Anyone who works in the NICU is more than familiar with the sad moment when you find out an infant has suffered a severe IVH (either grade III or IV) and the disclosure to the family. The family is in a state of shock with the fear of ventricular drainage a reality that will likely come to pass. We have spent many years trying to find ways to reduce this risk and antenatal steroids and delayed cord clamping are two relatively recent interventions that have had a real impact. Unfortunately we have not been able to eliminate this problem though. What if something as simple as an exclusive human milk diet could be that magic bullet to further reduce this problem in our NICUs?
Exclusive human milk diets
I have written about this topic before but as a refresher this generally refers to all sources of nutrition being derived from human milk. Ideally we would provide mothers own milk (MOM) but when this is not available units rely on pasteurized donor human milk (PDHM) as the base feed. Added to this is human derived human milk fortifier (H2HMF) as opposed to bovine powdered or liquid fortifier usually to provide a base caloric density of 24 cal/oz.
Reducing IVH Through Exclusive Human Milk Diets
It would be nice to have a prospective multicentre trial with this as the outcome but there is a significant problem when doing this type of study. The H2HMF is costly with a price tag of about $13-15000 per treatment course so to do a prospective RCT would not be easy for units that don’t use the product already. Moreover, for those units that are already sold on the product it would seem unethical if there was no equipoise to randomize to bovine or human fortifier. As such, when we talk about getting the best evidence it is most likely going to come in the form of a retrospective study as has been done here by Carome K et al in their paper Exclusive human milk diet reduces incidence of severe intraventricular hemorrhage in extremely low birth weight infants.
The authors in this study chose to look at three different time periods with different approaches to feeding of ELBW infants. They were as follows with all diets providing H2HMF going until 34 weeks. Aside from the source of nutrition, starting of and incremental advancement of feedings was protocolized as per unit approach.
2012 to 2014 – MOM was given when available. Preterm formula was the alternative as a supplement Fortification of was with bovine milk-derived liquid fortifier 2014 to 2015 – H2HMF used in those infants receiving exclusively MOM. All others received preterm formula as supplement or alternative. If MOM was available but in insufficient quantities for sole diet, it was fortified with bovine-HMF 2015 to 2017 – all ELBW infants received an EHM diet consisting of MOM if available and PDHM as a supplement to MOM or as full diet, each fortified with H2HMF
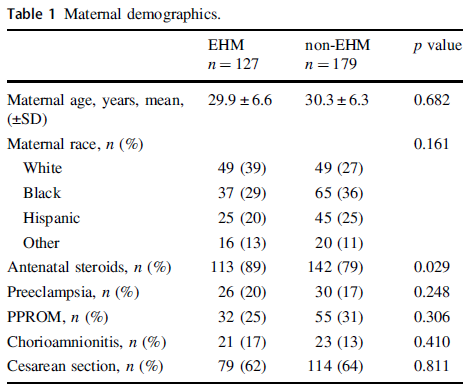
The maternal demographics were similar between those receiving exclusive human milk diets and those without except for a higher antenatal steroid provision in the EHM group. This of course bears consideration in the results as steroids have been shown to reduce IVH.
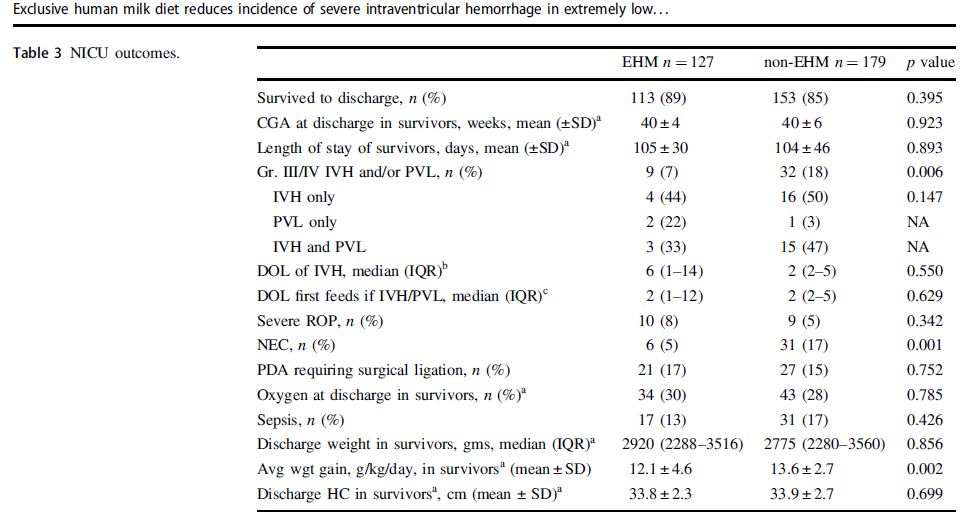
Looking at the results below shows some very promising findings. The incidence of Grade III/IV IVH and/or PVL was 7% in the EHM group and 18% in the non-EHM group. Also noted to be quite different was the incidence of NEC which was 5% in the EHM and 17% in the non group. The authors also did a subgroup analysis looking at the use of MOM vs PDHM and found no difference in outcomes regardless of source of human milk used. As the authors point out this might mean that the pasteurization process does not denature the components of milk responsible for these protective effects if the results are to be believed.
