Anyone who works in the NICU is more than familiar with the sad moment when you find out an infant has suffered a severe IVH (either grade III or IV) and the disclosure to the family. The family is in a state of shock with the fear of ventricular drainage a reality that will likely come to pass. We have spent many years trying to find ways to reduce this risk and antenatal steroids and delayed cord clamping are two relatively recent interventions that have had a real impact. Unfortunately we have not been able to eliminate this problem though. What if something as simple as an exclusive human milk diet could be that magic bullet to further reduce this problem in our NICUs?
Exclusive human milk diets
I have written about this topic before but as a refresher this generally refers to all sources of nutrition being derived from human milk. Ideally we would provide mothers own milk (MOM) but when this is not available units rely on pasteurized donor human milk (PDHM) as the base feed. Added to this is human derived human milk fortifier (H2HMF) as opposed to bovine powdered or liquid fortifier usually to provide a base caloric density of 24 cal/oz.
Reducing IVH Through Exclusive Human Milk Diets
It would be nice to have a prospective multicentre trial with this as the outcome but there is a significant problem when doing this type of study. The H2HMF is costly with a price tag of about $13-15000 per treatment course so to do a prospective RCT would not be easy for units that don’t use the product already. Moreover, for those units that are already sold on the product it would seem unethical if there was no equipoise to randomize to bovine or human fortifier. As such, when we talk about getting the best evidence it is most likely going to come in the form of a retrospective study as has been done here by Carome K et al in their paper Exclusive human milk diet reduces incidence of severe intraventricular hemorrhage in extremely low birth weight infants.
The authors in this study chose to look at three different time periods with different approaches to feeding of ELBW infants. They were as follows with all diets providing H2HMF going until 34 weeks. Aside from the source of nutrition, starting of and incremental advancement of feedings was protocolized as per unit approach.
2012 to 2014 – MOM was given when available. Preterm formula was the alternative as a supplement Fortification of was with bovine milk-derived liquid fortifier 2014 to 2015 – H2HMF used in those infants receiving exclusively MOM. All others received preterm formula as supplement or alternative. If MOM was available but in insufficient quantities for sole diet, it was fortified with bovine-HMF 2015 to 2017 – all ELBW infants received an EHM diet consisting of MOM if available and PDHM as a supplement to MOM or as full diet, each fortified with H2HMF
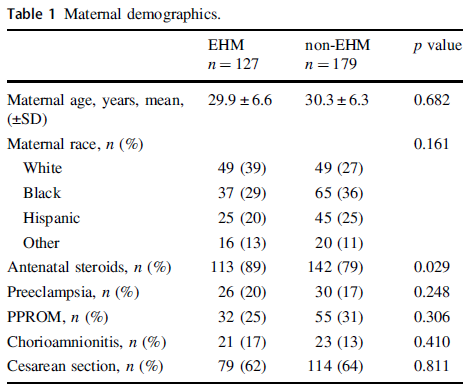
The maternal demographics were similar between those receiving exclusive human milk diets and those without except for a higher antenatal steroid provision in the EHM group. This of course bears consideration in the results as steroids have been shown to reduce IVH.
