The journey from conception to the labour floor and then for some to the NICU is not a straight one. There are times of joy, interspersed with sadness, denial, anger and eventually acceptance, as initial news of being pregnant leads to complications in pregnancy and then eventual admission of an infant to the NICU.
Much has been said in recent years about the building of partnerships with parents and in fact there is a new catchphrase attached to the concept “shared decision making” (SDM). There is no question that in the perfect world this is exactly the relationship that we should be striving for with all of our patients. The world however is not perfect and although this may not be the most popular opinion I have given, I question how applicable this really is in many situations.
A Reality Check
Take for instance the parents who present to the labour floor of their local hospital in advanced labour at 24 weeks. Proponents of this SDM model would suggest that a meeting take place and pertinent information be given to a family and together with the assistance of literature applicable to their situation (possibly a pamphlet) the health care providers and families come to a mutually agreeable decision as to what the best course of action is for them and their unborn infant. This all sounds wonderful but examining the real life situation a little more closely is it actually reasonable to assume we can obtain this? I have not been, nor will I ever be pregnant and certainly have never experienced contractions and felt the veil clouding my vision as the first dose of analgesia enters my veins to deal with the discomfort a woman experiences during labour. Not to mention there are people admitting this couple, taking histories, establishing IV access, scanning bellies and a whole host of other pokes and prods along the way.
My Role Better Defined
Then I come in. Among all this chaos I deliver the information, pass along a pamphlet and do the best job I can to inform said couple of the upcoming decision. The trouble of course is how do we come to this mutual decision in the 15 – 30 minutes I spend with them during this crisis? The answer sadly is we do our best but don’t for a minute think that SDM has occurred. I don’t believe this is possible unless the family has prior experience with a preterm birth or perhaps is a HCP working with newborns or children with disabilities themselves. In fact Boss RD et al in their own research on the subject identified that in hindsight religion, spirituality and hope are what motivated parents rather than what was said at the time. In essence their minds are already made up. It doesn’t mean we shouldn’t strive for the SDM but at least in my opinion, unless their contractions settle, a calmness ensues, they have time to digest the information being given and then meet again under less stressful circumstances, the SDM is a nice idea but for many not a reality.
Shifting To The NICU
I recall a significant moment in my training when I saw how the SDM model can actually cause more grief than help. Dr. Keith Barrington a fellow blogger (if you haven’t discovered him, his work is fascinating over at Neonatal Research) published one of the most impactful pieces of research of the decade during my fellowship. The adverse neuro-developmental effects of postnatal steroids in the preterm infant: a systematic review of RCTs. Following this analysis there was a near moratorium on the use of post natal steroids. The issue this created was that to now receive them you had to be close to the end of the limits of care. At this point you either died (thereby concluding they are of no help) or you survived with disability that was due in part no doubt to how sick you had become (thereby concluding they are dangerous).
The moment I am referring to was a conversation with a family in which the attending managing the unit presented the risks and benefits of postnatal steroids to the family when the FiO2 was at 40% one day. The language used was non directive and the parents asked for another day to decide. The next day and each of the following two days they were unable to choose between giving the steroids and the perceived risk of brain damage versus not and watching the FiO2 climb by about 10% per day. By the time the FiO2 several days later was at 80-90% they were distraught, teary and feeling helpless. What they needed was direction; someone to give them some advice or more simply an educated opinion.
We can strive to share in the decision making but I continue to believe there is a time and place to help our families by taking a stance or side. We can equip them with as much information as we want but is there really any replacement for actually taking care of these infants, experiencing the ups and downs and hearing how they have done in follow-up? We simply can’t expect the average parent to understand the true long term consequences of their decisions. I am not saying we go back to a paternalistic time in medicine but I am saying that one size does not fit all.
We owe it to our families to pursue SDM when we can but we have an equal obligation to recognize when this ideal state is simply not possible. At this point we have to use the experiences and knowledge we have to provide them with the best advice we can. We have gone through medical training, and gone down these paths so many times. We can avoid biased opinion and rely on the facts as they are in our institutions but to not take a stand when it is needed at least for me is doing a disservice to those we are so eager to help.
