When it comes to non-invasive ventilation the field has become a little more crowded in recent years at least in our institution. In the recent past if one decided to extubate an ELGAN the biggest decision was what CPAP pressure to use. These days we have the option of high frequency nasal ventilation (nHFOV) or non-invasive positive pressure ventilation (NIPPV) to choose from as additional options. Both of these modalities have their uses and I have written about nHFOV before as in Nasal High Frequency Oscillatory Ventilation For Preventing Intubation. On this post though I want to look at NIPPV which has actually been around longer as a modality. The gist of this mode is that one chooses a delta P, peep, Ti and rate much like you would on a conventional ventilator. When ventilating through a nasal interface the device provides ventilation although it is questionable I suppose how much of that is alveolar ventilation. The study we are going to talk about here caught my eye as the information gleaned from it gives me at least an idea of how this mode may work to help prevent reintubations.
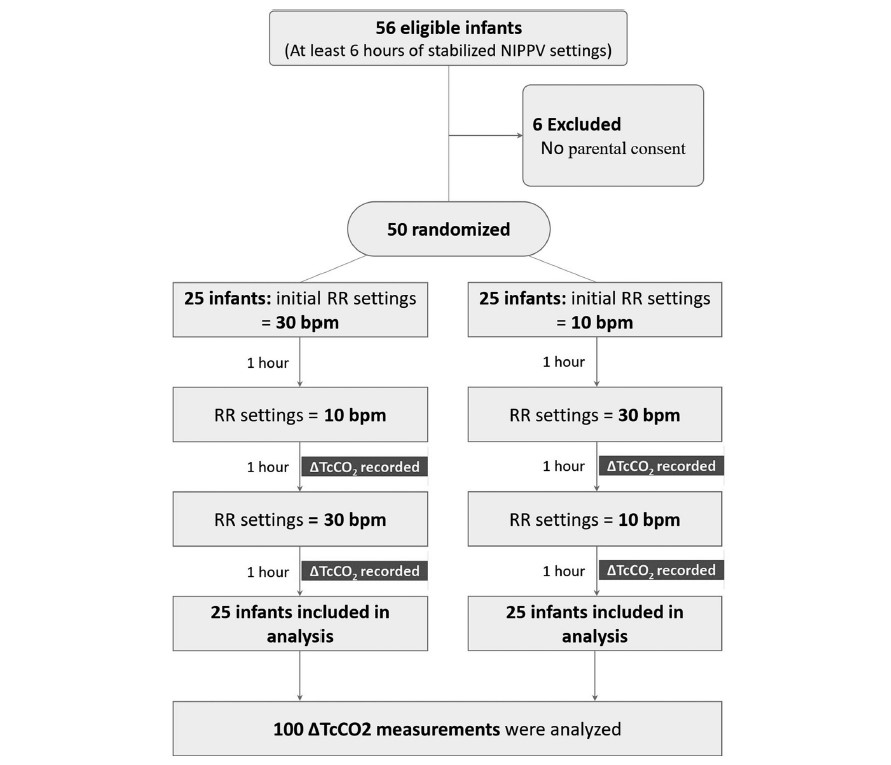
In this study each patient served as their own control and alternated between either a start of a rate of 10 BPM or a rate of 30 BPM as shown in the following diagram. The infants were all between 24 +0 and 32 +6 weeks gestation to be included in the study. Delivery of NIPPV was through the Leoni Ventilator using RAM cannulae and importantly the mode was non-synchronized. Each infant needed to be stable on their settings for at least 6 hours before being included. The authors hypothesis was that rate matters to clear carbon dioxide. To monitor CO2 levels they used transcutaneous CO2 measurements to allow for continuous measurement over each hour of the study. Given this belief, there was safety built into the protocol such that patients were excluded if on the set rate of 10 bpm the tcCO2-related pCO2 was <40 mmHg, or on NIPPV if the set rate of 30 bpm had a tcCO2-related-pCO2 is 60 mmHg, In other words, if rate matters and your tcCO2 was already less than 40 on a low rate then it would not be safe to blow off more CO2 and vice versa with high CO2 and low rates. To ensure that only rate affected the results “during the 3 h of the study no changes in PIP, PEEP or FiO2 were allowed with the following exceptions: if spO2 was <90% or >95% for more than 20 s, an increase or decrease in FiO2 were allowed to keep spO2 90–94%, and were documented”.