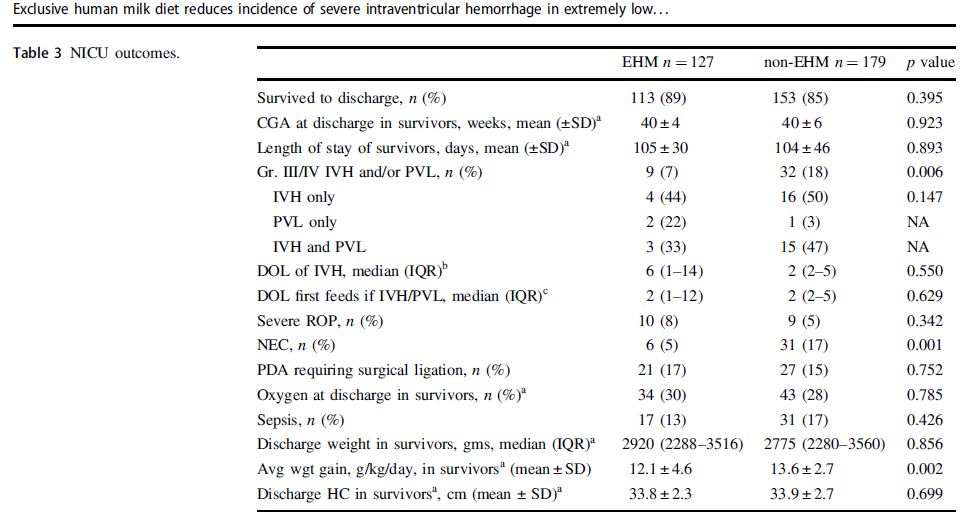
Looking at the results below shows some very promising findings. The incidence of Grade III/IV IVH and/or PVL was 7% in the EHM group and 18% in the non-EHM group. Also noted to be quite different was the incidence of NEC which was 5% in the EHM and 17% in the non group. The authors also did a subgroup analysis looking at the use of MOM vs PDHM and found no difference in outcomes regardless of source of human milk used. As the authors point out this might mean that the pasteurization process does not denature the components of milk responsible for these protective effects if the results are to be believed.
One strength of the study was that the authors performed a logistic regression to control for the higher rate of antenatal steroid use and lower rates of NEC in the EHM group since both would be expected to influence rates of IVH/PVL and found that the results remained significant after this analysis. The findings were an OR of 2.7 CI 1.2–6.0, p = 0.012 so that is promising!
What They Weren’t Able to Do
It’s possible I missed it in the article but like several other papers on this topic the babies who received formula and those who received human milk with bovine fortifier were grouped together. As such what we don’t know from this study is whether the addition of just the bovine fortifier vs H2HMF would have yielded the same results.
Nonetheless what the article does suggest is that use of EHM diets are protective against severe IVH/PVL regardless of the source of human milk when you compare it to receipt of any bovine sources. The caveats about retrospective studies of course exist as per usual but if this is the best evidence we have how do we use it? At the very least this calls out for strategies to maximize milk production for mothers and to use PDHM when MOM is not available. It certainly is suggestive that the use of H2HMF may confer benefit as well. What you unit does with this information I suppose will need to be determined based on the totality of the evidence. I suspect there is more of this story to be told and this adds yet another chapter in the tale of EHM.
If you have been following this blog for some time you would know that discussions about breastfeeding or breast milk are not an uncommon topic here. Literature exits already examining the impact of consumed breast milk on such outcomes as BPD and ROP. Much of our taste though is influenced by our sense of smell. Our olfactory sense therefore might be quite powerful in terms of having a calming effect on the neonate undergoing a painful procedure. This is the exact hypothesis of a recent study looking at the calming effect of the odor of breast milk during heel lance procedures.
The Study
This study out of Turkey by Tasci B is entitled The Calming Effect of Maternal Breast Milk Odor on Term Infant: A Randomized Controlled Trial. The authors performed a randomized trial of 84 infants (42 formula vs 42 mothers own milk) in which infants prior to a heel poke were exposed to the scent of either formula or human milk for a three minute duration. All infants were between 38-42 weeks gestation at birth and weighted between 2500 – 4000g. Two milliliters of either feed were soaked into filter paper and held under the nose for the study. Perhaps the only fault here was that the study could not be double blinded as the authors note that the intervention and assessment were done by the same researcher. The study though did use pain assessments using the NIPS scoring system and in addition to the researcher a nurse also did a simultaneous assessment. From a biological standpoint, as other authors have done before them, salivary cortisol was used to measure stress response of the infant before and after the noxious stimuli. Conditions under which sampling and scoring were done were standardized as much as possible by maintaining the temperature of the room at 23-26 degrees, and doing all heel pokes 1 hour after a feed.
