When it comes to non-invasive ventilation the field has become a little more crowded in recent years at least in our institution. In the recent past if one decided to extubate an ELGAN the biggest decision was what CPAP pressure to use. These days we have the option of high frequency nasal ventilation (nHFOV) or non-invasive positive pressure ventilation (NIPPV) to choose from as additional options. Both of these modalities have their uses and I have written about nHFOV before as in Nasal High Frequency Oscillatory Ventilation For Preventing Intubation. On this post though I want to look at NIPPV which has actually been around longer as a modality. The gist of this mode is that one chooses a delta P, peep, Ti and rate much like you would on a conventional ventilator. When ventilating through a nasal interface the device provides ventilation although it is questionable I suppose how much of that is alveolar ventilation. The study we are going to talk about here caught my eye as the information gleaned from it gives me at least an idea of how this mode may work to help prevent reintubations.
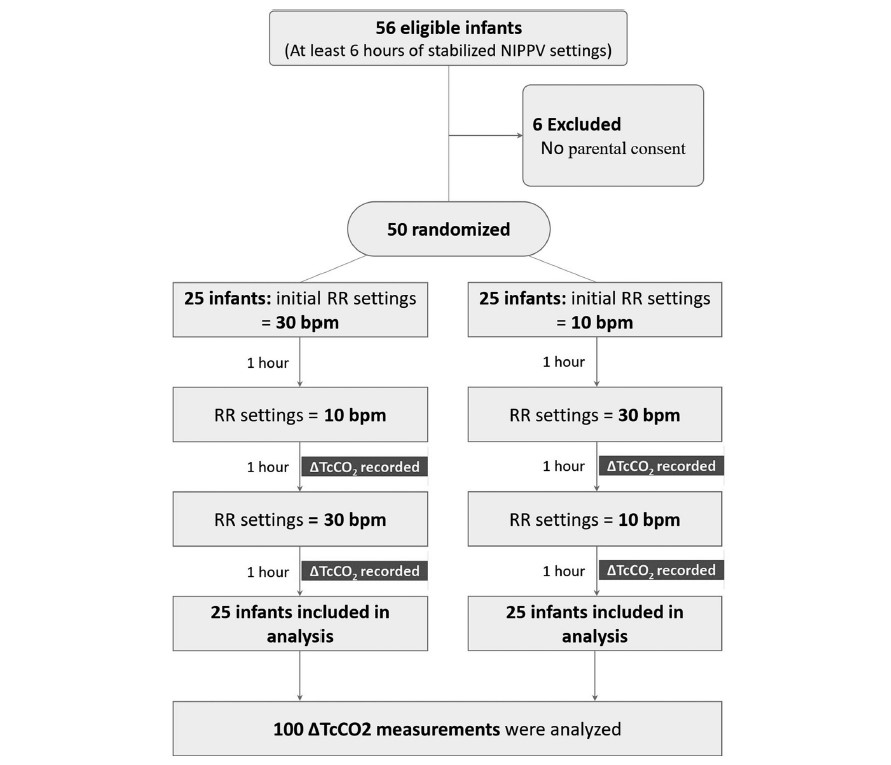
In this study each patient served as their own control and alternated between either a start of a rate of 10 BPM or a rate of 30 BPM as shown in the following diagram. The infants were all between 24 +0 and 32 +6 weeks gestation to be included in the study. Delivery of NIPPV was through the Leoni Ventilator using RAM cannulae and importantly the mode was non-synchronized. Each infant needed to be stable on their settings for at least 6 hours before being included. The authors hypothesis was that rate matters to clear carbon dioxide. To monitor CO2 levels they used transcutaneous CO2 measurements to allow for continuous measurement over each hour of the study. Given this belief, there was safety built into the protocol such that patients were excluded if on the set rate of 10 bpm the tcCO2-related pCO2 was <40 mmHg, or on NIPPV if the set rate of 30 bpm had a tcCO2-related-pCO2 is 60 mmHg, In other words, if rate matters and your tcCO2 was already less than 40 on a low rate then it would not be safe to blow off more CO2 and vice versa with high CO2 and low rates. To ensure that only rate affected the results “during the 3 h of the study no changes in PIP, PEEP or FiO2 were allowed with the following exceptions: if spO2 was <90% or >95% for more than 20 s, an increase or decrease in FiO2 were allowed to keep spO2 90–94%, and were documented”.