As the familiar saying goes, “when the U.S sneezes Canada catches a cold”. This post will be the most political one I have ever written I suppose but before I get too far into it let me say that I do not intend to write a pro or con piece about the President of the United States. What I do intend is to alert you all to a very interesting trend that occurred in the months following the election in November 2016 of Donald Trump.
A Shocking Result
It is fair to say that the election provided the US with a right leaning president and also fair to say that in Ontario the political leanings tend to be more to the middle or left of centre. When you have that disparity it could lead to stress in such left leaning areas of the Province as people would begin to worry about the impact of right leaning policies on their fortunes. Prior work had noted that in times of significant stress the ratio of male to female births can be affected. Interestingly on average there are almost always slightly more males born than females. Many theories abound as to why this might be with one theory being that we males fetuses tend to be more fragile (some women would say this is for life) so we need more of us to start in order to balance the population out. As seen in global catastrophes such as war this ratio can move closer to 1:1 for a period of a few months after the significant event but then recovers a few months later.
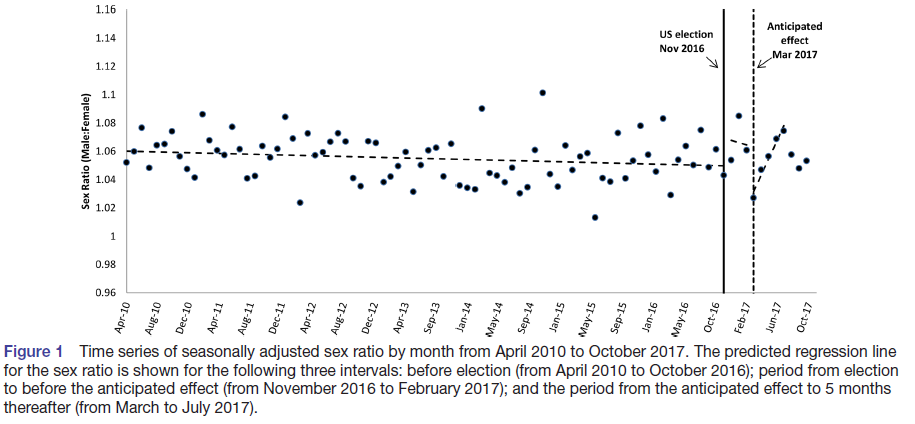
Study in Ontario
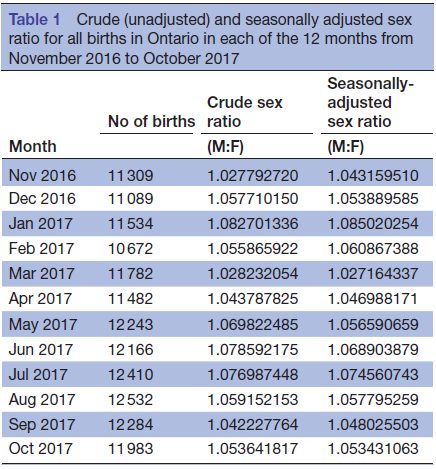
Outcome of the 2016 United States presidential election and the subsequent sex ratio at birth in Canada: an ecological study was published this year by Retnakaran and Yi using the Better Outcomes Registry & Network (BORN) in Ontario to capture data on birth ratios from 2010 to 2017. The authors were able to control for birth seasonality and looked at the change in birth ratio in left leaning health regions in particular between the months leading up to the election in November 2016 and then the 12 months afterwards. Their findings I found fascinating and like much research probably creates further questions. As has been seen in other situations like this a trough in the ratio occurred about 5 months after the election. A gradual but consistent increase in the ratio back to baseline came about close to 6 months later. This effect is seen in the figure below demonstrating that on the far right of the graph recovery was brisk and unidirectional. In the end it would appear that much like previous psychologically dramatic situations the impact in Ontario with a markedly different political viewpoint than their neighbours to the south had a similar effect.