The Results Please
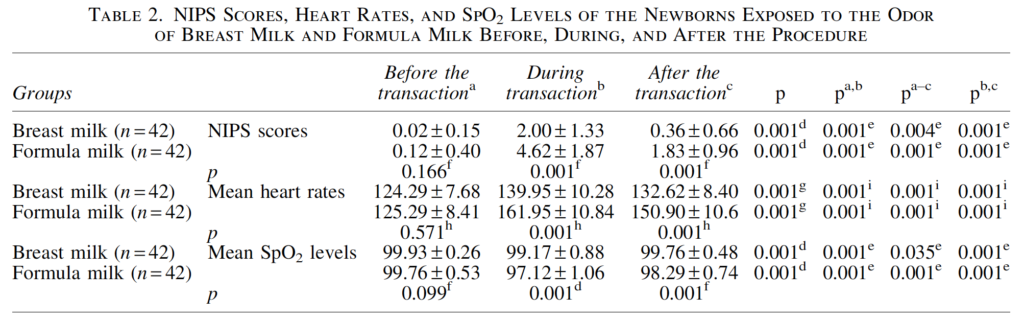
Pain scoring, heart rate and oxygen saturation levels were all better under conditions of sniffing breast milk than formula as shown in Table 2. The oxygen saturation decline in those who sniffed formula was not clinically significant but did reach statistical significance.
Also perhaps not surprisingly the duration of infant crying was much shorter with exposure to the scent of breast milk vs formula.
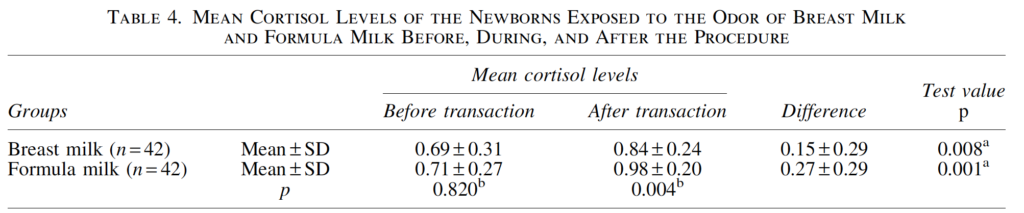
Finally the stress response biologically appeared to be attenuated with exposure to breast milk.
What now?
The results of the study are quite interesting to me in that prior work has shown that drops of human milk on a pacifier or in the mouth can improve tolerance to pain. This study adds to the research out there by demonstrating just the scent of breast milk can have a positive effect on tolerance of pain. I suppose the next question is how this could be used. I think for most patients who can tolerate drops of milk in the mouth that would be the preferred method as one would get two senses involved in taste and smell. Having said that there are infants who may not be able to tolerate even a few drops of milk due to poor gag or handling of secretions. What this study adds I suppose is that even have a few drops of milk on filter paper can make a difference to tolerance of pain.
Might this be something that people would prefer to use for a baby who is ventilated or on CPAP? Maybe depending on local unit practices and risk tolerance. At the end of the day though what we have learned here is that our sense of smell is a powerful thing and can modulate how we perceive and react to painful stimuli. As I often say, breast milk is a powerful thing.
It seems so simple doesn’t it. Shouldn’t we just be able to feed milk whether it be from humans or cows and our preemies will just adapt? I have often written about human milk diets vs those with bovine but this week an intriguing article came my way that really gave me some pause to say hmmm. Human milk diets have been shown to reduce the risk of necrotizing enterocolitis (NEC) compared to use of formula. The use of bovine human milk fortifiers falls somewhere in the middle I suppose as the diet in that case is mostly human milk with some bovine sprinkled in so to speak. If NEC is something that these infants are at increased risk of then what might be going at a tissue level when infants are exposed to human milk alone vs other bovine ingestions?
