Knowing when to extubate an ELBW is never an easy task. Much has been written about extubation checklists including such measures as mean airway pressure minimums and oxygen thresholds as well as trials of pressure support at low rates. The fact remains that no matter how hard we try there are those that fail even when all conditions seem to be met for success. The main culprit has been thought to be weakening of the diaphragm as the infant stays on the ventilator for longer periods of time. Specifically, myofibrillar contractile dysfunction and myofilament protein loss are what is occurring leading to a weakened diaphragm which may be incapable of supporting the infant when extubated even to CPAP. More recently in Neonatology the use of point of care ultrasound (POCUS) has gained in popularity and specifically use of lung ultrasound has helped to better classify various disease conditions not only in determining which disease is active but also following its course. Using POCUS to measure thickness and excursion of the diaphragm has been employed in the adult world so using it in neonates to determine extubation readiness seems like a logical next step.
An Observational Cohort Study
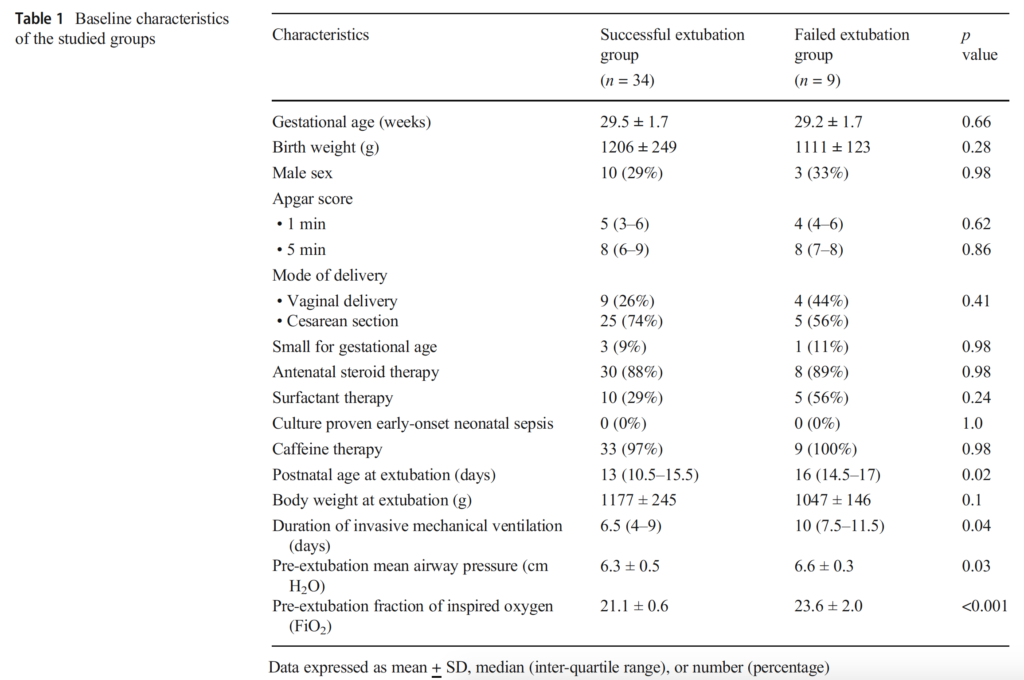
Bahgat E et al published Sonographic evaluation of diaphragmatic thickness and excursion as a predictor for successful extubation in mechanically ventilated preterm infants in the European Journal of Pediatrics. This small study sought to look at preterm infants born under 32 weeks and assessed a number of measurements of their diaphragm bilaterally including thickness of both during the respiratory cycle and the excursion (measured as most caudad and cephalad position during respiration). All patients underwent a similar process prior to extubation using PSV with a support of +4 over peep with measurements taken 1 hour prior to planned extubation. All infants met unit criteria for a trial of extubation based on blood gases, FiO2 and MAP being less than 8 cm H2O. All infants received a PSV trial for 2 hours before being extubated to CPAP +5. The sonographic assessment technique is laid out in the paper and the study end point was no reintubation in the 72 hours after extubation. The decision to reintubate was standardized as follows: more than six episodes of apnea requiring stimulation within 6 h, or more than one significant episode of apnea requiring bag and mask ventilation, respiratory acidosis (PaCO2 > 65 mmHg and pH < 7.25) or FiO2 > 60% to maintain saturation in the target range (90–95%).