So does rate matter?
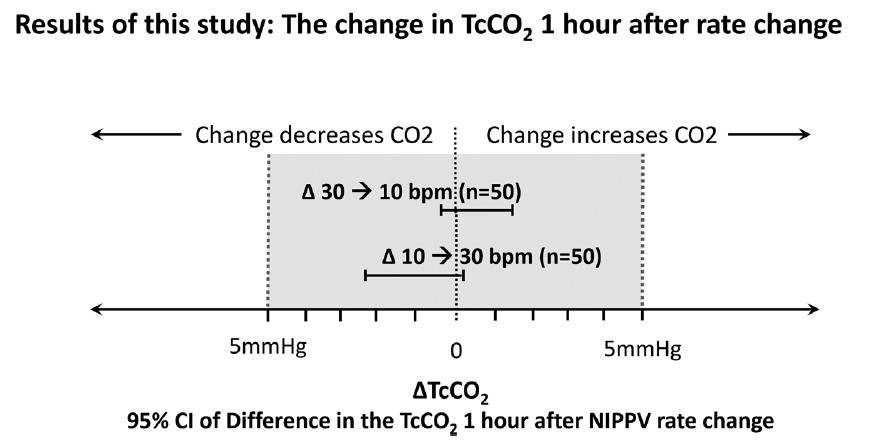
It turns out the authors found no difference in CO2 levels based on rate changes alone.
This of course is contrary to what the authors expected to find. The question is why this might be. What follows now is just speculation on my part but given the finding of no difference I can offer a few thoughts. The first is that NIPPV does not involve a distal delivery of gas like the situation of an endotracheal tube near the carina. With an endotracheal tube in place the delta P or pressure above the set peep is delivered to the gas exchanging areas of the lung. With NIPPV you are delivering the pressure at the nose and therefore there is a fair amount of dead space in between the exit of the gas into the baby and the lung. Might you just be really ventilating dead space for the most part?
Secondly, depending on the fit of the mask or the degree that the mouth was open how do we know how much of the non-invasive ventilation reached the infant? Lastly, in our own centre we have not been impressed with the RAM cannulae as we have found that whether the prongs are in or out of the nose the pressure being detected as being delivered seems to stay the same at least as the ventilator sees it. If the prongs were not in the nose properly and the atmosphere was being ventilated would one really know that the pressures weren’t really getting into the nose?
Lastly, the Leoni ventilator is not capable of delivering synchronized NIPPV. Now that there is the availability of synchronization on ventilators such as on the Puritan Bennett 980 ventilator it would be interesting to see the same study done again. If you are delivering non-synchronized breaths which are not in sync with the patient should we expect a change in CO2? What if half the breaths for example by chance are delivered on exhalation? Not much effect on CO2 I would think.
I am not saying that rate doesn’t matter at all but I suppose I am saying within the context of this study it doesn’t matter to CO2. My best guess as to how NIPPV works to prevent reintubation may be secondary to two things. The first would be by irritating the baby with the puffs of delta P. Think of it like intermittent stimulation. The second possibility is that the same puffs of air help keep the pharynx open and minimizes the obstructive portion of apnea of prematurity. Whatever the reason NIPPV appears to work to prevent reintubation in some infants!
I have no doubt the group here will look at the effect of delta P on CO2 soon enough and I wonder if we will see much difference there either. It also will be important to look at the effect of rate in a synchronized fashion! Time will tell.