Near Infrared Spectroscopy May Tell Us the Answer
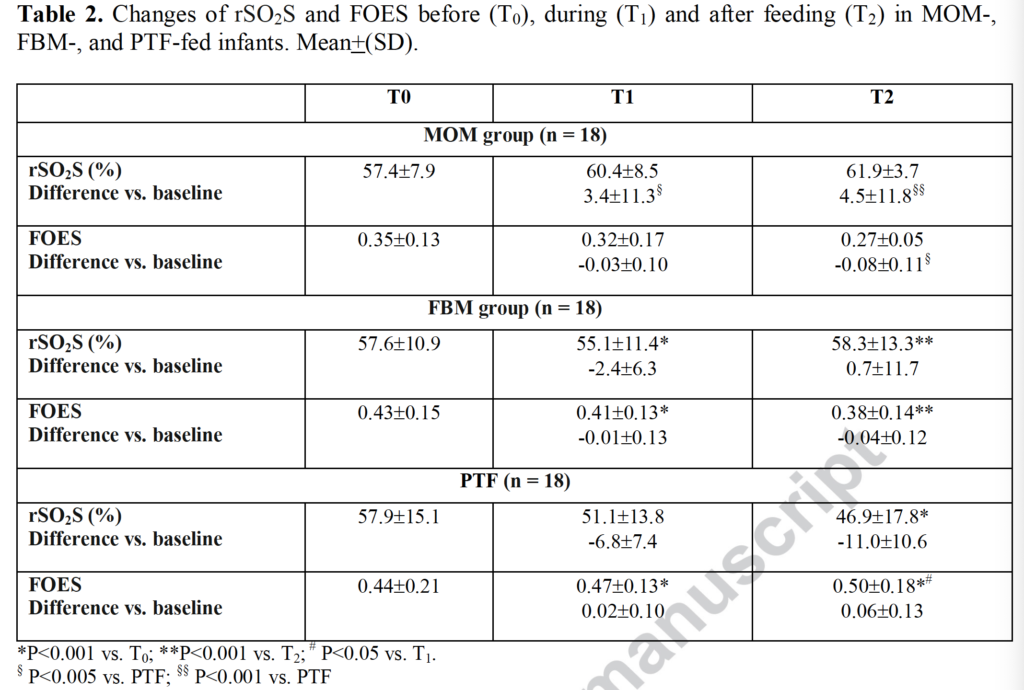
Dani C et from Italy just published an elegant study entitled EFFECT ON SPLANCHNIC OXYGENATION OF BREAST MILK, FORTIFIED BREASTMILK, AND FORMULA MILK IN PRETERM INFANTS. The study looked at the use of two particular measurements from regional splanchnic NIRS application. One is called splanchnic regional oxygenation (rSO2S) and the other splanchnic fractional oxygen extraction ratio (FOES). The rSO2S tells you how much oxygen is in the gut at a tissue level and FOES which is calculated by using systemic oxygenation (SpO2) using the formula (SpO2-rSO2S)/SpO2). So FOES will be high when rSO2S is low meaning the gut relative to the rest of the body is consuming more oxygen. For this study, increments in feedings were standardized for all infants. The study was done once patients were on full bolus feedings for one week.
The authors designed a study that needed 15 infants in three different groups with the first being human milk, then human milk + bovine fortifier and then the last formula fed infants. NIRS data was recorded 30 minutes before a feed (T0), 30 minutes after a bolus feed (T1) and then 2 hours after a bolus feed (T2). In the end the authors recruited 18 per arm. What the authors found is what I am having trouble not running with in terms of its meaning.
Looking at the data, babies who were fed exclusively mothers own milk experienced no change at all in rSO2S at any time points. Interestingly the value even trended higher after a feed. Infants who received fortified human milk experienced a decrease in this value from before the feed to 30 minutes afterwards but then recovered by 2 hours. Formula fed infants though simply dropped from exposure to formula after 30 minutes through 2 hours and the FOES rose over that time demonstrating a greater amount of oxygen extraction by the gut.
What is the meaning of all this?
Bovine sources of nutrition in the form of fortifier seem to cause the gut to become more metabolically active and consume more oxygen at least for the first 30 minutes after a feeding. Formula tends to have a progressive increase in oxygen extraction over the first two hours post feed. This may be reflective of stress in the gut as it works harder to absorb and process nutrients from a bovine source and perhaps in a dose response fashion, a little bovine content as in fortifier causes some short term increase in oxygen demand vs pure bovine formula causing a sustained increase in oxygen need.
This situation sets up an interesting concept. The NIRS results if you recall are from babies who have reached full feeds for one week. What if these same studies had been done in babies who were just in the process of increasing feeds? If infants consuming bovine sources of nutrition need more oxygen in the gut, might this explain why in the presence of acidosis, congenital heart defects or even with a PDA causing changes in end diastolic flow that they don’t tolerate in many cases anything other than human milk?