Differences between the groups at baseline included a longer median day of extubation by 3 days, total duration of mechanical ventilation, higher mean airway pressure and FiO2 all in in the failure group.
Results of the study find a key difference in measurements
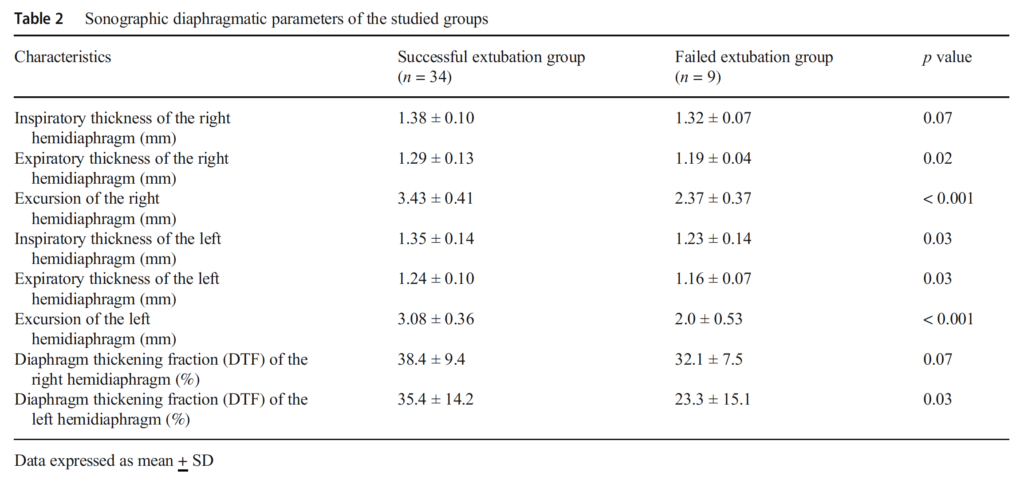
Looking at table 2 below the main finding of the study was that the biggest difference between those infants who succeeded and those that failed was the excursion of the diaphragm rather than the thickness. The greater the excursion the better the chance at successful extubation. In experienced hands the measurement does not take that long to do either.
As the authors point out in the paper:
“A right hemidiaphragmatic excursion of 2.75 mm was associated with 94% sensitivity and 89% specificity in predicting successful extubation. A left hemidiaphragmatic excursion of 2.45mmwas associated with 94% sensitivity and 89% specificity in predicting successful extubation”
Is this the holy grail?
There is no question that this technique adds another piece to the puzzle in helping us determine when it is safe to extubate. If I can pick one fault with the study it is the use of a pressure of +5 to support the extubated infants. If you look at the mean level of MAP the infants were on prior to extubation in the two groups it was 6.3 in the successful group and 6.6 in those who failed. By choosing to extubate the group that was already on a mean of about 24% to an even lower pressure level I can’t help but wonder what the results would have looked like if extubation occurred at a non-invasive level above that when they were intubated. Our unit would typically choose a level of +7 to extubate such infants to and avoid pulmonary volume loss so what would the results show if higher pressures were used (someone feel free to take this on).
One thing though that is borne out of all this however is that if diaphragmatic weakening happens in the neonate with prolonged ventilation as well it would be supported by the long length of ventilation in the failure group that also has less diaphragmatic thickness and excursion. What this study in my mind really says is that extubation should occur as early as possible. Every time you hear someone say “why don’t we wait one more day” you can now imagine that diaphragm getting just a little weaker.