Over the last number of years clinicians have sought more and more to limit the experience of babies to painful stimuli. In the area of surfactant administration this has focused on “less invasive” strategies such as use of small catheters while on CPAP (LISA or MIST) and surfactant via LMA or Surfactant Administration Through Laryngeal or Supraglottic Airways (SALSA) as it is sometimes known. Intubation Surfactant Extubation (INSURE) while not generally included in the less invasive approach is to a degree fitting since it involves at least intubating for a very brief period after surfactant is administered. SALSA has been growing in popularity due to its “extreme” non-invasiveness since babies are receiving surfactant without instrumentation of the airway at all. It should come as no surprise then that head to head comparisons will be done to determine which should be reigned king!
The Contenders
A group out of Albany, NY has looked at SALSA vs INSURE before in which they used morphine for premedication prior to the procedure. You might ask why any premedication is needed at all but I would suggest that covering one’s airway and dripping liquid into it might cause some irritation so why not keep them calm. The authors in their paper Randomized trial of laryngeal mask airway versus endotracheal intubation for surfactant delivery found a high rate of failure in the intubation arm which more than likely was attributable to the respiratory depressive effect of the same.
This time around in the current paper Randomized Trial of Surfactant Therapy via Laryngeal Mask Airway Versus Brief Tracheal Intubation in Neonates Born Preterm they switched to remifentanil for its brief duration of action. Babies in the SALSA arm received that drug while those in the ETT group received atropine as well. The authors included infants born from 27 weeks to 36 weeks gestation who were larger than 800g at birth. This was a non-inferiority trial with the primary outcome being Our primary outcome was failure of surfactant therapy to prevent the need for invasive mechanical ventilation or its surrogate indicators, namely, more than 2 doses of surfactant therapy, sustained need for FiO2 >0.60 to maintain target O2 saturations, or a second dose of surfactant within 8 hours of the first dose.
Surfactant redosing criteria were the same for both groups: FiO2 >0.60 or FiO2 >0.30 with clinical signs of worsening RDS. If surfactant needed to be given a second time it was via intubation. The decision to ultimately intubate though was in the hands of the practitioners.
Unfortunately, the trial was stopped after only 51 patients were enrolled into the LMA and 42 into the INSURE groups respectively. Randomization was by block design and the authors were looking for 130 patients per group so they fell far short of that. The reasons for falling short were interesting as they demonstrate one of the challenges of research and changing beliefs. At the start of the trial there was equipoise among practitioners with respect to the two modes of surfactant delivery but part way through people preferred SALSA. The authors changed the randomization to try and deal with that to a 2:1 favoring SALSA but with the combination of that and COVID they had to stop. They did manage to get enough though to determine the primary outcome in spite of this.
What did they find in the end?
Well first of all it is worth noting that there were no differences in baseline characteristics between the two groups. As it turns out, while the numbers were small it didn’t seem to lead to an unbalancing of groups.
With respect to inferiority the finding was that it was in fact not inferior as per the figure below.