I am not aware of any such studies looking at feeding advancement but it does really make me wonder what we would see as we advance feedings using our protocols? It is tempting to place abdominal NIRS sensors on the bellies of preterm infants who are just starting out on HMF and see what happens? If the rSO2S was going down and/or the FOES was rising, would you stop the bovine fortification if it reached a certain point? What would happen if a human milk fortifier was used instead of a bovine source? Any difference?
So many questions and in my mind a great area for research. I can’t wait to see where this all goes.
The metabolic syndrome describes the development as an adult of centripetal obesity, high blood pressure, high triglycerides, elevated blood sugar and low HDL cholesterol. These constellation of problems significantly increase the risk of cardiovascular disease, stroke and diabetes.
The theory here is that conditions in utero in which the fetus is chronically deprived of blood flow and nutrition lead to a tendency towards insulin resistance. The body is essentially trying to use any energy it is receiving to stay alive in an environment in which resources are scarce. Given that situation, resisting the effects of insulin by preventing storage of this needed energy serves a useful purpose but in the long run may be detrimental as the body become programmed to resist the effects of this hormone.
What if this programming could be overcome?
Breast milk certainly has many incredible properties and as we learn more we discover only more applications. My previous post on putting breast milk in the nasal cavity is just one such example (Can intranasal application of breastmilk cure severe IVH?). In 2019 Dr. Hair and Abram’s group looked at this with respect to insulin resistance and with potential extrapolation to the metabolic syndrome in their paper Premature small for gestational age infants fed an exclusive human milk-based diet achieve catch-up growth without metabolic consequences at 2 years of age. Texas Children’s Hospital uses an exclusive human milk diet for premature infants with the following criteria GA of <37 weeks, BW of ≤1250 g, with the diet maintained until approximately 34 weeks PMA. Exclusive human milk is provided through a combination of mother’s own milk and Prolacta instead of a bovine based human milk fortifier. In this study they were able to prospectively track 51 preterm infants of which 33 were AGA and 18 SGA. The first visit (visit 1) was performed at 12–15 months CGA and the second visit (visit 2) was at 18–22 months CGA. The question at hand was whether these children would experience catch up growth at 2 years of age and secondly what their levels of insulin might look like at these times. Higher insulin levels might correlate with levels of insulin resistance with higher levels being needed to maintain euglycemia. As a measure of insuline resistance the authors used the calculation of the Non-fasting homeostatic model of assessment-insulin resistance (HOMA-IR) = (insulin × glucose)/22.5 which has been validated elsewhere. Protein intakes were equal for both groups at about 4 g/kg of human milk protein.
The Results Please
The SGA group had greater weight gain between visit 1 and 2 as evidenced by a significant difference in the change in BMI z-score, AGA −0.21±0.84 vs.SGA 0.25±1.10. I suppose this isn’t too shocking as we know that many babies born SGA experience catch up growth after discharge. What is surprising and once again speaks to the power of breast milk is the impact observed on insulin levels and resistance to the same as measured by the HOMA-IR (AGA babies are the left column and SGA the right).
The adjusted p vlaues for glucose were 0.06 with insulin and HOMA-IR being 0.02. What does this mean? Well, these are not fasting insulin levels which would be ideal but what it does say is that at fairly comparable glucose levels the level of insulin is higher in former AGA babies and the level of insulin resistance lower in the SGA infants! This result is quite the opposite of what previous studies have shown as referenced above. Aren’t these growth restricted infants supposed to have had insulin resistance in utero and been programmed for life to have insulin resistance and as adults develop the metabolic syndrome? This study falls short of making any claims about the latter as these infants are only two years of age. What this study provides though is certainly a raised eyebrow. There will be those of course that look at the size of the study and dismiss it as being too small but at the very least this study will lead to further work in this area. This paper though adds to the mystery around the potential impacts of breast milk and certainly provides strength to the thought that perhaps breastmilk should be the exclusive source of nutrition for preterm infants in the NICU. While I understand that not all women are able to produce enough for their own infants or may choose not to for a variety of reasons, with access to donor milk supply this could become a reality. The cost savings to the health care system by preventing insulin resistance would be many fold greater than the cost of donor milk in the newborn period.
Another intriguing question will be whether use of an exclusive human milk diet with use of only mother’s own milk will have similar effects or even greater impact on glucose homestasis later in life. I think the authors are to be commended for their dedication to work in this field and I certainly look forward to the next publication from this group.