As I said on a “tweet” recently “No one should brag about having a 100% extubation success rate”. If that is your number you are waiting too long to extubate. Based on the information here it should be a reminder that the plan for extubation needs to start as soon as the tube is inserted in the first place.
We hope to provide education through links to publications and videos demonstrating the benefits of adopting POCUS! Less ionizing radiation and enhanced diagnostic accuracy are just two of the benefits of using such techniques. Videos demonstrating and discussing this technique can be found on the Point of Care Neonatal Ultrasound Playlist on my Youtube channel
Background
Use of point of care ultrasound has expanded over the last decades particularly in intensive care to the point that it is now readily available for use by the clinical care practitioners in this setting (1). Today clinicians are using ultrasound at the bedside to assist in the evaluation of physiological abnormalities in a number of body systems. Ultrasound has been used to image body organs for over 50 years (2). It is currently the most widely used imaging modality in medicine. Advantages are that ultrasound is portable, free of radiation risk and relatively inexpensive compared to other diagnostic modalities like magnetic resonance and computed tomography (3). The main limitation when considering this for use by NICU clinicians is that it requires advanced training. In addition, when compared to traditional x-ray, ultrasound has limited penetration to air and bones and therefore structures deeper to them cannot be well assessed (4).
Indications:
There are three general indications for ultrasound in the neonatal setting:
1) Anatomic assessment of static organs such as the brain, lungs, liver, kidney and spleen to evaluate for anomalies, hemorrhage, space occupying lesions and abnormal fluid collections.
2) Dynamic assessment of moving organs, such as the heart, lungs, intestine, and the vascular system to evaluate blood flow and physiologic processes.
3) Locating vessels for cannulation and determining the position of catheter tips.
Anatomic ultrasound assessment of static organs should be provided by a trained radiologist. Dynamic ultrasound assessment can be performed by a trained neonatal clinician who understands the clinical details of his or her patients and is familiar with the underlying pathophysiologic mechanisms (5). Table 1 shows different applications performed by a trained clinician.
Point of care lung ultrasound:
In the last 10 years, research studies have shown that lung ultrasound (LUS) is an accurate, non-invasive method for predicting ventilatory failure and offers advantages over traditional chest radiography (6). LUS can accurately and reliably diagnose transient tachypnea of the newborn (TTN) and has a great value in differentiating TTN from respiratory distress syndrome (RDS) (7). Additionally, many of the other common pulmonary and pleural diseases in neonates display specific findings on LUS which can be useful in the differential diagnosis (8).
We developed a screening model of bedside lung ultrasound assessment for infants requiring respiratory support5. Like any other diagnostic technique it should be only used in integration with the clinical assessment and interpreted according to the clinical presentation of the individual patient while considering particular limitations of this modality.
Point of care intestinal ultrasound:
Necrotising enterocolitis is a serious disorder in infants and commonly associated with complications like short bowel syndrome and total parenteral nutrition related issues. The reported mortality is up to 40%, so early diagnosis and management are essential (9). The radiographic diagnosis by XR after clinical suspicion is still the standard in most centers. The main issue with radiograph is being limited to 3 main findings, pneumatosis intestinalis (PI), portal vein gases (PVG), and perforation, and radiograph diagnosis of PI and PVG is sometimes a challenge with low sensitivity and wide range of inter-observer variability. There has been increasing evidence that with real-time ultrasound, PI and PVG can be better detected than with x-ray (10). Ultrasound is able to assess the bowel wall directly and detect bowel wall thickening or thinning, reduced peristalsis or abnormal bowel wall perfusion by color Doppler. Peritoneal fluid, both intraluminal and extra luminal is also visible (11,12). This can be performed in any suspected case with compromised intestinal performance like intestinal obstruction or ischemia and not only in cases with suspected NEC.