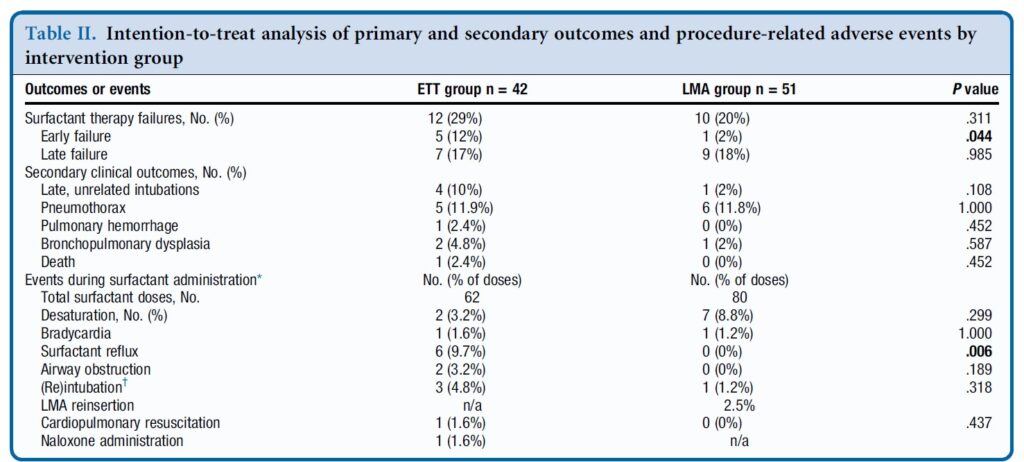
In table 2 some interesting findings emerge
Early failure of surfactant which was defined as within 1 hour of surfactant administration was found to be significantly increased in the intubation group. Late failure through at 5 days of age was not any different. An early failure is suggestive of the procedure not working to deliver the surfactant. When you look at the bottom half of table 2 the answer may be there. As part of the planned procedure the authors aspirated a gastric tube after surfactant administration to ensure that it went to the right place. There was no difference in surfactant volume aspirated via this route. There was however 9.7% of infants in the ETT group that experienced reflux in the ETT vs zero with observed reflux in the SALSA group (in the mouth perhaps?). Is surfactant without PPV better tolerated maybe?
There was a trend overall to more failures in the ETT arm although this was not found to be significant either in the intention to treat or per protocol analysis.
Where do we go from here?
First off it is important to look at who was chosen for this strategy. You may have noticed that there were no micropreemies in this trial. The reason for this is likely two-fold. The first is that prior trials on SALSA have found it doesn’t work as well to prevent intubations in babies below 27 weeks. This is very similar to the findings of studies using aerosolized surfactant. It may well be that there just isn’t enough of the total dose getting to the alveoli. If you can get some of the dose in deep into the lung for those with less severe RDS it may work ok for those babies. The second reason likely has to do with using LMAs in those in that weight range as they generally are designed for larger preemies although I understand smaller ones are becoming more readily available.
The second point is that this was not a blinded study. This could have become an issue as the authors acknowledge that there was a growing institutional preference for SALSA as the study went on. If the Neonatologist subconsciously believes it is better, might that have influenced some of the decisions to intubate again since one of the criteria was “clinical signs of worsening RDS”. It is quite possible this could have led to a few more intubations in the INSURE group for repeat doses. We can’t prove that but it is a weakness of the study.
At the very least it can be argued that the use of SALSA works as a small percentage overall failed the procedure. The largest groups of infants though were above 29 weeks so we also might not expect a high rate of failure after one dose though. It works but how well is tough to say.
Where I think this study is really important though is what it tells us for centers in particular who don’t intubate as often. Intubation is a skill that is declining in opportunity, both because of a turn to more use of non-invasive support as a primary mode of treatment. It also has become scarcer at an individual level due to there being more practitioners who can perform the skill. Having an option to use SALSA for those who aren’t as comfortable with intubation will no doubt be of much interest to many in this situation.
What is no doubt going to come next is the LISA/MIST vs SALSA trials. I hope that in the future pain scores are included in these sorts of analyses to really determine if in being less invasive we are also ensuring that we are also not undertreating discomfort. I suppose the lesson being learned from all of this is that less very well may be more.
I couldn’t think of a better topic for World Prematurity Day 2021 than what constitutes the edge of viability. Thinking back over my career, when I was a resident and fellow infants born at 25 and 26 weeks were deemed about as low as “we should” go but we certainly resuscitated infants at 24 weeks but this was considered heroic. Jump ahead to the last decade and we began caring for infants at birth at 23 weeks so commonly that the thought of offering comfort care only to infants at 24 weeks became almost unthinkable for many health care providers. Before I get jumped on, let me say that I am not saying I agree or disagree with that sentiment but it is something that is felt by many.