One strength of the study was that the authors performed a logistic regression to control for the higher rate of antenatal steroid use and lower rates of NEC in the EHM group since both would be expected to influence rates of IVH/PVL and found that the results remained significant after this analysis. The findings were an OR of 2.7 CI 1.2–6.0, p = 0.012 so that is promising!
What They Weren’t Able to Do
It’s possible I missed it in the article but like several other papers on this topic the babies who received formula and those who received human milk with bovine fortifier were grouped together. As such what we don’t know from this study is whether the addition of just the bovine fortifier vs H2HMF would have yielded the same results.
Nonetheless what the article does suggest is that use of EHM diets are protective against severe IVH/PVL regardless of the source of human milk when you compare it to receipt of any bovine sources. The caveats about retrospective studies of course exist as per usual but if this is the best evidence we have how do we use it? At the very least this calls out for strategies to maximize milk production for mothers and to use PDHM when MOM is not available. It certainly is suggestive that the use of H2HMF may confer benefit as well. What you unit does with this information I suppose will need to be determined based on the totality of the evidence. I suspect there is more of this story to be told and this adds yet another chapter in the tale of EHM.
It seems so simple doesn’t it. Shouldn’t we just be able to feed milk whether it be from humans or cows and our preemies will just adapt? I have often written about human milk diets vs those with bovine but this week an intriguing article came my way that really gave me some pause to say hmmm. Human milk diets have been shown to reduce the risk of necrotizing enterocolitis (NEC) compared to use of formula. The use of bovine human milk fortifiers falls somewhere in the middle I suppose as the diet in that case is mostly human milk with some bovine sprinkled in so to speak. If NEC is something that these infants are at increased risk of then what might be going at a tissue level when infants are exposed to human milk alone vs other bovine ingestions?
Near Infrared Spectroscopy May Tell Us the Answer
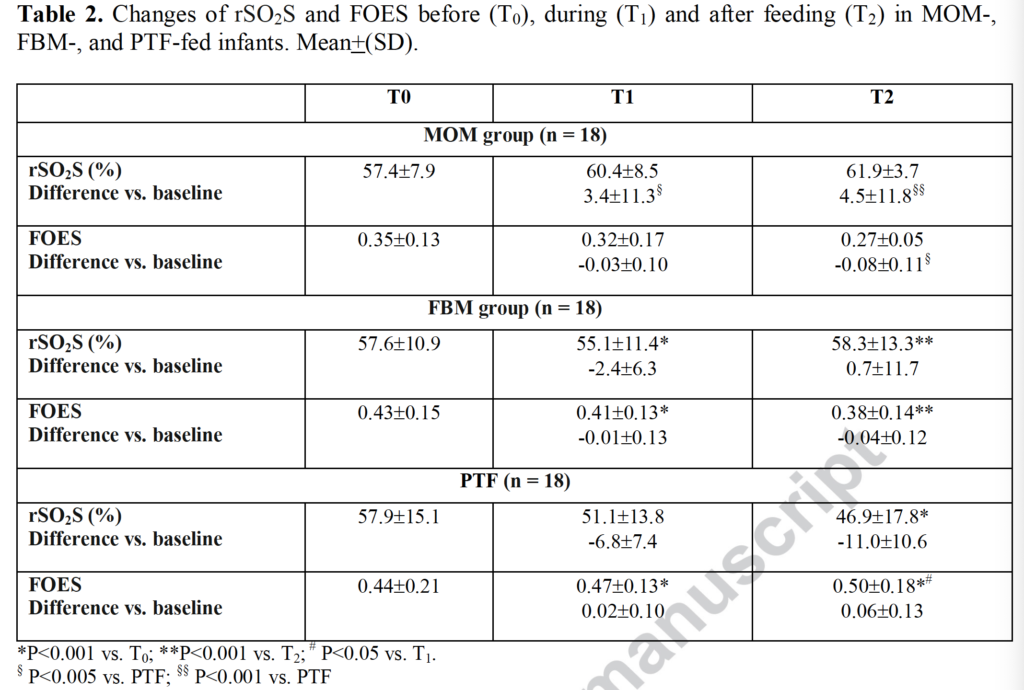
Dani C et from Italy just published an elegant study entitled EFFECT ON SPLANCHNIC OXYGENATION OF BREAST MILK, FORTIFIED BREASTMILK, AND FORMULA MILK IN PRETERM INFANTS. The study looked at the use of two particular measurements from regional splanchnic NIRS application. One is called splanchnic regional oxygenation (rSO2S) and the other splanchnic fractional oxygen extraction ratio (FOES). The rSO2S tells you how much oxygen is in the gut at a tissue level and FOES which is calculated by using systemic oxygenation (SpO2) using the formula (SpO2-rSO2S)/SpO2). So FOES will be high when rSO2S is low meaning the gut relative to the rest of the body is consuming more oxygen. For this study, increments in feedings were standardized for all infants. The study was done once patients were on full bolus feedings for one week.
The authors designed a study that needed 15 infants in three different groups with the first being human milk, then human milk + bovine fortifier and then the last formula fed infants. NIRS data was recorded 30 minutes before a feed (T0), 30 minutes after a bolus feed (T1) and then 2 hours after a bolus feed (T2). In the end the authors recruited 18 per arm. What the authors found is what I am having trouble not running with in terms of its meaning.