Table 1: different applications performed by either professional sonographer (radiologist or cardiologist) or a trained clinician
Cranial ultrasound
emergency assessment of suspected hemorrhage
Doppler assessment of cerebral arteries in cases hemodynamic instability e.g. PDA
Intestinal ultrasound Urgent evaluation of suspected necrotizing entercolitis, intestinal ischemia
Lung ultrasound New emerging modality for assessment of common neonatal lung diseases, e.g. RDS, TTN, meconium, pneumothorax, pleural effusions.
Focused heart ultrasound Assessment of specific neonatal hemodynamics issues
Vascular assessment Blood flow by Doppler for assessment of resistance or shunting of blood through arteriovenous malformation or PDA
Interventional POCUS Central line placement, lumber puncture, bladder tapping for urine sample. Peritoneal and pericardial tap of significant effusions
References:
1. Evans N, Gournay V, Cabanas F, et al. Point-of-care ultrasound in the neonatal intensive care unit: international perspectives. Semin Fetal Neonatal Med. 2011;16(1):61-68. doi:10.1016/j.siny.2010.06.005.
2. Pereda M a., Chavez M a., Hooper-Miele CC, et al. Lung ultrasound for the diagnosis of Pneumonia in Children: A Meta-analysis. Pediatrics. 2015;135(4):714-722. doi:10.1542/peds.2014-2833.
3. Escourrou G, De Luca D. Lung ultrasound decreased radiation exposure in preterm infants in a neonatal intensive care unit. Acta Paediatr. 2016:n/a-n/a. doi:10.1111/apa.13369.
4. Volpicelli G, Elbarbary M, Blaivas M, et al. International evidence-based recommendations for point-of-care lung ultrasound. Intensive Care Med. 2012;38(4):577-591. doi:10.1007/s00134-012-2513-4.
5. Elsayed Y, Abdelmawla M, Narvey M. A model of integrated lung and focused heart ultrasound as a new screening examination in infants at risk of respiratory or hemodynamic compromise. 2017;6(1):1-14. doi:10.7363/060131.
6. Xirouchaki N, Magkanas E, Vaporidi K, et al. Lung ultrasound in critically ill patients: comparison with bedside chest radiography. Intensive Care Med. 2011;37(9):1488-1493. doi:10.1007/s00134-011-2317-y.
7. Liu J, Cao H-Y, Wang X-L, Xiao L-J. The significance and the necessity of routinely performing lung ultrasound in the neonatal intensive care units. J Matern Neonatal Med. 2016;7058(March):1-6. doi:10.3109/14767058.2016.1152577.
8. Copetti R, Cattarossi L. Lung Ultrasound in Newborns, Infants, and Children. 2011:241-245. doi:10.1007/978-3-642-21247-5.
9. Dilli D, Suna Oğuz S, Erol R, Ozkan-Ulu H, Dumanlı H, Dilmen U. Does abdominal sonography provide additional information over abdominal plain radiography for diagnosis of necrotizing enterocolitis in neonates? Pediatr Surg Int. 2011;27(3):321-327. doi:10.1007/s00383-010-2737-8.
10. Bohnhorst B. Usefulness of abdominal ultrasound in diagnosing necrotising enterocolitis. Arch Dis Child Fetal Neonatal Ed. 2013;98:F445-50. doi:10.1136/archdischild-2012-302848.
11. Gale HI, Gee MS, Westra SJ, Nimkin K. Abdominal ultrasonography of the pediatric gastrointestinal tract. World J Radiol. 2016;8(7):656. doi:10.4329/wjr.v8.i7.656.
12. Kim H-Y, Kim I-O, Kim WS, Kang GH. Bowel sonography in sepsis with pathological correlation: an experimental study. Pediatr Radiol. 2011;41(2):237-243. doi:10.1007/s00247-010-1806-4.