The Shared Decision Model
In the last few years a rethink again has occurred whereby the concept of the treating team knowing best has been replaced by the “shared decision model”. In this line of thinking, it is not up to us as health care providers to “tell the parents” what to do but rather come to a shared decision based on an assessment of the wishes and values of the parents in conjunction with hearing about both short and long term problems their infants may face if resuscitated. This concept was central to the statement by the Canadian Pediatric Society that I am proud to have been part of with respect to its development. The statement for those that are interested is Counselling and management for anticipated extremely preterm birth
What’s next? Going below 22 weeks?
The challenge of the shared decision model is that there comes a point where the answer is simply “no”. If for example a family at 19 weeks gestation demanded an attempt at resuscitation I would have to inform them that survival is not possible (assuming ultrasound confirmed anthropometric measurements consistent with that age). The question though becomes a little more difficult to answer at 21 weeks and was the subject of a recent article in the New York Times about a survivor at 21 weeks gestation.
Even with the best gestational age dating the estimate can be off by up to 5 days so it’s possible that the infant in this story was closer to 22 weeks or even midpoint between 22 and 23 weeks in reality. Regardless it does raise the question about what to do at 21 weeks and I suspect we will begin to see more stories about this now that the glass ceiling of 22 weeks has been breached. What about below 21 weeks? Sounds impossible I know but with research that remains at the stage of animal studies this may become possible. Maybe not in the next 5-10 years but it could happen in my lifetime in this chosen field.
The Artificial Placenta
This made headlines a few years ago with the news that the Children’s Hospital of Philadelphia had successfully kept a lamb alive for a period of 4 weeks using an artificial placenta and amniotic fluid.
You might think that this was a one-off experiment that will never see the light of day but similar work is being done in Toronto, Canada where they have been able to do similar work with preterm piglets in their paper Achieving sustained extrauterine life: Challenges of an artificial placenta in fetal pigs as a model of the preterm human fetus. Incidentally as my colleague Dr. Ayman Sheta worked on this project while in Toronto I am particularly pleased to share this research. Similar to the experience in CHOP the team in Toronto has been able to keep piglets alive for progressively longer durations. My understanding is that despite the best efforts infectious complications over arise limiting how long one can sustain such animals.
This leads me to my final thoughts on where we might be able to go. I see a future where we apply such technology to humans but not in the way that people might have thought. Keeping a fetus after delivery at 21 or 20 weeks on an artificial placenta for many weeks is not likely a realistic goal. What if we could get 1 or 2 weeks though and allow the fetus to be oxygenated without using positive pressure on their developing lungs and transition them at 23 or 24 weeks gestation? We may in this way be able to allow for postnatal maturation in a artificial uterine environment and give babies a chance who would otherwise never had the opportunity for a shared decision with medical staff.
Sound like science fiction? Well the beauty of the internet as my friend told me today is that once it’s out there it out there for good. Let’s see how this post stands the test of time and to all the babies out there in NICUs and to their families I wish you all a good and uneventful World Prematurity Day wherever you may be!
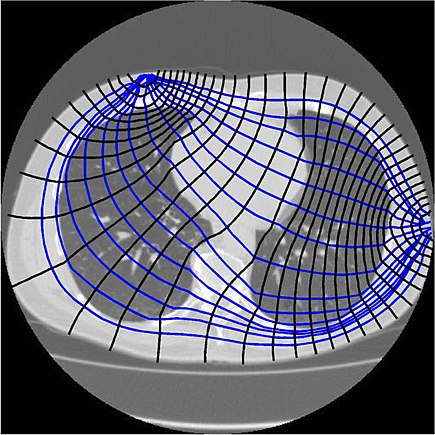
Extubation is a regular occurrence in the NICU. We do our best to predict who will succeed and who will fail but it isn’t always easy to figure out who they are in advance. We use techniques such as looking at oxygenation histograms and using thresholds for PIP, PEEP or MAP but in the end sometimes it works and other times it doesn’t. In an effort to improve on intubation success, some creative researchers in Switzerland employed a technique called end-expiratory lung impedance or EELI to measure lung volume before, during and after the extubation process. The use of EELI is based on the impendance of the lung changing with the distribution of tissue and air and by placing electrodes one can generate a cross sectional volume that has been shown in neonates to be representative of total lung volume. The EELI technique creates an image like this which is use to generate the estimate of lung volume.