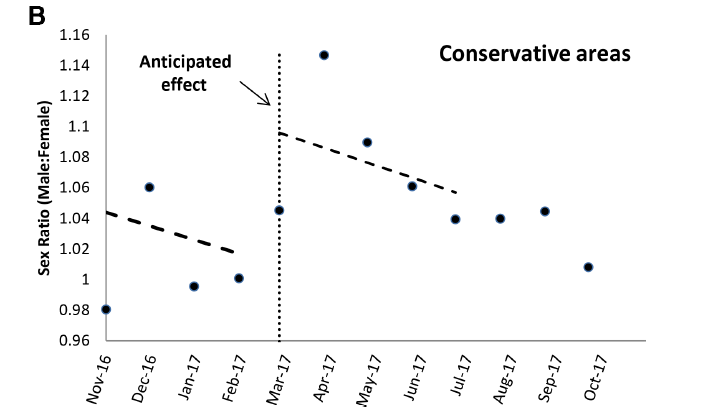
Perhaps equally interesting is what happened in right leaning health regions with respect to birth ratio. No increase in ratio was seen in the months after the election. The trend was really reversed as shown below.
The Next Question is Why and How?
The answer to this question is likely a sad one that at this point is speculative. Five months after the election the die was cast so to speak as women were already pregnant so the answer cannot be that people were having less pregnancies or selecting out female fetuses through IVF. The most likely answer is that there was an disproportionate loss of male fetuses after this political moment in history. We teach often in medicine that the female sex is the stronger one and it is for this reason that in times of trauma the male fetuses might be expected to be lost in a higher frequency than female.
I can’t help but think if people knew of this phenomenon and could anticipate that it could happen that an opportunity for intervention would exist. Maybe the next time an election involves such polarizing candidates (such as now) part of the antenatal visit could be reminding families about programs for grief counseling or help with stress relief. I have to confess I had no idea this phenomenon existed but I must confess I am sold that it is real and if fetal loss is a risk there is something that we can do before the next US election and help maybe save a few lives along the way.
The benefits of antenatal steroids before preterm birth have been clearly demonstrated in the literature and have been nicely summarized in a Cochrane Review. From this report the evidence is clear. Treatment with antenatal corticosteroids prior to preterm birth is associated with an overall reduction in neonatal death (relative risk (RR) 0.69, 95% confidence interval (CI) 0.58 to 0.81, 18 studies, 3956 infants), RDS (RR 0.66, 95% CI 0.59 to 0.73, 21 studies, 4038 infants), cerebroventricular haemorrhage (RR 0.54, 95% CI 0.43 to 0.69, 13 studies, 2872 infants), necrotising enterocolitis (RR 0.46, 95% CI 0.29 to 0.74, eight studies, 1675 infants), respiratory support, intensive care admissions (RR 0.80, 95% CI 0.65 to 0.99, two studies, 277 infants) and systemic infections in the first 48 hours of life (RR 0.56, 95% CI 0.38 to 0.85, five studies, 1319 infants).
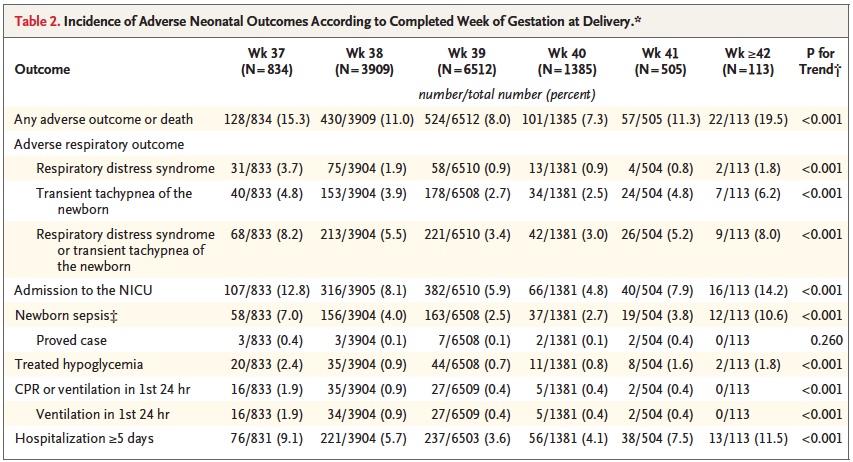
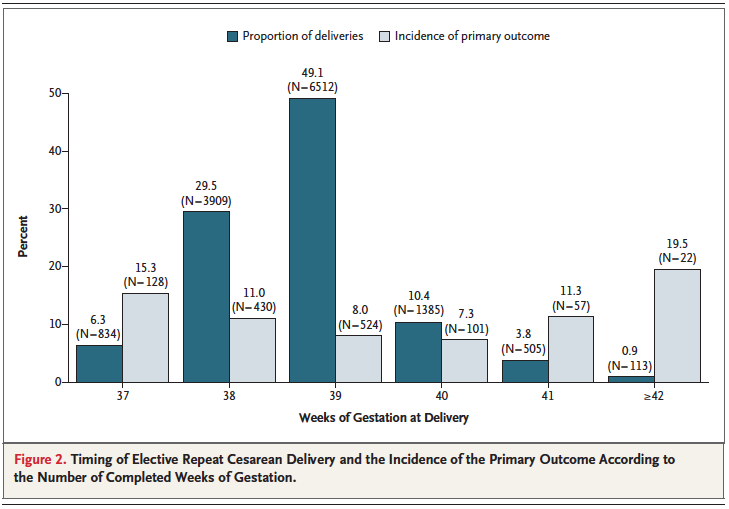