When I think back to my early days as a medical student, one of the first lessons on the physical exam involves checking central and peripheral perfusion as part of the cardiac exam. In the newborn to assess the hemodynamic status I have often taught that while the blood pressure is a nice number to have it is important to remember that it is a number that is the product of two important factors; resistance and flow. It is possible then that a newborn with a low blood pressure could have good flow but poor vascular tone (warm shock) or poor flow and increased vascular tone (cardiogenic shock or hypovolemia). Similarly, the baby with good perfusion could be in septic shock and be vasodilated with good flow. In other words the use of capillary and blood pressure may not tell you what you really want to know.
Is there a better way?
As I have written about previously, point of care ultrasound is on the rise in Neonatology. As more trainees are being taught the skill and equipment more readily available opportunities abound for testing various hypotheses about the benefit of such technology. In addition to my role as a clinical Neonatologist I am also the Medical Director of the Child Health Transport Team and have pondered about a future where ultrasound is taken on retrievals to enhance patient assessment. I was delighted therefore to see a small but interesting study published on this very topic this past month. Browning Carmo KB and colleagues shared their experience in retrieving 44 infants in their paper Feasibility and utility of portable ultrasound during retrieval of sick preterm infants. The study amounted to a proof of concept and took 7 years to complete in large part due to the rare availability of staff who were trained in ultrasound to retrieve patients. These were mostly small higher risk patients (median birthweight, 1130 g (680–1960 g) and median gestation, 27 weeks (23–30)). Availability of a laptop based ultrasound device made this study possible now that there are nearly palm sized and tablet based ultrasound units this study would be even more feasible now (sometimes they were unable to send a three person team due to weight reasons when factoring in the ultrasound equipment). Without going into great detail the measurements included cardiac (structural and hemodynamic) & head ultrasounds. Bringing things full circle it is the hemodynamic assessment that I found the most interesting.
Can we rely on capillary refill?
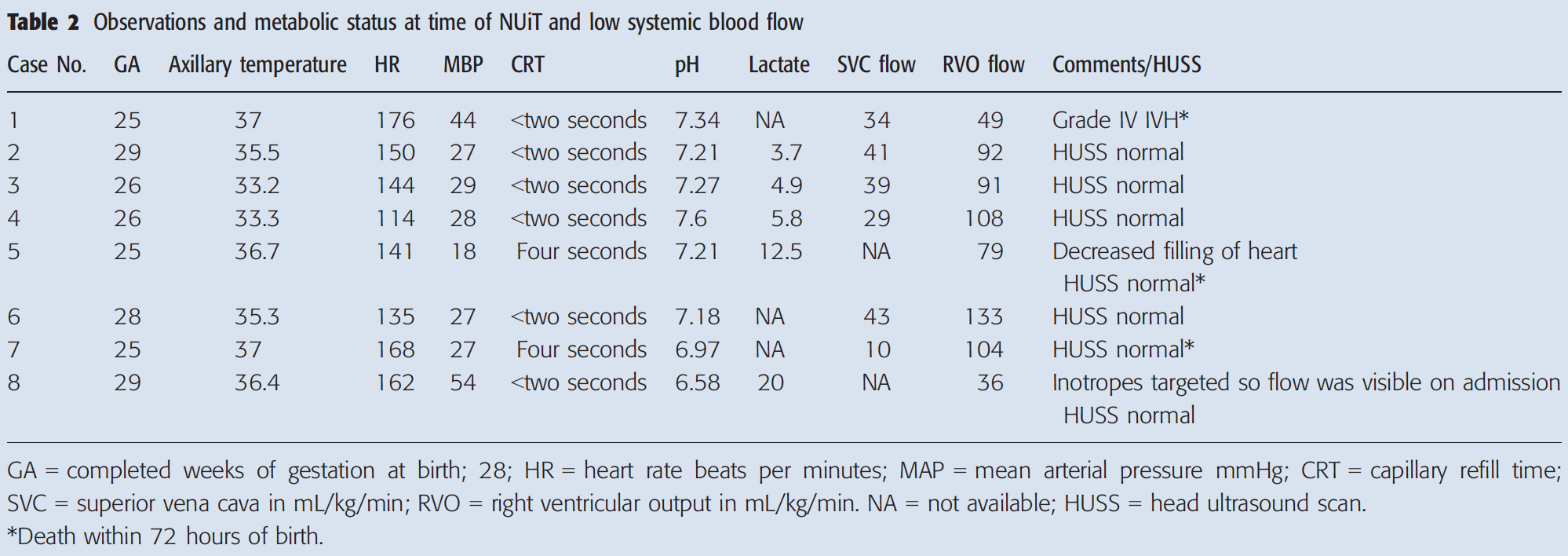
From previous work normal values for SVC flow are >50 ml/kg/min and for Right ventricular output > 150 ml/kg/min. These thresholds if not met have been correlated with adverse long term outcomes and in the short term need for inotropic support. In the absence of these ultrasound measurements one would use capillary refill and blood pressure to determine the clinical status but how accurate is it?