Looking at the data, babies who were fed exclusively mothers own milk experienced no change at all in rSO2S at any time points. Interestingly the value even trended higher after a feed. Infants who received fortified human milk experienced a decrease in this value from before the feed to 30 minutes afterwards but then recovered by 2 hours. Formula fed infants though simply dropped from exposure to formula after 30 minutes through 2 hours and the FOES rose over that time demonstrating a greater amount of oxygen extraction by the gut.
What is the meaning of all this?
Bovine sources of nutrition in the form of fortifier seem to cause the gut to become more metabolically active and consume more oxygen at least for the first 30 minutes after a feeding. Formula tends to have a progressive increase in oxygen extraction over the first two hours post feed. This may be reflective of stress in the gut as it works harder to absorb and process nutrients from a bovine source and perhaps in a dose response fashion, a little bovine content as in fortifier causes some short term increase in oxygen demand vs pure bovine formula causing a sustained increase in oxygen need.
This situation sets up an interesting concept. The NIRS results if you recall are from babies who have reached full feeds for one week. What if these same studies had been done in babies who were just in the process of increasing feeds? If infants consuming bovine sources of nutrition need more oxygen in the gut, might this explain why in the presence of acidosis, congenital heart defects or even with a PDA causing changes in end diastolic flow that they don’t tolerate in many cases anything other than human milk?
I am not aware of any such studies looking at feeding advancement but it does really make me wonder what we would see as we advance feedings using our protocols? It is tempting to place abdominal NIRS sensors on the bellies of preterm infants who are just starting out on HMF and see what happens? If the rSO2S was going down and/or the FOES was rising, would you stop the bovine fortification if it reached a certain point? What would happen if a human milk fortifier was used instead of a bovine source? Any difference?
So many questions and in my mind a great area for research. I can’t wait to see where this all goes.
After several reports providing reassurance to breastfeeding mothers, two very recent reports are giving me reason to pause. The Canadian Pediatric Society has been recommending breastfeeding if a mother has COVID19 with precautions in place; Breastfeeding when mothers have suspected or proven COVID-19. It would be heresy to suggest that a mother not be permitted to breastfeed her infant but what follows are two reports that at the very least may need to enter the discussion when a COVID19 positive mother gives birth and is deciding about route of feeding.
Toronto Case Report
The first report was notable not so much for breastmilk but rather that a mother with a chronic immunodeficiency and pneumonia from COVID19 had placental surfaces that tested positive on PCR for COVID19. This was the main focus of the paper Probable congenital SARS-CoV-2 infection in a neonate born to a woman with active SARS-CoV-2 infection. In the same paper though, testing of breastmilk in this mother demonstrated a positive PCR with a semi-quantitative cycle time result (there are 40 cycles of amplification of RNA in PCR testing- the further away from 40 cycles the more likely it is a true positive).