While it is clear that corticosteroid administration prior to 37 weeks has great benefit, the question is whether these benefits might actually extend to 37 and 38 weeks. It has been known for some time that having an elective c-section before 39 weeks exposes the infant to an increased risk of pulmonary morbidity and NICU admission. In 2009 Tita At et al studied 24077 repeat elective c-sections at term finding that 36% were performed prior to 39 weeks. The findings conclusively demonstrated that delivery at 37 and 38 weeks increased the likelihood of a composite outcome of death or respiratory complications, treated hypoglycemia, newborn sepsis and admission to the NICU. Interestingly one can also see that after 40 weeks these complications rose again. Post term deliveries are not without their consequences either.
Broken down by outcome, it is also clear that each component has an increased risk at both 37 and 38 weeks compared to delivery at 39 or 40 weeks.
With such increased risk this practice has been discouraged by many obstetrical organizations including the American College of Obstetricians and Gynecologists.
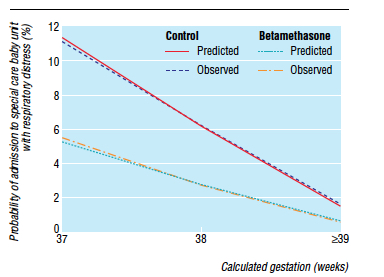
Knowing that there is clear benefit to providing corticosteroids before 37 weeks, it was only a matter of time before someone would test the hypothesis that treatment of women having an elective c-section in would reduce the incidence of respiratory complications such as TTN and RDS. Surprisingly there is really only one relevant study on this subject performed by P. Stutchfield et al in 2005 entitled Antenatal Betamethasone and Incidence of Neonatal Respiratory Distress After Elective Caesarean Section: A Pragmatic Trial. The trial provided betamethasone as a single course of two doses 24 hours apart starting 48 hours before a planned c-section with 998 participants in total.
The primary outcome in this trial was admission to NICU with respiratory distress. While the study was unblinded, the results were impressive and shown in the figure to the right indicating that below 39 weeks there was a significant difference in likelihood of admission for respiratory distress if women were treated with betamethasone prior to elective delivery via c-section. In terms of effectiveness this translates to the need to treat 37 women at 37-38 weeks with betamethasone to prevent one admission for respiratory distress to NICU. Eighty percent of the newborns in the control group had TTN versus RDS so I would expect you would need to treat about 200 women to prevent one case of RDS at this gestational age. Is it worth it? I suspect if you told parents that you could prevent hospital admission of their newborn at all many would choose to do so. There is another side to this though that one must consider and that side is the impact on neurodevelopment.