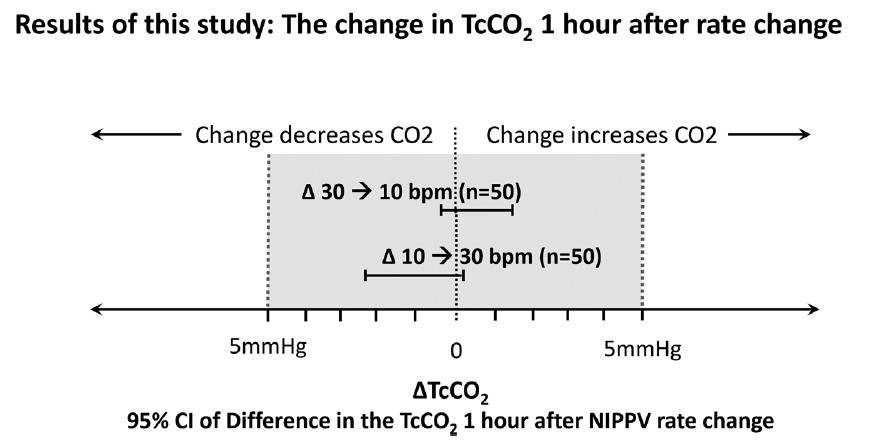
So does rate matter?
It turns out the authors found no difference in CO2 levels based on rate changes alone.
This of course is contrary to what the authors expected to find. The question is why this might be. What follows now is just speculation on my part but given the finding of no difference I can offer a few thoughts. The first is that NIPPV does not involve a distal delivery of gas like the situation of an endotracheal tube near the carina. With an endotracheal tube in place the delta P or pressure above the set peep is delivered to the gas exchanging areas of the lung. With NIPPV you are delivering the pressure at the nose and therefore there is a fair amount of dead space in between the exit of the gas into the baby and the lung. Might you just be really ventilating dead space for the most part?
Secondly, depending on the fit of the mask or the degree that the mouth was open how do we know how much of the non-invasive ventilation reached the infant? Lastly, in our own centre we have not been impressed with the RAM cannulae as we have found that whether the prongs are in or out of the nose the pressure being detected as being delivered seems to stay the same at least as the ventilator sees it. If the prongs were not in the nose properly and the atmosphere was being ventilated would one really know that the pressures weren’t really getting into the nose?
Lastly, the Leoni ventilator is not capable of delivering synchronized NIPPV. Now that there is the availability of synchronization on ventilators such as on the Puritan Bennett 980 ventilator it would be interesting to see the same study done again. If you are delivering non-synchronized breaths which are not in sync with the patient should we expect a change in CO2? What if half the breaths for example by chance are delivered on exhalation? Not much effect on CO2 I would think.
I am not saying that rate doesn’t matter at all but I suppose I am saying within the context of this study it doesn’t matter to CO2. My best guess as to how NIPPV works to prevent reintubation may be secondary to two things. The first would be by irritating the baby with the puffs of delta P. Think of it like intermittent stimulation. The second possibility is that the same puffs of air help keep the pharynx open and minimizes the obstructive portion of apnea of prematurity. Whatever the reason NIPPV appears to work to prevent reintubation in some infants!
I have no doubt the group here will look at the effect of delta P on CO2 soon enough and I wonder if we will see much difference there either. It also will be important to look at the effect of rate in a synchronized fashion! Time will tell.
Over the last number of years clinicians have sought more and more to limit the experience of babies to painful stimuli. In the area of surfactant administration this has focused on “less invasive” strategies such as use of small catheters while on CPAP (LISA or MIST) and surfactant via LMA or Surfactant Administration Through Laryngeal or Supraglottic Airways (SALSA) as it is sometimes known. Intubation Surfactant Extubation (INSURE) while not generally included in the less invasive approach is to a degree fitting since it involves at least intubating for a very brief period after surfactant is administered. SALSA has been growing in popularity due to its “extreme” non-invasiveness since babies are receiving surfactant without instrumentation of the airway at all. It should come as no surprise then that head to head comparisons will be done to determine which should be reigned king!