The researchers in this study were seeking to do a quality improvement project and use EELI to estimate lung volume at different time points in an extubation. The time points were all 30 seconds including, immediately before first handling of the infant (baseline), tracheal suctioning (suction), start and end of adhesive tape removal (adhesive tape begin and adhesive tape end), pulling the endotracheal tube (extubation), initiation of non-invasive ventilation (NIV), immediately before and after turning the infant to prone position (supine and prone, respectively), and 10 min after turning to prone position (prone10). As per unit policy all babies were ventilated with Draeger VN500 ventilators and if <28 weeks went on to NIPPV when extubated or if 28 weeks or more straight CPAP. The purpose of this quality initiative was to determine using EELI at what point in the extubation process infants might be losing lung volume and then based on the information see if they could ultimately use this to improve the chances of successful extubation in the future.
What makes this study interesting is that the infants were found to lose volume but at a time when I would not have expected it.
The Reveal
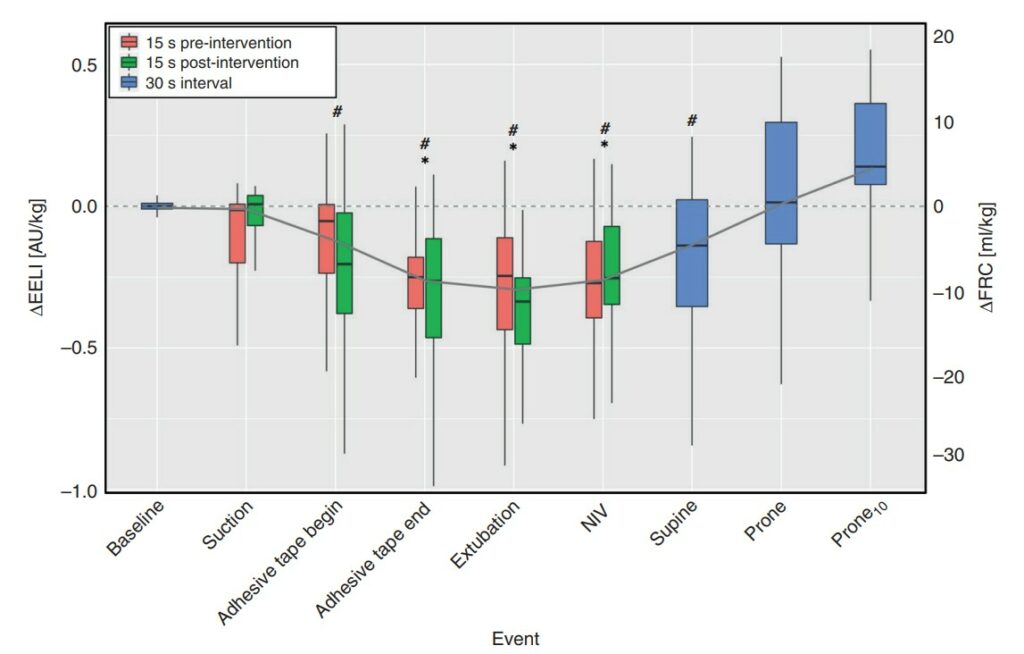
Below is a graphical depiction of EELI and estimates of FRC during the different time points. The changes in electrical impedance by EELI were converted on the right Y axis to an FRC in mL/kg.
