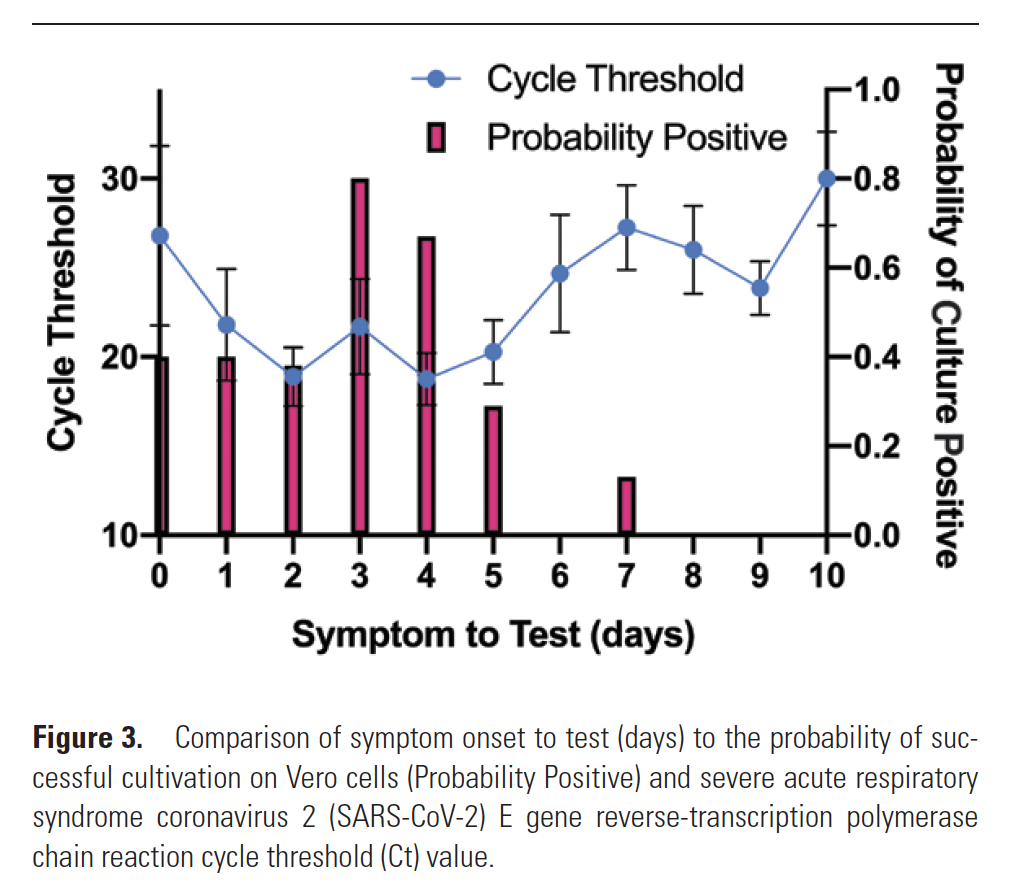
The authors analyzed 90 samples either from naso-pharyngeal swab or ETT secretions with a median age of 45 years (I know not neonatal). Collected samples included from day 0 to day 21 after symptom onset. What the authors did that was interesting in this paper was that in addition to the samples being tested by RT-PCR, for each positive sample they went through the laborious task of performing tissue culture to attempt to grow the virus. By doing so the authors were then able to compare the time to positivity (STT) and Ct thesholds to determine if there were numbers for each that could be used to predict which samples would have live virus that could be grown,
The Results Please
The two main findings in the paper were that no patient after day 8 from symptom onset with a positive RT-PCR could actually have live virus grown in tissue culture. This is shown in Figure 3 from the paper
Secondly, no patient with a cycle time greater than 24 could also have live virus grown. In fact for every 1 unit increase of Ct the odds ratio for infectivity decreased by 32%.
The size of the study is fairly large when it comes to COVID19 studies like this but as the authors say the results are for adults and given how few children have been infected especially in our location in Canada we should be hesitant to generalize to children and in particular neonates.
What the study does give us
This study I felt was worth sharing with you for the reassurance that I think it may give especially if it leads to further validation by even larger studies including children and those who are immunocompromised who may have prolonged shedding. What it suggests though is that the next time you encounter a patient who you are told tests positive there are a couple important questions to ask from your lab. The first is how many days from the start of symptoms was the RT-PCR done? Secondly, ask them for the Ct value. As per the authors
“Receiver operating characteristic curves constructed using Ct vs positive culture showed an area of 0.91 (95% CI, .85–.97; P < .001) with 97% specificity obtained at a Ct of > 24. Similarly, STT vs positive culture showed an area of 0.81 (95% CI .73–.90; P < .001), with 96% specificity at > 8 days”
In other words, if the answers to those questions are >8 days and a value for Ct >24 you should be able to leave the patient with reasonable expectation that they are either no longer infectious or at worst almost clear of live virus.