The results above were positive at 2 days and negative at 7 days. One could possibly excuse this case as an anomaly since the mother in this case not only was sick but also has chronic neutropenia but then along comes another report.
Second Research Report
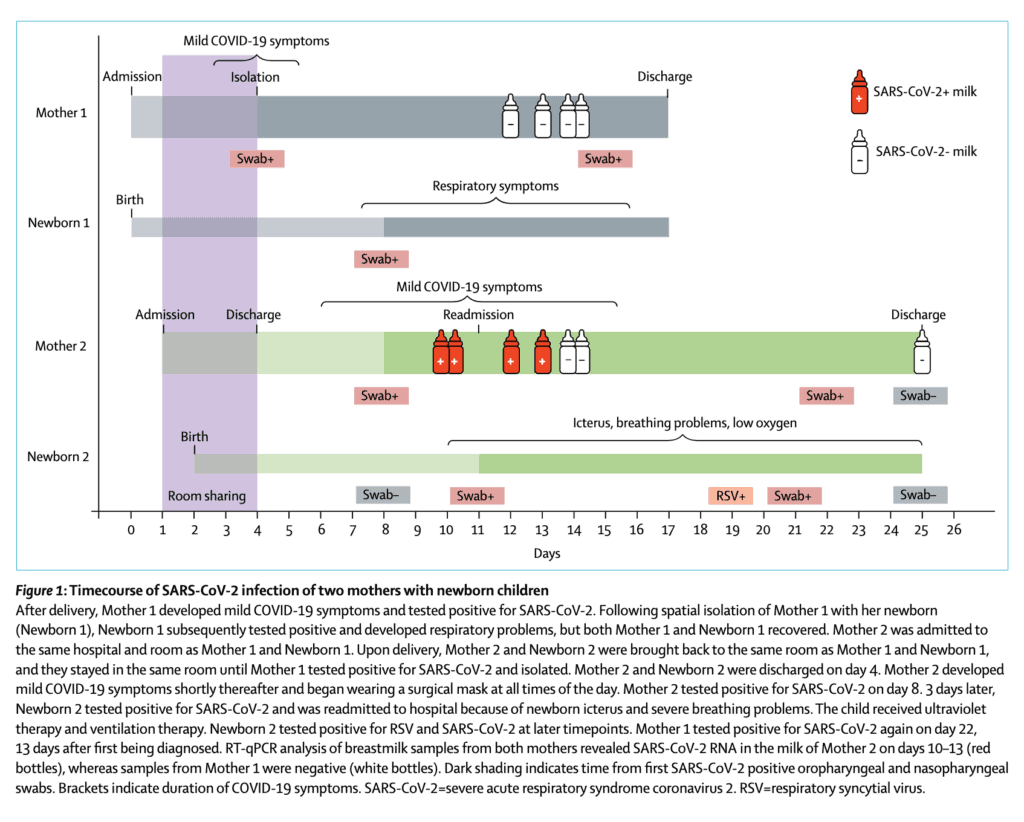
This week a second report emerged that adds to the uncertainty around breastmilk. Detection of SARS-CoV-2 in human breastmilk looks at two mothers one of whom was negative on testing of breastmilk but the other unfortunately tested positive. The authors included the following timeline which is very informative.
From the timeline above you will note that in the second case the mother becomes positive at 11 days of age and the infant tests positive around the same time the milk comes back positive. The infant in this case also develops RSV which likely explains the symptoms they developed later in the course. What is concerning to me though is that in this case while the mother was COVID19 positive, she was not acutely ill. When thinking of vertical transmission this has been something that has been postulated in suspecting that those with more severe illness have higher viral loads and therefore may be capable of vertical transmission. Not the case here if the results are to be believed. Adding to the strength of the result are Ct values for SARSCoV2 N peaked at 29∙8 and 30∙4 in whole milk and skimmed milk respectively so this seems real.
How does this differ than past testing?
What intrigues me about this study in particular is that past research on transmission into breastmilk has failed to detect the virus. It could be that previous testing close to delivery was negative and that with time might the virus enter breastmilk? At eleven days I think this may be the latest testing done. In virtually all cases reported about COVID19 positives in newborns the authors have always explained the painstaking steps they took to prevent postnatal infection. I do wonder now if some of these cases may be related to a small percentage of women carrying the virus in their breastmilk. This leaves us in a tough spot. What do we tell women who are thinking of breastfeeding and have COVID19? There will need to be discussion on this but one option is to proceed with feeding accepting there may be a small risk of transmission. A second option would be to test milk but if the transmission occurs late you may miss it in hospital on initial sampling Finally it may be worth pumping and discarding milk until mothers test negative and using donor breastmilk in the meantime (or formula for those who don’t have DBM).