The Contenders
A group out of Albany, NY has looked at SALSA vs INSURE before in which they used morphine for premedication prior to the procedure. You might ask why any premedication is needed at all but I would suggest that covering one’s airway and dripping liquid into it might cause some irritation so why not keep them calm. The authors in their paper Randomized trial of laryngeal mask airway versus endotracheal intubation for surfactant delivery found a high rate of failure in the intubation arm which more than likely was attributable to the respiratory depressive effect of the same.
This time around in the current paper Randomized Trial of Surfactant Therapy via Laryngeal Mask Airway Versus Brief Tracheal Intubation in Neonates Born Preterm they switched to remifentanil for its brief duration of action. Babies in the SALSA arm received that drug while those in the ETT group received atropine as well. The authors included infants born from 27 weeks to 36 weeks gestation who were larger than 800g at birth. This was a non-inferiority trial with the primary outcome being Our primary outcome was failure of surfactant therapy to prevent the need for invasive mechanical ventilation or its surrogate indicators, namely, more than 2 doses of surfactant therapy, sustained need for FiO2 >0.60 to maintain target O2 saturations, or a second dose of surfactant within 8 hours of the first dose.
Surfactant redosing criteria were the same for both groups: FiO2 >0.60 or FiO2 >0.30 with clinical signs of worsening RDS. If surfactant needed to be given a second time it was via intubation. The decision to ultimately intubate though was in the hands of the practitioners.
Unfortunately, the trial was stopped after only 51 patients were enrolled into the LMA and 42 into the INSURE groups respectively. Randomization was by block design and the authors were looking for 130 patients per group so they fell far short of that. The reasons for falling short were interesting as they demonstrate one of the challenges of research and changing beliefs. At the start of the trial there was equipoise among practitioners with respect to the two modes of surfactant delivery but part way through people preferred SALSA. The authors changed the randomization to try and deal with that to a 2:1 favoring SALSA but with the combination of that and COVID they had to stop. They did manage to get enough though to determine the primary outcome in spite of this.
What did they find in the end?
Well first of all it is worth noting that there were no differences in baseline characteristics between the two groups. As it turns out, while the numbers were small it didn’t seem to lead to an unbalancing of groups.
With respect to inferiority the finding was that it was in fact not inferior as per the figure below.
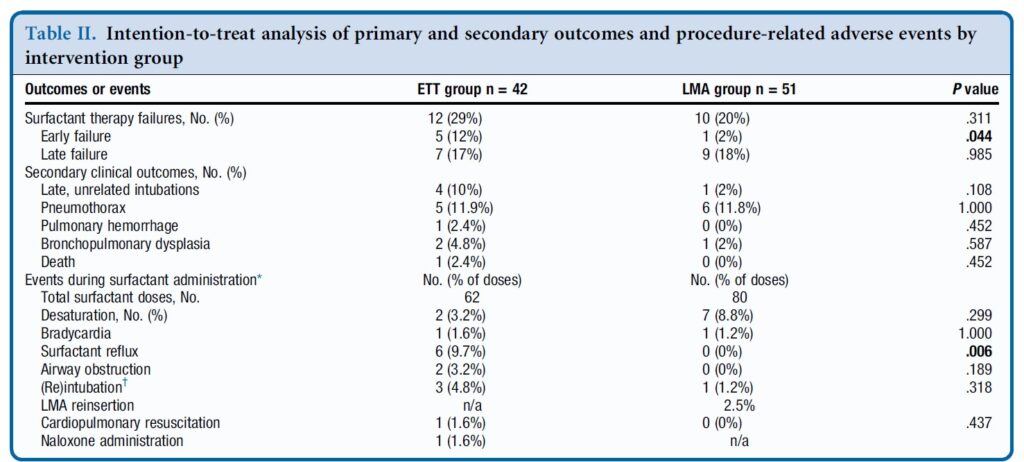
In table 2 some interesting findings emerge
Early failure of surfactant which was defined as within 1 hour of surfactant administration was found to be significantly increased in the intubation group. Late failure through at 5 days of age was not any different. An early failure is suggestive of the procedure not working to deliver the surfactant. When you look at the bottom half of table 2 the answer may be there. As part of the planned procedure the authors aspirated a gastric tube after surfactant administration to ensure that it went to the right place. There was no difference in surfactant volume aspirated via this route. There was however 9.7% of infants in the ETT group that experienced reflux in the ETT vs zero with observed reflux in the SALSA group (in the mouth perhaps?). Is surfactant without PPV better tolerated maybe?