First of all out of the 44 patients retrieved, assessment in the field demonstrated 27 (61%) had evidence using these parameters of low systemic blood flow. After admission to the NICU 8 had persistent low systemic blood flow with the patients shown below in the table. The striking finding (at least to me) is that 6 out of 8 had capillary refill times < 2 seconds. With respect to blood pressure 5/8 had mean blood pressures that would be considered normal or even elevated despite clearly compromised systemic blood flow. To answer the question I have posed in this section I think the answer is that capillary refill and I would also add blood pressure are not telling you the whole story. I suspect in these patients the numbers were masking the true status of the patient.
How safe is transport?
One other aspect of the study which I hope would provide some relief to those of us who transport patients long distance is that the head ultrasound findings before and after transport were unchanged. Transport with all of it’s movement to and fro and vibrations would not seem to put babies at risk of intracranial bleeding.
Where do we go from here?
Before we all jump on the bandwagon and spend a great deal of money buying such equipment it needs to be said “larger studies are needed” looking at such things as IVH. Although it is reassuring that patients with IVH did not have extension of such bleeding after transport, it needs to be recognized that with such a small study I am not comfortable saying that the case is closed. What I am concerned about though is the lack of correlation between SVC and RVO measurements and the findings we have used for ages to estimate hemodynamic status in patients.
There will be those who resist such change as it does require effort to acquire a new set of skills. I do see this happening though as we move forward if we want to have the most accurate assessment of clinical status in our patients. As equipment with high resolution becomes increasingly available at lower price points, how long can we afford not to adapt?
It has been some time since I wrote on the topic of point of care ultrasound (POC). The first post spoke to the benefits of reducing radiation exposure in the NICU but was truly theoretical and also was really at the start of our experience in the evolving area. Here we are a year later and much has transpired.
We purchased an ultrasound for the NICU in one of our level III units and now have two more on the way; one for our other level III and one for our level II unit. The thrust of these acquisitions have been to reduce radiation exposure for one but also to shorten the time to diagnosis for a number of conditions. No matter how efficient x-ray technologists are, from the time a requisition is placed to the arrival of the tech, placement of the baby and then processing of the film, it is much longer than using a POC at the bedside. Having said that though is it accurate? There are many examples to choose from but when thinking about times when one would like an answer quickly I can’t think of anything much better than a pneumothorax.
Chest X-ray vs POC for Diagnosis of Pneumothorax
The diagnosis of a pneumothorax is easily diagnosed by ultrasound when there is an absence of lung sliding as seen in this video. In the majority of cases employing POC we are looking at ultrasound artifacts. In the case of pleural sliding which is best described as ants marching, it’s absence indicates the presence of a pneumothorax. The “lung point” sign as shown in this video marks the transition from pleural sliding to none and in a mode called “M” appears as a bar code when the pneumothorax is present.