Regardless I think this information coming out will need to be digested and centres think about how they will approach this issue. My guess is these will not be the last reports on this.
The metabolic syndrome describes the development as an adult of centripetal obesity, high blood pressure, high triglycerides, elevated blood sugar and low HDL cholesterol. These constellation of problems significantly increase the risk of cardiovascular disease, stroke and diabetes.
The theory here is that conditions in utero in which the fetus is chronically deprived of blood flow and nutrition lead to a tendency towards insulin resistance. The body is essentially trying to use any energy it is receiving to stay alive in an environment in which resources are scarce. Given that situation, resisting the effects of insulin by preventing storage of this needed energy serves a useful purpose but in the long run may be detrimental as the body become programmed to resist the effects of this hormone.
What if this programming could be overcome?
Breast milk certainly has many incredible properties and as we learn more we discover only more applications. My previous post on putting breast milk in the nasal cavity is just one such example (Can intranasal application of breastmilk cure severe IVH?). In 2019 Dr. Hair and Abram’s group looked at this with respect to insulin resistance and with potential extrapolation to the metabolic syndrome in their paper Premature small for gestational age infants fed an exclusive human milk-based diet achieve catch-up growth without metabolic consequences at 2 years of age. Texas Children’s Hospital uses an exclusive human milk diet for premature infants with the following criteria GA of <37 weeks, BW of ≤1250 g, with the diet maintained until approximately 34 weeks PMA. Exclusive human milk is provided through a combination of mother’s own milk and Prolacta instead of a bovine based human milk fortifier. In this study they were able to prospectively track 51 preterm infants of which 33 were AGA and 18 SGA. The first visit (visit 1) was performed at 12–15 months CGA and the second visit (visit 2) was at 18–22 months CGA. The question at hand was whether these children would experience catch up growth at 2 years of age and secondly what their levels of insulin might look like at these times. Higher insulin levels might correlate with levels of insulin resistance with higher levels being needed to maintain euglycemia. As a measure of insuline resistance the authors used the calculation of the Non-fasting homeostatic model of assessment-insulin resistance (HOMA-IR) = (insulin × glucose)/22.5 which has been validated elsewhere. Protein intakes were equal for both groups at about 4 g/kg of human milk protein.
The Results Please
The SGA group had greater weight gain between visit 1 and 2 as evidenced by a significant difference in the change in BMI z-score, AGA −0.21±0.84 vs.SGA 0.25±1.10. I suppose this isn’t too shocking as we know that many babies born SGA experience catch up growth after discharge. What is surprising and once again speaks to the power of breast milk is the impact observed on insulin levels and resistance to the same as measured by the HOMA-IR (AGA babies are the left column and SGA the right).
The adjusted p vlaues for glucose were 0.06 with insulin and HOMA-IR being 0.02. What does this mean? Well, these are not fasting insulin levels which would be ideal but what it does say is that at fairly comparable glucose levels the level of insulin is higher in former AGA babies and the level of insulin resistance lower in the SGA infants! This result is quite the opposite of what previous studies have shown as referenced above. Aren’t these growth restricted infants supposed to have had insulin resistance in utero and been programmed for life to have insulin resistance and as adults develop the metabolic syndrome? This study falls short of making any claims about the latter as these infants are only two years of age. What this study provides though is certainly a raised eyebrow. There will be those of course that look at the size of the study and dismiss it as being too small but at the very least this study will lead to further work in this area. This paper though adds to the mystery around the potential impacts of breast milk and certainly provides strength to the thought that perhaps breastmilk should be the exclusive source of nutrition for preterm infants in the NICU. While I understand that not all women are able to produce enough for their own infants or may choose not to for a variety of reasons, with access to donor milk supply this could become a reality. The cost savings to the health care system by preventing insulin resistance would be many fold greater than the cost of donor milk in the newborn period.
Another intriguing question will be whether use of an exclusive human milk diet with use of only mother’s own milk will have similar effects or even greater impact on glucose homestasis later in life. I think the authors are to be commended for their dedication to work in this field and I certainly look forward to the next publication from this group.
