Over the last number of years clinicians have sought more and more to limit the experience of babies to painful stimuli. In the area of surfactant administration this has focused on “less invasive” strategies such as use of small catheters while on CPAP (LISA or MIST) and surfactant via LMA or Surfactant Administration Through Laryngeal or Supraglottic Airways (SALSA) as it is sometimes known. Intubation Surfactant Extubation (INSURE) while not generally included in the less invasive approach is to a degree fitting since it involves at least intubating for a very brief period after surfactant is administered. SALSA has been growing in popularity due to its “extreme” non-invasiveness since babies are receiving surfactant without instrumentation of the airway at all. It should come as no surprise then that head to head comparisons will be done to determine which should be reigned king!
The Contenders
A group out of Albany, NY has looked at SALSA vs INSURE before in which they used morphine for premedication prior to the procedure. You might ask why any premedication is needed at all but I would suggest that covering one’s airway and dripping liquid into it might cause some irritation so why not keep them calm. The authors in their paper Randomized trial of laryngeal mask airway versus endotracheal intubation for surfactant delivery found a high rate of failure in the intubation arm which more than likely was attributable to the respiratory depressive effect of the same.
This time around in the current paper Randomized Trial of Surfactant Therapy via Laryngeal Mask Airway Versus Brief Tracheal Intubation in Neonates Born Preterm they switched to remifentanil for its brief duration of action. Babies in the SALSA arm received that drug while those in the ETT group received atropine as well. The authors included infants born from 27 weeks to 36 weeks gestation who were larger than 800g at birth. This was a non-inferiority trial with the primary outcome being Our primary outcome was failure of surfactant therapy to prevent the need for invasive mechanical ventilation or its surrogate indicators, namely, more than 2 doses of surfactant therapy, sustained need for FiO2 >0.60 to maintain target O2 saturations, or a second dose of surfactant within 8 hours of the first dose.
Surfactant redosing criteria were the same for both groups: FiO2 >0.60 or FiO2 >0.30 with clinical signs of worsening RDS. If surfactant needed to be given a second time it was via intubation. The decision to ultimately intubate though was in the hands of the practitioners.
Unfortunately, the trial was stopped after only 51 patients were enrolled into the LMA and 42 into the INSURE groups respectively. Randomization was by block design and the authors were looking for 130 patients per group so they fell far short of that. The reasons for falling short were interesting as they demonstrate one of the challenges of research and changing beliefs. At the start of the trial there was equipoise among practitioners with respect to the two modes of surfactant delivery but part way through people preferred SALSA. The authors changed the randomization to try and deal with that to a 2:1 favoring SALSA but with the combination of that and COVID they had to stop. They did manage to get enough though to determine the primary outcome in spite of this.
What did they find in the end?
Well first of all it is worth noting that there were no differences in baseline characteristics between the two groups. As it turns out, while the numbers were small it didn’t seem to lead to an unbalancing of groups.
With respect to inferiority the finding was that it was in fact not inferior as per the figure below.
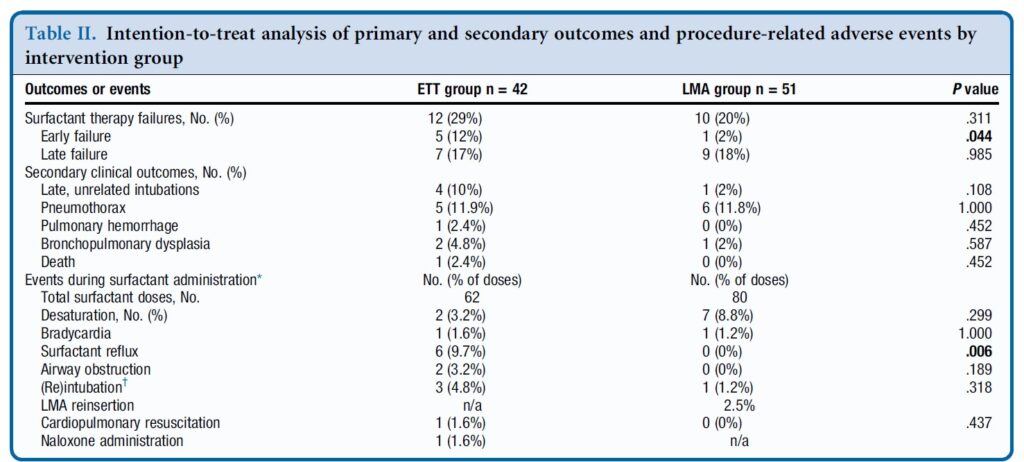
In table 2 some interesting findings emerge
Early failure of surfactant which was defined as within 1 hour of surfactant administration was found to be significantly increased in the intubation group. Late failure through at 5 days of age was not any different. An early failure is suggestive of the procedure not working to deliver the surfactant. When you look at the bottom half of table 2 the answer may be there. As part of the planned procedure the authors aspirated a gastric tube after surfactant administration to ensure that it went to the right place. There was no difference in surfactant volume aspirated via this route. There was however 9.7% of infants in the ETT group that experienced reflux in the ETT vs zero with observed reflux in the SALSA group (in the mouth perhaps?). Is surfactant without PPV better tolerated maybe?
There was a trend overall to more failures in the ETT arm although this was not found to be significant either in the intention to treat or per protocol analysis.
Where do we go from here?
First off it is important to look at who was chosen for this strategy. You may have noticed that there were no micropreemies in this trial. The reason for this is likely two-fold. The first is that prior trials on SALSA have found it doesn’t work as well to prevent intubations in babies below 27 weeks. This is very similar to the findings of studies using aerosolized surfactant. It may well be that there just isn’t enough of the total dose getting to the alveoli. If you can get some of the dose in deep into the lung for those with less severe RDS it may work ok for those babies. The second reason likely has to do with using LMAs in those in that weight range as they generally are designed for larger preemies although I understand smaller ones are becoming more readily available.