Corticosteroids work by overcoming the maternal capacity to break down cortisol by a placental enzyme 11β-hydroxysteroid dehydrogenase type 2 (11β-HDS-2). Furthermore the corticosteroids used (betamethasone and dexamethasone) are resistant to degradation by this enzyme. In the brain this enzyme exists as well and has increased activity such that levels of active cortisol in the brain are at a minimum. In animal models, high levels of glucocorticoids cause decreased brain differentiation with reduced neurogenesis. These processes are likely to be similar in humans given the presence of the same enzyme which has little effect in inactivating these synthetic medications.
Even with this knowledge, we as health care providers freely recommend antenatal steroids to women at risk of preterm birth for all the benefits outlined at the start of this post. Preterm infants are at significant risk of IVH, PVL, NEC, PDA and many other conditions which in and of themselves have been linked with adverse neurodevelopment. It is the avoidance of these outcomes which likely explains why corticosteroid administration with it’s known effect on the developing brain leads to improved neurodevelopmental outcome. The challenge here is that can we extrapolate this to the 38 and 39 week fetus? I would suggest that this is not the case as the risks of the conditions leading to neurodevelopmental impairment are magnitudes less. We are then exposing these fetuses to the potential harm or glucocorticoids without the benefit of reducing the conditions that matter to outcome. On the other side of the scale is a reduction in TTN/RDS and admission to the NICU but is it worth treating 37 mothers to avoid this with the heavy weight on the other side?
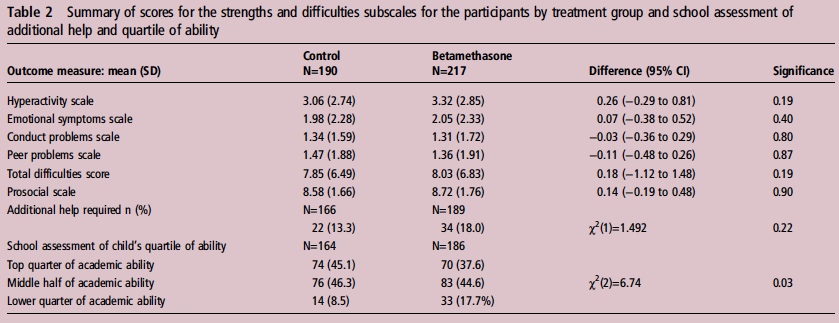
If you believe I am making some unfair assumptions it is worth seeing what happened to the patients in the 2005 study by Stuchfield when they were followed up between 8 – 15 years of age. The study used a questionnaire to address a number of outcomes related to education, atopy and behaviour. The response rate for the study was only 51% of the original cohort so any conclusions must be taken with a grain of salt. That being said the authors state that there were no differences in outcome or difference in rates of asthma and atopy. In their conclusion they affirm that based on the lack of differences in long-term outcomes but with improved short-term respiratory status at birth steroids should be provided before elective c-sections. Curiously though the authors do not address an interesting finding shown in table 2 from the article.
Looking at the bottom section pertaining to the school’s assessment of a child’s academic ability, less children in the steroid group performed at the top quarter of the class and twice as many children were in the lower quarter of the class. To me at least it seems disingenuous to claim no differences were seen when clearly here is a difference based on a third-party (the teacher) that is significant. The academic purists will be quick to point out that this is a secondary analysis and not the primary outcome specifically of the study and that the numbers are small. Additionally one can also argue that at a 51% response rate we are missing a great deal of outcomes. Furthermore it may well be that when it comes to surveys, those who have concerns about their participation in the study may be more apt to complete it skewing the results.
I will allow all these arguments as it really helps to support my conclusion on all of this. There is very little data out there on the benefit of providing antenatal steroids at term before elective c-section. The data out there for long-term effects does show a concern regarding school performance and the exposure in this case is to medication which is known to have effects on the developing brain. That data though is suspect as well given the issues raised in the above paragraphGiven the number of women that need to be treated to avoid one admission for respiratory distress and with the above mentioned concerns I believe more studies are needed to determine whether this is worth instituting as standard practice. Finally, any future studies will need to address in a prospective manner using a large number of patients whether there is indeed any impact on development in the long-term from such practice.
The story is the same. You and your partner find out that you will be expecting a newborn in the near future. You dream of what they might look like and dream about meeting them for the first time. In the case of the mother in this video that was not the case as she suffers from Macular Degeneration. A disease that typically affects people beyond the childbearing years but in her case afflicted her at an age way too soon.