Using such signs Raimondi F et al as part of the LUCI (Lung Ultrasound in the Crashing Infant) group compared traditional x-ray diagnosis as the gold standard to POC for diagnosis of pneumothorax. This study is important as it demonstrated two very important things in the 42 infants who were enrolled in the study. The first was the accuracy of POC. In this study each patient had both an ultrasound and an x-ray and the results compared to determine how accurate the POC was. Additionally in cases where there was no time for an x-ray to confirm the clinical suspicion the accuracy of the study was determined based on the finding of air with decompression along with abrupt clinical improvement. In case people are wondering infants as small as 24 weeks were included in the study with an average weight of 1531 +/-832 g for included infants.
The accuracy was stunning with a sensitivity and specificity of 100% each. Comparing this with clinical evaluation (transillumination, assessment of breath sounds) was far less accurate with a sensitivity of 84% (65-96) and specificity 56% (30-80).
Adding to the accuracy of the test is the efficiency of the procedure. “After clinical decompensation, lung ultrasound scans were completed in a mean time of 5.3 +/- 5.6 minutes vs a mean time of 19 +/- 11.7 minutes required for a chest radiograph (P < .001).” In short, it is very accurate and can be done quickly. In an emergency, can you think of a better test?
If efficiency weren’t enough what about the reduction in radiation exposure?
This was the focus of a recent paper by Escourrou G & Deluca D entitled Lung ultrasound decreased radiation exposure in preterm infants in a neonatal intensive care unit. The authors in this study chose to examine retrospecitively the period from 2012 – 2014 as in 2013 they rolled out a program of teaching POC ultrasound to clinicians. The purpose of this paper was to see if practitioners educated in interpretation of ultrasound would actually change their practice and use less ionizing radiation.
Their main findings are indicated in the table
Test
2012
2014
p
Min 1 x-ray during admission
81%
70%
<0.001
Total x-rays
1976
1476
Mean x-rays per patient
4.9+/-1.5
2.6+/-1.0
<0.001
Mean radiation dose (microGy)
183+/-78
68+/-30
<0.001
As they predicted use of ionizing radiation dropped dramatically. I should also mention that they tracked outcomes such as IVH, mortality and BPD to name a few and found no change over time. In conclusion the use of ultrasound did not affect major outcomes but did spare each neonate ionizing radiation.
Now before anyone hits the panic button I still think the amounts of radiation here are safe for the most part. In Canada the maximum allowed dose for the public per year is 1 mSv which is the equivalent of 1000 microGy. This was obtained from the Nuclear Safety agency in Canada in case you are interested in finding out more about radiation safety limits.
Back in 2012 at least in this study, 2 standard deviations from the mean would have put the level received at a little over a third of what the annual limit is but it is the outliers we need to think of. What about kids getting near daily x-rays while on high frequency ventilation or for monitoring pleural fluid collections? There certainly are many who could receive much higher dosages and it is for those kids that I believe this technology is so imperative to embrace.
It will take time to adopt and much patience. With any new roll out there is a learning curve. Yes there will be learners who will need to handle patients and yes there will be studies done at times to obtain the skills necessary to perform studies in an efficient and correct manner but I assure you it will be worth it. If we have a way of obtaining faster and accurate diagnoses and avoiding ionizing radiation don’t we owe it to our patients and families to obtain such skill? I look forward to achieving a centre of excellence utilizing such strategies and much like this last study it will be interesting to look back in a year an see how things have changed.
This post is meant to supplement an earlier post on the same topic.
Since introducing POC U/S in our unit there has been great enthusiasm and we will begin shortly introducing our nursing group to it’s use in order to enhance usage. Now that we have had some exposure we took the time to capture some our thoughts on this technology in this accompanying video graciously supported by the Children’s Hospital Foundation in Winnipeg. To watch this wonderful video by Dr. Ganesh Srinivasan a Neonatologist and technology aficionado in our institution click on the link below.