There was a trend overall to more failures in the ETT arm although this was not found to be significant either in the intention to treat or per protocol analysis.
Where do we go from here?
First off it is important to look at who was chosen for this strategy. You may have noticed that there were no micropreemies in this trial. The reason for this is likely two-fold. The first is that prior trials on SALSA have found it doesn’t work as well to prevent intubations in babies below 27 weeks. This is very similar to the findings of studies using aerosolized surfactant. It may well be that there just isn’t enough of the total dose getting to the alveoli. If you can get some of the dose in deep into the lung for those with less severe RDS it may work ok for those babies. The second reason likely has to do with using LMAs in those in that weight range as they generally are designed for larger preemies although I understand smaller ones are becoming more readily available.
The second point is that this was not a blinded study. This could have become an issue as the authors acknowledge that there was a growing institutional preference for SALSA as the study went on. If the Neonatologist subconsciously believes it is better, might that have influenced some of the decisions to intubate again since one of the criteria was “clinical signs of worsening RDS”. It is quite possible this could have led to a few more intubations in the INSURE group for repeat doses. We can’t prove that but it is a weakness of the study.
At the very least it can be argued that the use of SALSA works as a small percentage overall failed the procedure. The largest groups of infants though were above 29 weeks so we also might not expect a high rate of failure after one dose though. It works but how well is tough to say.
Where I think this study is really important though is what it tells us for centers in particular who don’t intubate as often. Intubation is a skill that is declining in opportunity, both because of a turn to more use of non-invasive support as a primary mode of treatment. It also has become scarcer at an individual level due to there being more practitioners who can perform the skill. Having an option to use SALSA for those who aren’t as comfortable with intubation will no doubt be of much interest to many in this situation.
What is no doubt going to come next is the LISA/MIST vs SALSA trials. I hope that in the future pain scores are included in these sorts of analyses to really determine if in being less invasive we are also ensuring that we are also not undertreating discomfort. I suppose the lesson being learned from all of this is that less very well may be more.
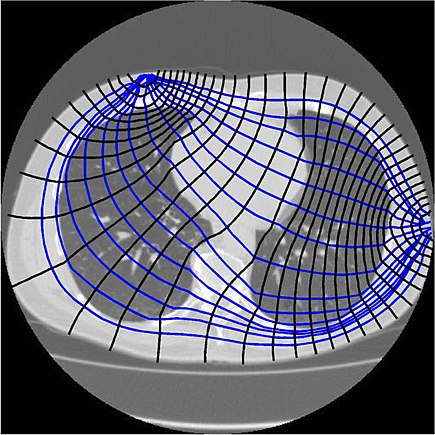
Extubation is a regular occurrence in the NICU. We do our best to predict who will succeed and who will fail but it isn’t always easy to figure out who they are in advance. We use techniques such as looking at oxygenation histograms and using thresholds for PIP, PEEP or MAP but in the end sometimes it works and other times it doesn’t. In an effort to improve on intubation success, some creative researchers in Switzerland employed a technique called end-expiratory lung impedance or EELI to measure lung volume before, during and after the extubation process. The use of EELI is based on the impendance of the lung changing with the distribution of tissue and air and by placing electrodes one can generate a cross sectional volume that has been shown in neonates to be representative of total lung volume. The EELI technique creates an image like this which is use to generate the estimate of lung volume.
The researchers in this study were seeking to do a quality improvement project and use EELI to estimate lung volume at different time points in an extubation. The time points were all 30 seconds including, immediately before first handling of the infant (baseline), tracheal suctioning (suction), start and end of adhesive tape removal (adhesive tape begin and adhesive tape end), pulling the endotracheal tube (extubation), initiation of non-invasive ventilation (NIV), immediately before and after turning the infant to prone position (supine and prone, respectively), and 10 min after turning to prone position (prone10). As per unit policy all babies were ventilated with Draeger VN500 ventilators and if <28 weeks went on to NIPPV when extubated or if 28 weeks or more straight CPAP. The purpose of this quality initiative was to determine using EELI at what point in the extubation process infants might be losing lung volume and then based on the information see if they could ultimately use this to improve the chances of successful extubation in the future.