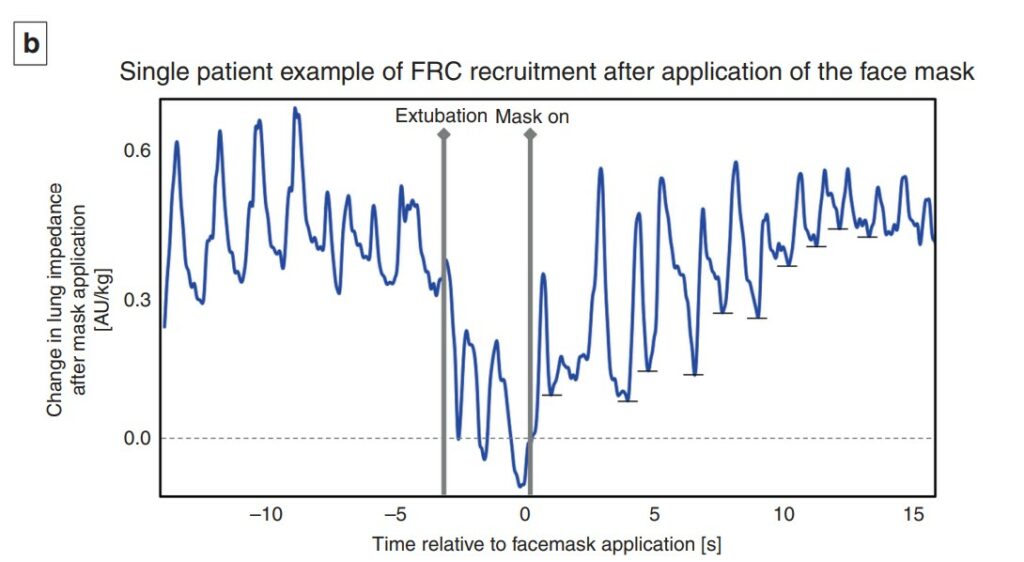
What is surprising at least to me here is the loss of volume occurs not with extubation but rather when the tape removal process happens. With the placement of the prongs on the infant at extubation the FRC gradually rises and recovery occurs. Moreover as shown in the 12 patients included in this study, the recovery once non-invasive ventilation is provided is quite rapid and evident within 1-2 breaths.
A couple other things to note. The loss of FRC during tape removal was about 10 mL/kg and if typical FRC in a preterm infant is 20-25 mL/kg you can see the impact this would have on lung volume and reserve. As this was a small study it could not detect a threshold at which extubation would fail but one infant who developed a pneumothorax and required reintubation did not get back to their baseline FRC.
What is this signaling?
Yes this is a small study but it did look at about 3000 breaths so there is a fair amount of data to look at. What the paper demonstrates I think is that there is a vulnerable time during tape removal where likely due to the fact that we use uncuffed ETTs in neonatology it is possible for these infants to lose lung volume. It may be that as they strain and bear down the ventilator may not be as effective at delivering volume to them. Measures that might help during this time could be skin to skin care, breastmilk drops or scent, sucrose or a variety of other non-pharmacologic measures to keep them calm. This might help to minimize such volume loss. Secondly, knowing the significant risk of volume loss it underlines the importance of placing nasal prongs on as quickly as possible during the transition from invasive to non-invasive ventilation as recovery of lung volume is possible. It think it also suggests that if we are “peepaphobic” and use an insufficient amount of support at extubation these infants may be vulnerable to experience significant volume loss as well.
While EELI may not be perfect, this study is the first of its kind and may shed some light into why some infants fail after extubation. While usually I say less is more, I do wonder if in the case of extubation, this study gives some evidence to support starting with a higher PEEP than you think you need non-invasively and then backing off after one has successfully extubated. This may be the first study I have seen on this but I am certain it won’t be the last.
The journey from conception to the labour floor and then for some to the NICU is not a straight one. There are times of joy, interspersed with sadness, denial, anger and eventually acceptance, as initial news of being pregnant leads to complications in pregnancy and then eventual admission of an infant to the NICU.