A recent post on the intranasal application of breast milk Can intranasal application of breastmilk cure severe IVH? garnered a lot of attention and importantly comments. Many of the comments were related to other uses for breast milk (almost all of which I had no idea about). A quick search by google uncovered MANY articles from the lay press on such uses from treating ear infections to diaper dermatitis. One such article 6 Surprising Natural Uses For Breast Milk certainly makes this liquid gold sound like just that! This got me thinking as I read through the claims as to how much of this is backed by science and how much is based on experience of mothers who have tried using breast milk for a variety of unconventional treatments. I was intrigued by the claim about acne as with several family members nearing that wonderful period of the teenage years I wondered might there have been a treatment right under my nose all this time? Before going on I will tell you what this post is not. This is not going to be about telling everyone that this is a terrible idea. What this is about is breaking down the science that is behind the articles that have surfaced on the internet about its use. I thought it was interesting and I hope you do too!
The Year Was 2009
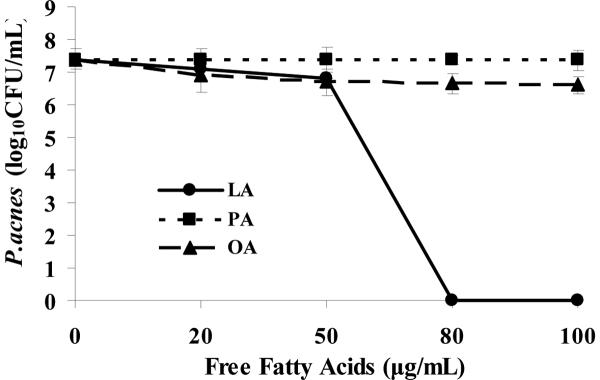
The story begins here (or at least this is the point that I found some evidence). A group of nanoengineering researchers published a paper entitled The antimicrobial activity of liposomal lauric acids against Propionibacterium acnes. The authors examined the antibacterial effect of three fatty acids one of which was lauric acid (which is found in coconut oil but also in breast milk) against Propionibacterium acnes (P. acnes) the bacterium responsible for acne in those teen years. The results in terms of dose response to lauric acid was quite significant.
This is where the link in the story begins. Lauric acid kills P. Acne and it is found in high concentrations in breast milk so might topical application of breast milk treat acne? From what I can see this concept didn’t take off right away but a few years later it would.
Next we move on to 2013
This same group published In vivo treatment of Propionibacterium acnes infection with liposomal lauric acids. in 2013. This time around they used a mouse model and demonstrated activity against P. Acnes using a liposomal gel delivery system to get the Lauric acid onto the skin of the mouse. Interestingly, the gel did not cause any irritation of the mouse skin but using the traditional benzoyl peroxide and salicylic acid caused severe irritation. From this it appears that the news story broke about using breast milk to treat acne as I note several lay press news stories about the same after 2013. Let’s be clear though about what the state of knowledge is at this point. Lauric acid kills P. Acne without irritating skin in a mouse model. As with many early discoveries people can get very excited and apply the same to humans after extrapolation.
What Happened Since Then?
Well, in late 2018 this study was released Design, preparation, and evaluation of liposomal gel formulations for treatment of acne: in vitro and in vivo studies. This is another animal study but this time in the rat which demonstrated application of the gel led to “∼2 fold reduction in comedones count and cytokines (TNF-α and IL-1β) on co-application with curcumin and lauric acid liposomal gel compared to placebo treated group.” Essentially, comedones were reduced and markers of inflammation. So not only do we see an antimicrobial effect, once the bacteria are erradicated, there is a clinical reduction in acne lesions!
Where do we go from here?
This story is still evolving. Based on the animal research thus far here is what I believe.
1. Lauric acid a fatty acid found in breast milk can kill P. Acne.
2. Lauric acid provided in a gel form and topically applied to rodents with acne can achieve clinical benefits.
3. Whereas current standard treatments of benzoyl peroxide and salicylic acid cause inflammation of the skin with a red complexion, lauric acid does not seem to have that effect.