What makes this study interesting is that the infants were found to lose volume but at a time when I would not have expected it.
The Reveal
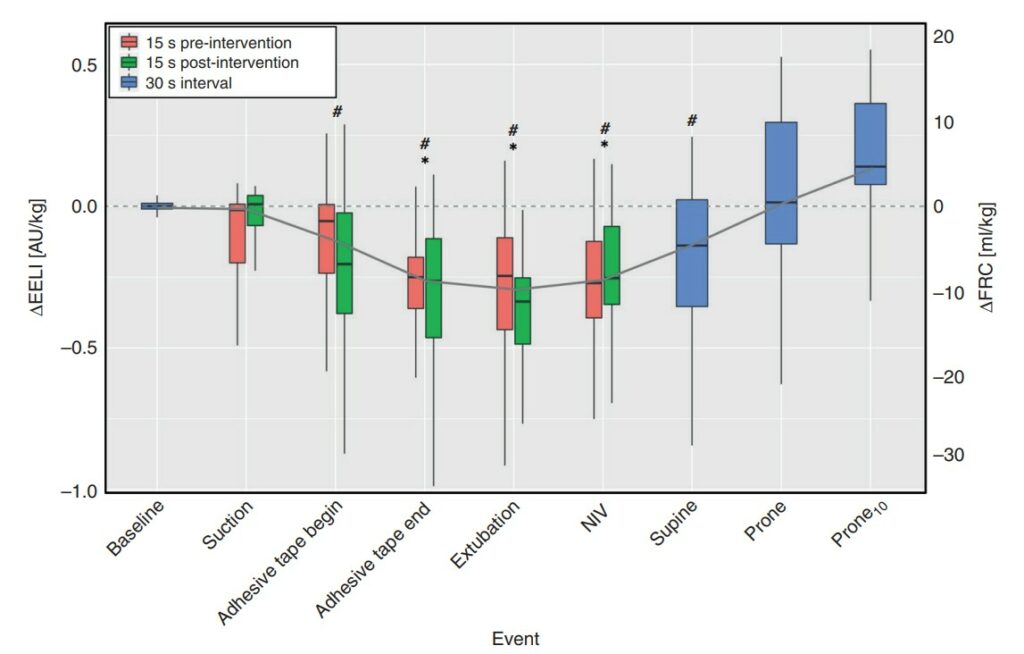
Below is a graphical depiction of EELI and estimates of FRC during the different time points. The changes in electrical impedance by EELI were converted on the right Y axis to an FRC in mL/kg.
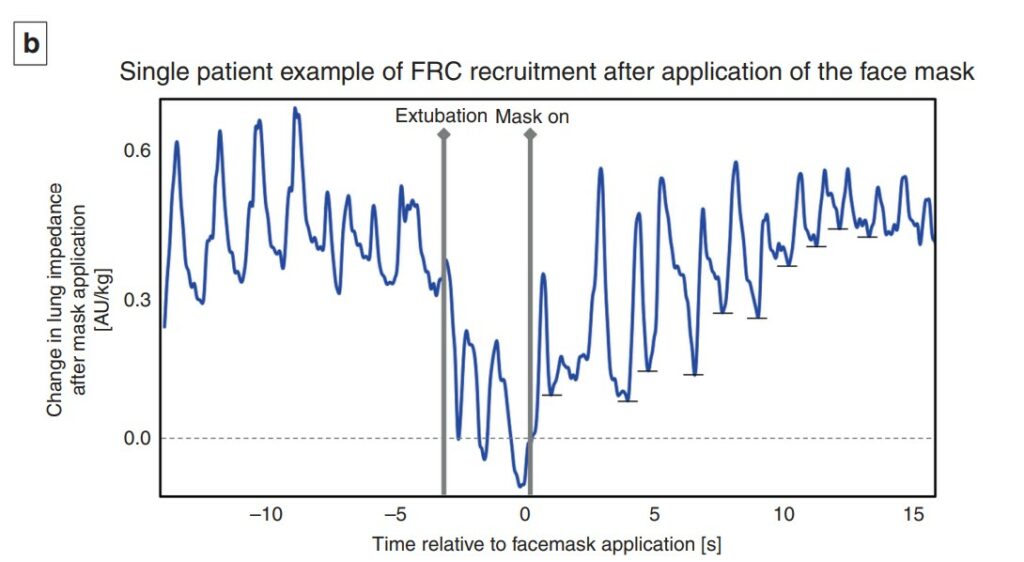
What is surprising at least to me here is the loss of volume occurs not with extubation but rather when the tape removal process happens. With the placement of the prongs on the infant at extubation the FRC gradually rises and recovery occurs. Moreover as shown in the 12 patients included in this study, the recovery once non-invasive ventilation is provided is quite rapid and evident within 1-2 breaths.