Interesting work that I hope will be helpful to someone out there!
Regardless of where you live, you may have noticed that this year’s flu and RSV season has not been as bad as in previous years. I recall early in the pandemic hearing that Australia had virtually no flu season at all this year. The question therefore is where did these viruses go? Many people have attributed the drop is other viral illnesses to the fact that we are wearing masks and washing our hands a lot more. This no doubt has something to do with it but the reality is that many have chosen not to wear masks and additionally we know that others have failed to use PPE appropriately. Let’s face it, COVID has spread far and wide and yet the other viruses have not. So where did they go?
Viral Interference
This is a subject I had never heard of or really considered as an entity until I began looking at COVID19 as part of a talk I gave this year. The concept has been known since the 1930s or even earlier. The first reference I found for this was by Findlay GM An interference phenomenon in relation to yellow fever and other viruses from 1937 (sorry no link to the paper) and then Lennette EH, Koprowski H. INTERFERENCE BETWEEN VIRUSES IN TISSUE CULTURE. J Exp Med. 1946 Feb 28;83(3):195-219. In this latter study innoculation of yellow fever virus and the West Nile virus produced either partial or complete suppression of growth of the Venezuelan equine encephalomyelitis virus. In other words, the idea here is that once one virus takes hold of a cell it becomes quite difficult (but not impossible) for another virus to also grow at the same time. Looking at how SARS-CoV-2 and RSV might interact is interesting as in tissue culture RSV is the slower replicating virus. SARS-CoV-2 seems to grow in cell culture in the order of 3-5 days while RSV tends to be longer at 5-14 days. In vivo of course things can be different as the host can influence rapidity of growth but the if SARS-CoV-2 is spreading rapidly through the community it could be that by infecting the host first and being the faster growing virus it effectively and strangely protects the host against other viruses such as RSV. If there is anything about this pandemic that maybe we can take some comfort it it is maybe that!
What about disease severtiy when two viruses take hold?
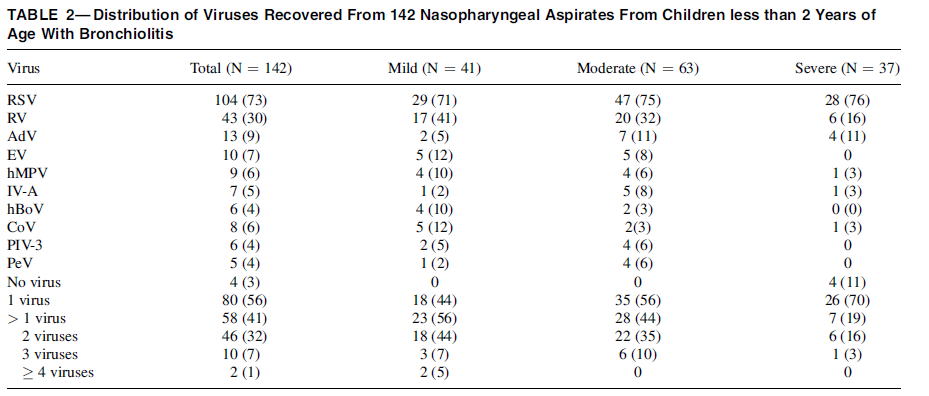
You would think if you were unlucky enough to get RSV and COVID19 at the same time your symptoms would be worse than getting RSV alone but the evidence suggests otherwise. Having two viruses competing for the same host may lessen the severity of the disease. This was demonstrated by Kim Brand H et al in Infection with multiple viruses is not associated with increased disease severity in children with bronchiolitis Pediatr Pulmonol 2012 Apr;47(4):393-400, In this study the authors examined 142 nasal aspirates of children with bronchiolitis and grouped them into categories of mild, moderate and severe disease. What they found suggests that two or more viruses infecting the same host may reduce the severity of the illness usually ascribed to the virus compared to when it affects the host alone. In the case of RSV from Table 2 above, with severe bronciolitis, RSV was found 76% of the time. Bronchiolitis may be caused by other viruses of course and towards the bottom of the table when severe disease was present one virus was found 70% of the time. Howeve as the number of viruses in the host increased the likelihood of severe diease dropped while mild diease increased.
What to expect then?