These are pretty incredible findings and I have no doubt, pharmaceutical companies will be bringing forth treatments with lauric acid face creams (they already exist) with a target for acne soon enough. The question though is whether families should go the “natural route” and apply expressed breast milk to their teenagers face. Aside from the issue of whether or not your teenager would allow that if they knew what it was the other question is what might grow on the skin where breast milk is left. I am not aware of any further studies looking at other bacteria (since P. Acnes certainly isn’t welcome around breast milk) but that is one potential concern.
In the end though I think the research is still a little premature. We don’t have human trials at this point although I suspect they are coming. Can I say this is a terrible idea if you are currently using breast milk in such a fashion? I suppose I can’t as there is some data presented above that would give some credibility to the strategy. I am curious for those who read this post what your experience has been if you have used breast milk for acne or for other skin conditions.
It isn’t often in Neonatology these days that something truly innovative comes along. While the study I will be discussing is certainly small I think it represents the start of something bigger that we will see evolve over the coming years.
There is no question that the benefits of mother’s own milk are extensive and include such positive outcomes as improved cognition in preterm infants and reductions in NEC. The benefits come from the immunological properties as well as the microbiome modifying nature of this source of nutrition and have been discussed many times over. Mother’s own milk contains a couple of very special things that form the basis of the reason for the study to be presented.
What are neurotrophins and stem cells?
Before discussing the study it is important to understand what these two classes of molecules and cells are capable of. Neurotrophins are molecules that have the capability of promoting growth and survival of neural cells. Included in this class are EGF, brain-derived neurotrophic factor, glial derived neurotrophic factor, nerve growth factor, insulin-like growth factor-1, and hepatic growth factor. It turns out that not only are these found in high concentrations in breast milk but that a woman who produces breast milk at early gestational ages has higher amounts of these substances in her milk. Pretty convenient that substances promoting development of the brain and survival of brain cells increase the earlier you deliver! Stem cells are pluripotent cells meaning that they can develop into pretty much any cell type that they need to in the body. This would come in handy for example if you needed some new cells in the brain after a neurological insult. These are also present in mother’s milk and in fact can represent as much as 30% of the population of cells in breast milk.
The Nasal Cavity and the Brain
Clearly, the distance from the nasal cavity to the brain is relatively short. Without going into exhaustive detail it has been demonstrated in animal models that provision of medications intranasally can reach the brain without traversing the blood stream. This affords the opportunity to provide substances to the neonate through the nasal cavity in the hopes that it will reach the brain and achieve the desired effect. When you think about it, newborns when feeding have contact between the whole nasopharyngeal cavity and milk (as evidenced by milk occasionally dripping out of the nose when feeding) so using an NG as we do in the NICU bypasses this part of the body. Is that a good thing?
Intranasal application of breast milk
Researchers in Germany led by Dr. Kribs published an early experience with this strategy in their article Intranasal breast milk for premature infants with severe intraventricular hemorrhage—an observation. In this paper the strategy;follows; 2 × 0.1 ml of his or her mother’s milk 3 to 8 times a day (0.6 to 1.6 ml total per day). The breast milk was freshly expressed, which means the milk was used within 2 h after expression. The daily application started within the first 5 days of life and was continued for at least 28 days to a maximum of 105 days.
The outcome of interest was whether the severe IVH would improve over time compared to a cohort of infants with severe IVH who did not receive this treatment. Importantly this was not a randomized trial and the numbers are small. A total of 31 infants were included with 16 receiving this treatment and 15 not. The two groups were compared with the results as follows.
The results don’t reach statistical significance but there is a trend at the bottom of the table above to having less progressive ventricular dilatation and surgery for the same. Again this is a very small study so take the results with a grain of salt!
Is this practice changing? Not yet but it does beg the question of what a properly designed RCT might look like. The authors predict what it might look like with a sham nasal application versus fresh mother’s milk. I do wonder though if it may become a study that would be hard to recruit into as when families are approached and the potential benefit explained it may be hard to get them to say anything other than “Just give my baby the breast milk!” Such is the challenge with RCTs so it may be that a larger retrospective study will have to do first. Regardless, be on the lookout for this research as I suspect we may see more studies such as this coming and soon!
* Featured image from the open access paper. (There couldn’t be a better picture of this out there!)