A couple other things to note. The loss of FRC during tape removal was about 10 mL/kg and if typical FRC in a preterm infant is 20-25 mL/kg you can see the impact this would have on lung volume and reserve. As this was a small study it could not detect a threshold at which extubation would fail but one infant who developed a pneumothorax and required reintubation did not get back to their baseline FRC.
What is this signaling?
Yes this is a small study but it did look at about 3000 breaths so there is a fair amount of data to look at. What the paper demonstrates I think is that there is a vulnerable time during tape removal where likely due to the fact that we use uncuffed ETTs in neonatology it is possible for these infants to lose lung volume. It may be that as they strain and bear down the ventilator may not be as effective at delivering volume to them. Measures that might help during this time could be skin to skin care, breastmilk drops or scent, sucrose or a variety of other non-pharmacologic measures to keep them calm. This might help to minimize such volume loss. Secondly, knowing the significant risk of volume loss it underlines the importance of placing nasal prongs on as quickly as possible during the transition from invasive to non-invasive ventilation as recovery of lung volume is possible. It think it also suggests that if we are “peepaphobic” and use an insufficient amount of support at extubation these infants may be vulnerable to experience significant volume loss as well.
While EELI may not be perfect, this study is the first of its kind and may shed some light into why some infants fail after extubation. While usually I say less is more, I do wonder if in the case of extubation, this study gives some evidence to support starting with a higher PEEP than you think you need non-invasively and then backing off after one has successfully extubated. This may be the first study I have seen on this but I am certain it won’t be the last.
When I began my career in Neonatology we initially ventilated primarily with pressure limited time cycled modes of ventilation and only supported some of the breaths as in SIMV modes. With time and emerging research a movement to using set volumes came about and in many centres supporting every breath using an assist control mode or similar version. Although I don’t have access to it in my centre, ventilators such as the Avea also allow for automated FiO2 control in addition to having a choice of two different volume targeting modes. The difference between the modes is the subject of a study entitled Comparison of volume guarantee and volume-controlled ventilation both using closed loop inspired oxygen in preterm infants: a randomised crossover study (CLIO-VG study). I suppose it shouldn’t be a big surprise that as technology advances and we fine tune practice, different modes for volume targeting would arise.
What’s the difference?
Volume Controlled Ventilation (VCV) – flow based on a set volume and measurement of the PIP every 2 ms. Next breath is given the greater of PEEP+2 cm H2O or PIP-2 cmH2O. The ventilator at the end of each breath is able to determine if the baby is still demanding flow and continues providing flow but stops when inspiratory flow is <25% of peak set flow. There is constant inspiratory flow and peak volumes.
Volume Guarantee (VG)- inspiratory pressure is adjusted breath to breath. These breaths have a decelerating flow instead of a fixed flow as in VCV.
The Study
Using automated FiO2 control for both groups the study design was a crossover one. The concept was that better ventilation would help to keep O2 saturations more reliably in a target range of 90-95% and that one of these modes might be superior than the other in doing so. Infants in the study were born at 23+0 – 36+6 weeks and had to be intubated and on >21% FiO2 to be part of the study. Each group spent 12 hours in each arm with the starting mode randomly chosen before switching over to the other mode.
Based on a power calculation in which the authors selected looking for a 5% difference they determined they needed 19 patients in the study overall. The median GA of the infants was 25 weeks (IQR 24-28) with a BW of 685g.