I am just a Neonatologist but based on the above research I am expecting a couple things this winter season. I predict we will continue to see lower rates of RSV infection and perhaps influenza as the domination of SARS-CoV-2 continues. The other thing that will be interestin to look at retrospectively will be what the distribution of disease spectrum for RSV is this season as if the above is correct we should see less severe disease when looking at emergency visits and hospitalizations. Will be an interesting story for 2021 and I suspect much will be written about the impacts of COVID19 on many fronts. Look forward to no longer talkign about that virus at some point later in 2021 when we all start saying “remember when…”
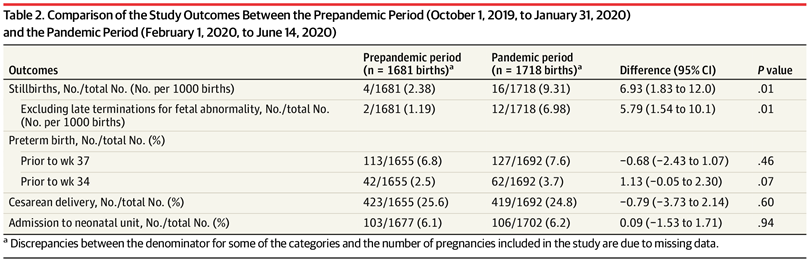
This topic has been making its rounds for awhile now. Periodically whether on Twitter or via email I get asked this exact question. Anecdotally, the numbers of babies in the NICUs across many units in Canada seem to be lower as estimated by various Neonatologists. The question is whether this is real or not and without national data it is tough to say for sure. This week though a research letter came out of the UK entitled Change in the Incidence of Stillbirth and Preterm Delivery During the COVID-19 Pandemic. The authors compared two time periods at a single centre ; St George’s University Hospital, London in 2 epochs: from October 1, 2019, to January 31, 2020 (preceding the first reported UK cases of COVID-19), and from February 1, 2020, to June 14, 2020. Specifically they wanted to look at the rate of stillbirths and preterm births during these two time periods.
What did they find?
There were 1681 births in the prepandemic period and 1718 births during the pandemic. There were no differences in maternal characteristics before and after so presumably if there is a difference in rates of stillbirth and preterm birth it might be the influence of the pandemic. As it is an observational study though it certainly is possible that unmeasured factors are different in the groups but let’s give them the benefit of the doubt.
The rate of stillbirth was up and by a significant margin but the rate of preterm birth was not. There certainly was a trend though towards an increase in preterm delivery prior to 34 weeks. While I don’t know what the cause of all this is for sure it sure is fun to speculate.
Possible reasons for higher rates of stillbirth
It has been documented that rates of perforated appendicitis in our own centre increased during the pandemic. As the population became frightened of leaving the home, more and more people waited longer to go to the hospital to seek care. I can’t help but wonder if the same thing may have happened here. Might the pattern of seeking care by women for decreased fetal movement shifted ever so slightly? What about the frequency of prenatal visits? In Manitoba a COVID modified approach was done with fewer visits than normal. It certainly is possible that women by having fewer visits could have in some cases missed clinical findings that might have alerted a midwife or obstetrician to a reason to deliver early.
Possible reasons for a decline in preterm birth
The authors here did not find a difference but in fairness out of the number of pregnancies the number of preterm births would have been about 10% so difficult to really find a difference. Given that under 34 weeks showed a trend to a lower number let’s assume that there might be a difference (or not).
At least in terms of the perception of lower rates, this might be a case of confirmation bias. One of my colleagues who initally sent me an email from another institution two weeks later sent another that said “I thought we were seeing lower rates and now we are packed to the rafters”. It could well be that we are all noticing when the census is low and not paying attention to the times when it rises. Every time the numbers drop it seems to confirm our suspicions.
It wasn’t from people choosing to delay family planning as it was too early to see a change in birth rate. I do worry though that we may see declining admissions in the latter part of the year and then a “boom” when a vaccine is produced as families once again choose to conceive. This happened similarly during the Zika epidemic in Brazil.
It could also be that the finding is real. During the pandemic essentially all pregnant women went on extended rest. Instead of dealing with stressful daily tasks like battling traffic, being late for work and working altogether they were told to stay at home. Financial stress could have then been a factor but at least in Canada the government provided $2000 a month to offset the job losses. It is quite possible at least in my mind that an extended period of rest could have truly led to less preterm birth.
The Future
The next step I imagine will be for larger organizations such as the Public Health Agency of Canada to publish their data on this and see what happened across Canada during this period. When we are able to look at tens of thousands of pregnancies we will have enough numbers to drill down whether there has been a change for our smallest infants or not.