Much has been said in recent years about the building of partnerships with parents and in fact there is a new catchphrase attached to the concept “shared decision making” (SDM). There is no question that in the perfect world this is exactly the relationship that we should be striving for with all of our patients. The world however is not perfect and although this may not be the most popular opinion I have given, I question how applicable this really is in many situations.
A Reality Check
Take for instance the parents who present to the labour floor of their local hospital in advanced labour at 24 weeks. Proponents of this SDM model would suggest that a meeting take place and pertinent information be given to a family and together with the assistance of literature applicable to their situation (possibly a pamphlet) the health care providers and families come to a mutually agreeable decision as to what the best course of action is for them and their unborn infant. This all sounds wonderful but examining the real life situation a little more closely is it actually reasonable to assume we can obtain this? I have not been, nor will I ever be pregnant and certainly have never experienced contractions and felt the veil clouding my vision as the first dose of analgesia enters my veins to deal with the discomfort a woman experiences during labour. Not to mention there are people admitting this couple, taking histories, establishing IV access, scanning bellies and a whole host of other pokes and prods along the way.
My Role Better Defined
Then I come in. Among all this chaos I deliver the information, pass along a pamphlet and do the best job I can to inform said couple of the upcoming decision. The trouble of course is how do we come to this mutual decision in the 15 – 30 minutes I spend with them during this crisis? The answer sadly is we do our best but don’t for a minute think that SDM has occurred. I don’t believe this is possible unless the family has prior experience with a preterm birth or perhaps is a HCP working with newborns or children with disabilities themselves. In fact Boss RD et al in their own research on the subject identified that in hindsight religion, spirituality and hope are what motivated parents rather than what was said at the time. In essence their minds are already made up. It doesn’t mean we shouldn’t strive for the SDM but at least in my opinion, unless their contractions settle, a calmness ensues, they have time to digest the information being given and then meet again under less stressful circumstances, the SDM is a nice idea but for many not a reality.
Shifting To The NICU
I recall a significant moment in my training when I saw how the SDM model can actually cause more grief than help. Dr. Keith Barrington a fellow blogger (if you haven’t discovered him, his work is fascinating over at Neonatal Research) published one of the most impactful pieces of research of the decade during my fellowship. The adverse neuro-developmental effects of postnatal steroids in the preterm infant: a systematic review of RCTs. Following this analysis there was a near moratorium on the use of post natal steroids. The issue this created was that to now receive them you had to be close to the end of the limits of care. At this point you either died (thereby concluding they are of no help) or you survived with disability that was due in part no doubt to how sick you had become (thereby concluding they are dangerous).
The moment I am referring to was a conversation with a family in which the attending managing the unit presented the risks and benefits of postnatal steroids to the family when the FiO2 was at 40% one day. The language used was non directive and the parents asked for another day to decide. The next day and each of the following two days they were unable to choose between giving the steroids and the perceived risk of brain damage versus not and watching the FiO2 climb by about 10% per day. By the time the FiO2 several days later was at 80-90% they were distraught, teary and feeling helpless. What they needed was direction; someone to give them some advice or more simply an educated opinion.
We can strive to share in the decision making but I continue to believe there is a time and place to help our families by taking a stance or side. We can equip them with as much information as we want but is there really any replacement for actually taking care of these infants, experiencing the ups and downs and hearing how they have done in follow-up? We simply can’t expect the average parent to understand the true long term consequences of their decisions. I am not saying we go back to a paternalistic time in medicine but I am saying that one size does not fit all.
We owe it to our families to pursue SDM when we can but we have an equal obligation to recognize when this ideal state is simply not possible. At this point we have to use the experiences and knowledge we have to provide them with the best advice we can. We have gone through medical training, and gone down these paths so many times. We can avoid biased opinion and rely on the facts as they are in our institutions but to not take a stand when it is needed at least for me is doing a disservice to those we are so eager to help.








 I am not saying we go back to a paternalistic time in medicine but I am saying that one size does not fit all.
I am not saying we go back to a paternalistic time in medicine but I am saying that one size does not fit all.