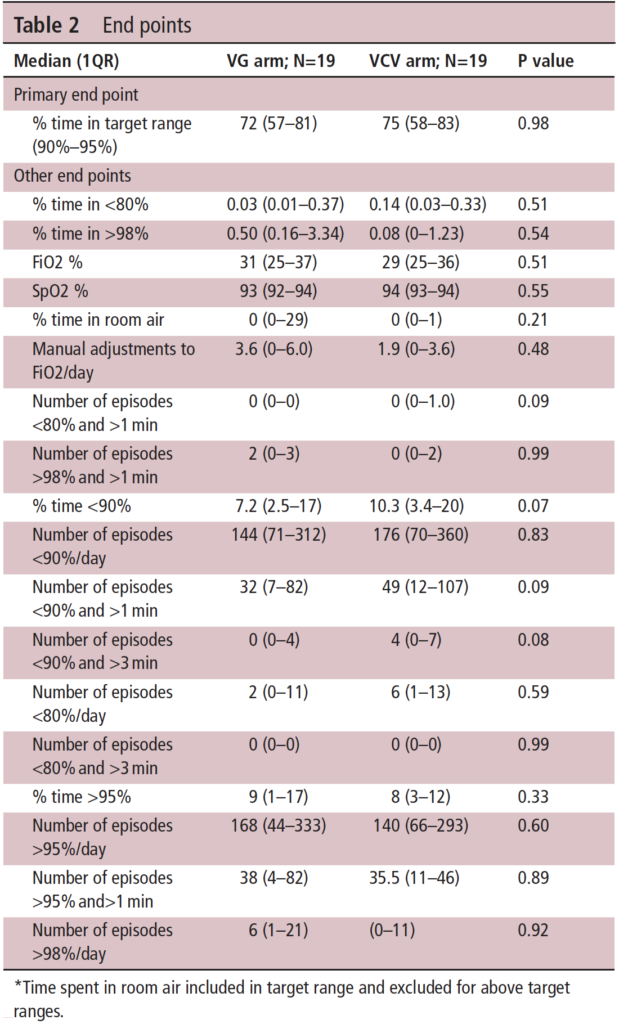
The results demonstrate at the top of Table 2 that the primary outcome was no different at all. Basically whichever mode you choose will work just fine when used with automated FiO2 control to keep the saturations in the target range. If there is anything that the study suggests though is that the percentage of time below 90% may be worse with VCV than VG. You get this from looking at the table and looking at the secondary outcomes. A word of warning though that since the study is small (very small) it is really difficult to take too much stock in the secondary outcomes as the study wasn’t powered to detect such differences. One can’t help but wonder though if that trend might have become a one of significance if the numbers in the study were greater. Is there biological plausibility for this? Looking at the two modes, it would appear that VG by adjusting each breath based on the last expired tidal volume may be more agile. If you believe the hypothesis that tighter control of alveolar ventilation by delivering better ventilation is key to reducing time outside the target ranges then it makes some sense that this mode would be better.
On a personal note, I use only VG in my centre so I am pleased to see there is really no difference in the primary outcome but the trend in the secondary outcomes at least puts a slight smile on my face as well!
Who doesn’t love a good match up?! Supporting neonates in need of resuscitation after delivery has been the subject of many studies over the years. The movement has certainly been to non-invasive support with CPAP or NIPPV but some babies need some degree of support with PPV after delivery when they simply won’t breathe. Prior to intubation the rise of the t-piece resuscitator has meant that practitioners can set a PIP and PEEP and with only a finger press to deliver a tidal volume at set pressure and with the finger released provide CPAP through the same device. The only problem potentially with use of these devices is the imposed work of breathing (iWOB) which has been measured in other studies. Any device I have used has provided ventilation through a mask so imagine my surprise to come across a new device called rPAP using prongs from the original infant flow design. From the manufacturers website the company claims that their design used with either a mask or nasal prongs reduces iWOB by 92% compared to other comparable machines! Imagine my greater surprise to see a head to head RCT comparing this new device to standard t-piece resuscitators with a mask.
The intervention was completed with one of three outcomes were met.
Infant intubated
Stable and breathing on method of support after a minimum of 10 minutes of support.