The medical term for this is placentophagy and it is a real thing. If you follow the lay press you may have seen that originally this was promoted by Kourtney Kardashian who did this herself and then by Kim who planned on doing the same after delivery. See Did Kourtney Kardashian Eat Her Placenta?
This is not completely without basis as many readers will be thinking already that they have heard about the health benefits of doing the same. Reports of improved mood and reductions in the baby blues following ingestion of placenta as well as improvements in breast milk production have led to this growing practice. The evidence for this up until recently though was quite old and fraught with poorly design of such studies. The bigger driver however has been word of mouth as many women having heard about the promises of better mood at the very least have thought “why not? Can’t hurt.”
What I will do in this post is run through a little background and a few recent studies that have shed some light on how likely this is to actually work.
Where did the idea come from?
Animals eat their placentas after delivery. It turns out that unprocessed placenta is quite high in the hormone prolactin which is instrumental for breastfeeding. Given the large amount of this hormone as well as the number of other hormones present in such tissue it was thought that the same benefits would be found in humans. Eating unprocessed human tissue whether it is put in a capsule or not is unwise as unwanted bacteria can be consumed. In fact, a case of GBS sepsis has been linked to such a practice in which the source of the GBS was thought to be due to contaminated unprocessed maternal placenta that had been ingested. Buser GL, Mat´o S, Zhang AY, Metcalf BJ, Beall B, Thomas AR. Notes from the field: Late-onset infant group B streptococcus infection associated
with maternal consumption of capsules containing dehydrated placenta.
What happens when you process placenta by steaming and drying?
This would be the most common way of getting it into capsules. This process which renders it safe to consume may have significant effects on reducing hormonal levels.This was found in a recent study that measured oxytocin and human placental lactogen (both involved positively in lactation) and found reductions in both of 99.5% and 89.2%, respectively compared versus raw placenta. I would assume that other hormones would be similarly affected so how much prolactin might actually wind up in these capsules after all?
Clinical Randomized Double Blind Controlled Trial
Twenty seven women from Las Vegas were recruited into a pilot trial (12 beef placebo vs 15 steamed and dried placenta) with the authors examining three different outcomes across three studies. The first study Effects of placentophagy on maternal salivary hormones: A pilot trial, part 1 looked at a large number of salivary hormones at four time points. Plasma samples were taken as well to determine the volume of distribution of the same. First samples were at week 36 of gestation then within 4 days (96 h) of birth followed by days 5–7 (120–168 h) postpartum and finally Days 21–27 (504–648 h) postpartum. All consumption of capsules was done in the home as was collection of samples. As per the authors in terms of consumption it was as follows “two 550 mg capsules three times daily for the first 4 days; two 550 mg capsules twice daily on days 5 through 12, and then to decrease the dose to two 550 mg capsules once daily for the remainder of the study (days 13 through approximately day 20 of supplementation).
Outcomes
No difference was found between salivary concentrations of hormones at any time point other than that with time they declined following birth. Curiously the volume of distribution of the hormones in serum was slightly higher in the placenta capsule groups but not enough to influence the salivary concentrations. It was felt moreover that the amount of incremental hormone level found in the serum was unlikely to lead to any clinical response.
The second study was on mood Placentophagy’s effects on mood, bonding, and fatigue: A pilot trial, part 2. Overall there were no differences for the groups but they did find “some evidence of a decrease in depressive symptoms within the placenta group but not the placebo group, and reduced fatigue in placenta group participants at the end of the study compared to the placebo group.”
What is clear to me is that the answer to this question remains unclear! What is clear is that I don’t think it is wise to consume raw placenta due to the risks of bacterial contamination. Secondly, the levels of hormones left in the placental preparation and the most common preparation of steaming and drying leave hormone levels that are unlikely to influence much at all from a biochemical standpoint. It also seems that breastmilk production and neonatal weight gain aren’t influenced much by consumption of these pills.
The issue though in all of this is that while the previous research was of low quality, the current research while of better quality is at a low volume. These were pilot trials and not powered to find a difference likely. The finding in the subgroup of some effect on mood at the end of the study does leave some hope to those that believe in the power of the placenta to help. Would a larger study find benefit to this practice? My suspicion from a biochemical standpoint is not but that one may feel a benefit from a placebo response.
Should you go out and have your placenta prepared for consumption? If you have Kardashian like wealth then go for it if you think it will help. If you don’t then I would suggest waiting for something more definitive before spending your money on placentophagy.