Medical breakthroughs happen frequently and are wonderful to behold but this story caught my eye due to the impact of being able to restore something that we as parents hold so dear to us. To be able to view our beautiful baby with our own eyes. Thanks to an Ottawa company featured in the video this is now a reality for this mother.
As I sit and write this post with my beautiful children close by I can’t help but think how grateful I am to be able to take in their beauty. This is something I never questioned I would be able to do but for some no doubt this was a dream. The difference is that thanks to http://www.esighteyewear.com/ a Canadian company this is now a reality.
I am not an Ophthalmologist but I have no doubt that such eyewear will transform the quality of life beyond this case as Macular Degeneration is something that many unfortunately live with. If you know someone with MD you may wish to pass this along to them as it may change their life.
The answer to this question seems to be quite elusive! In 2009 the American Society of Obstetricians and Gynecologists published a recommendation to avoid elective delivery of infants < 39 weeks gestational age.
http://bit.ly/1JT84fm
Induction after 41 but before 42 weeks was advised, however due to the increased rates of complications after 42 weeks including mortality, asphyxia and complications of having a large infant to name a few. This was also supported by the Cochrane Review on the same topic that can be found here: http://1.usa.gov/1E2aq8a
The decision to avoid elective delivery prior to 39 weeks was secondary to many published reports demonstrating that such deliveries had a higher chance of having babies born with complications, the most likely of which was respiratory distress leading to increased rates of NICU admissions. That being said the incidence of asphyxia in the same group was lower than if one waited until a later gestational age.
Since that time, the recommendations have been to avoid these elective deliveries but a recent article has been receiving a lot of press that suggests we have it all wrong. Outcomes may be better if one delivers prior to 37 weeks.
In this study from Denmark (published Feb 18th in the British Journal of Obstetrics and Gynecology) an enormous sample of patients (832935) over a ten year period were studied to determine outcomes for each pregnancy when one compared elective delivery prior to 37 weeks with c-sections or planned vaginal birth. Despite an adoption in Denmark of the recommendations as outlined above from ACOG, the incidence of delivery prior to 37 weeks increased significantly. What makes this article so sensational is that during this time the number of NICU admissions decreased in this cohort delivered prior to 37 weeks vs the expectant vaginal births. Concurrently the risk of cerebral palsy decreased, large babies decreased and also less nerve injuries after birth but strangely with an increase in the incidence of shoulder dystocia. The original article abstract is found here: http://1.usa.gov/1MXaE2U
Before I go on I feel the need to state the obvious. As a man I have no idea what it is like to be pregnant although I do know that as women approach and then pass the 37 week mark of their pregnancy, many are enamoured with the idea of giving birth ASAP. I have no doubt there is an appeal to this research study explaining why so much press has been devoted to this paper. It suggests an action that many women I believe would be more than happy to accept but is it the right way to go?
The short answer is I don’t know for sure. The authors do a fairly good job of looking at variables that might have influenced outcomes such as maternal age, smoking rates, number of prior pregnancies etc but one has to question what variables may have influenced outcomes that were not measured? Looking at a massive number of patients gives a robustness to the results but it also means that you have collected a sample over a large period of time. Over a ten year period, practices can change, new technologies become implemented and new NICUs may be built all of which may account for an improvement in outcome over time. This is not to say that the authors are not on to something here but it does give one reason to pause and question how one study can have such a different result than many others that have come before it.
I think that the authors in this case took the right path and acknowledge at the end of the article that more work must be done in essence to confirm the findings. As a Neonatologist I am very interested to see if further work in the area will confirm these findings in a modern cohort.
If they do though will we have the capacity to deal with the increased number of admissions if it turns out they are wrong. Only time will tell.


 I am not saying we go back to a paternalistic time in medicine but I am saying that one size does not fit all.
I am not saying we go back to a paternalistic time in medicine but I am saying that one size does not fit all.
 Interestingly one can also see that after 40 weeks these complications rose again. Post term deliveries are not without their consequences either.
Interestingly one can also see that after 40 weeks these complications rose again. Post term deliveries are not without their consequences either.