At 30 minutes when respiratory support could continue as decided by the clinician without crossover allowed.
Looking at the appendices for the trial it appears that one could use either device to administer PPV or CPAP but the point of the trial was that the devices would be used to support the infants until one of the three above criteria were met. If the claims about reduced iWOB were true compared to other devices in use then one might expect to see a difference in the primary outcome of incidence of intubation or death within 30 minutes of birth.
In total there were 250 infants recruited with 127 assigned to the rPAP and the other 123 to t-piece resuscitation. The mean GA in the trial was 24.8 weeks and the baseline characteristics between groups were similar although the group randomized to the rPAP has more c-sections and more general anesthetic exposure compared to the t-piece group. Lastly, humidification of gases during resuscitation was similar between the two groups.
How Did They Compare?
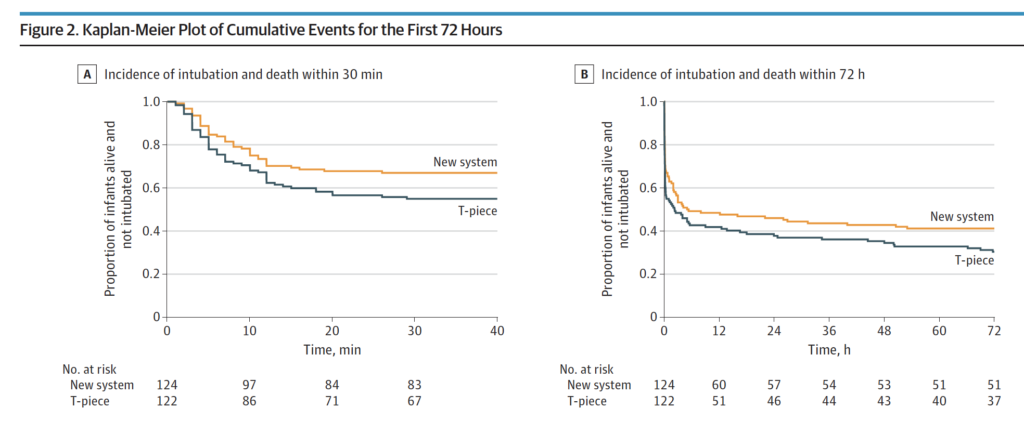
It just might be that the claims of decreased iWOB might have merit. In Figure 2 below the Kaplan-Meier curves show a difference favouring the rPAP device when looking at the primary outcome. This difference was significant with 41 of 124 infants (33.1%) in the rPAP group and in 55 of 122 infants (45.1%) in the T-piece group having the primary outcome of intubation or death within the first 30 minutes of life. Moreover when looking at the adjusted odds ratio it was still significant at 0.53; 95% CI, 0.30-0.94. The incidence of intubation and death in the first 72 hours although trending towards favouring the new system did not reach statistical significance.
Finally, none of the secondary outcomes reached statistical significance which included such things as death in the delivery room, use of surfactant, or PPV in the DR.
Does it make sense?
If you had asked me to tell you prior to the study whether resuscitation with nasal prongs vs a mask would be different I would have said a mask would be better due to less leak. Turns out based on this data that I would be wrong in that guess. A look at the website though for the rPAP device indicates that it can be used with a mask or nasal prongs. It would have been nice in the study presented here to have used a mask as a third arm with the rPAP device as it leaves me wondering a bit whether it was the interface that mattered more than the type of driver used? Maybe I am wrong and by using prongs it allows the infant to have less iWOB than with a mask over the mouth and nose? Could it be that it has more to do with that that the type of driver whether it is a traditional t-piece resuscitator or the new rPAP device? Regardless, I have a suspicion that these results will resonate with people. A posting of the abstract alone has garnered a lot of attention on twitter this week so clearly this is of interest.
I don’t think there is much fault to find in this study other than my question of why they didn’t choose to have a head to head comparison with masks as well but perhaps that is for another study. I imagine we will see this approach adopted in many centres around the world as they replace their traditional t-piece resuscitators in need of replacement. I also suspect there will be many that will want a larger study before adopting this strategy to look more closely with come faith in the results at secondary outcomes in particular having to do with safety.
One thing is for certain. There will be more studies to come!