The second point is that this was not a blinded study. This could have become an issue as the authors acknowledge that there was a growing institutional preference for SALSA as the study went on. If the Neonatologist subconsciously believes it is better, might that have influenced some of the decisions to intubate again since one of the criteria was “clinical signs of worsening RDS”. It is quite possible this could have led to a few more intubations in the INSURE group for repeat doses. We can’t prove that but it is a weakness of the study.
At the very least it can be argued that the use of SALSA works as a small percentage overall failed the procedure. The largest groups of infants though were above 29 weeks so we also might not expect a high rate of failure after one dose though. It works but how well is tough to say.
Where I think this study is really important though is what it tells us for centers in particular who don’t intubate as often. Intubation is a skill that is declining in opportunity, both because of a turn to more use of non-invasive support as a primary mode of treatment. It also has become scarcer at an individual level due to there being more practitioners who can perform the skill. Having an option to use SALSA for those who aren’t as comfortable with intubation will no doubt be of much interest to many in this situation.
What is no doubt going to come next is the LISA/MIST vs SALSA trials. I hope that in the future pain scores are included in these sorts of analyses to really determine if in being less invasive we are also ensuring that we are also not undertreating discomfort. I suppose the lesson being learned from all of this is that less very well may be more.
This is the one as the saying goes that you have all been waiting for! Poractant entered the scene in Canada a few years ago with a lot of promise as a great alternative to the bovine source generally used here. The volume of administration was about half and as the use of MIST/LISA rose in popularity the option to use the lower volume was of interest to many. A study out of London Ontario demonstrated however that the bovine form could be used for LISA/MIST successfully and was written about in Less Invasive Surfactant Administration with High Volume Surfactant.
What about if we look at a real head to head comparison looking at meaningful outcomes like length duration of respiratory support? To do so would require a fairly large sample and would generally be difficult to accomplish but us Canadians opted for a study design to allow this to move forward with a sample size that for a neonatal study I think at least were admirable!
The Study
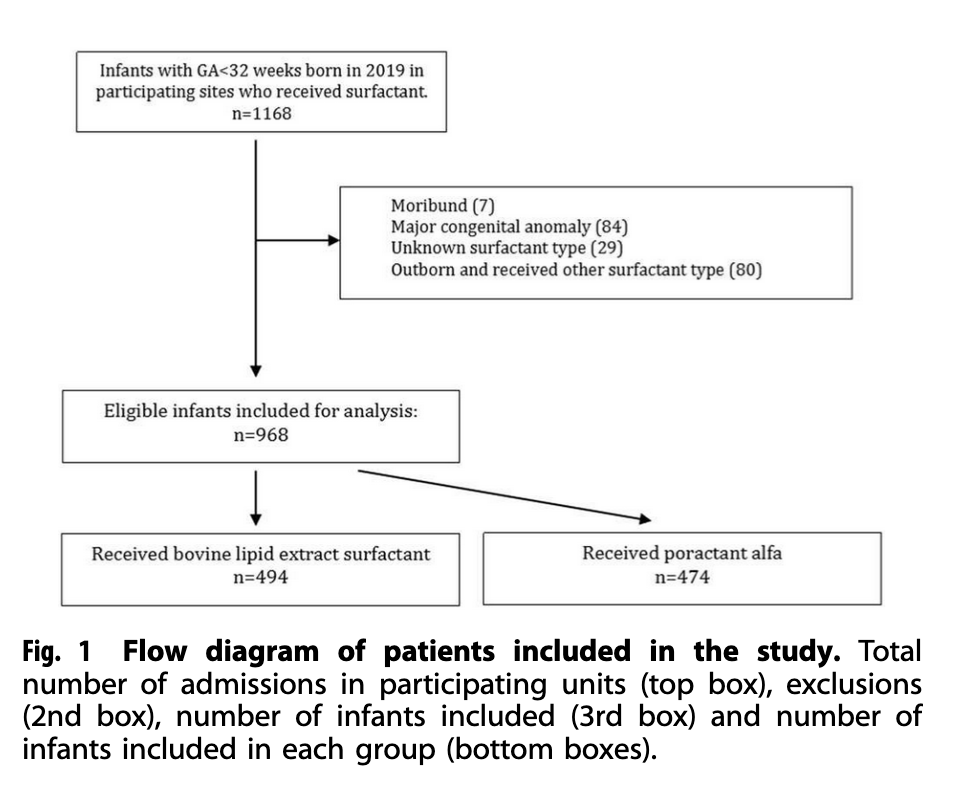
The study design here was a prospective comparative effectiveness cohort study of babies all born under 32 weeks at 13 NICUs across Canada. The study in question was entitled Poractant alfa versus bovine lipid extract surfactant: prospective comparative effectiveness study and is authored by many I consider colleagues and friends! To do this study each centre agreed to start off for 6 months with the bovine surfactant for any baby that had respiratory distress syndrome and in the opinion of the team needed surfactant. After that period each centre switched to poractant for an additional 6 months. This was a pragmatic trial designed to be less rigid with respect to criteria for intubation and allow for a “real world” determination of effect of using one surfactant vs another. While the study was not randomized the collection of outcome data relied on trained abstractors for the Canadian Neonatal Network in each centre. The authors determined that to see a difference in the primary outcome would require 484 patients per surfactant group. What they obtained in terms of recruitment is shown below.
The Results Please
I realize you have been waiting with excitement about what they could have found. Sadly they didn’t find too much!
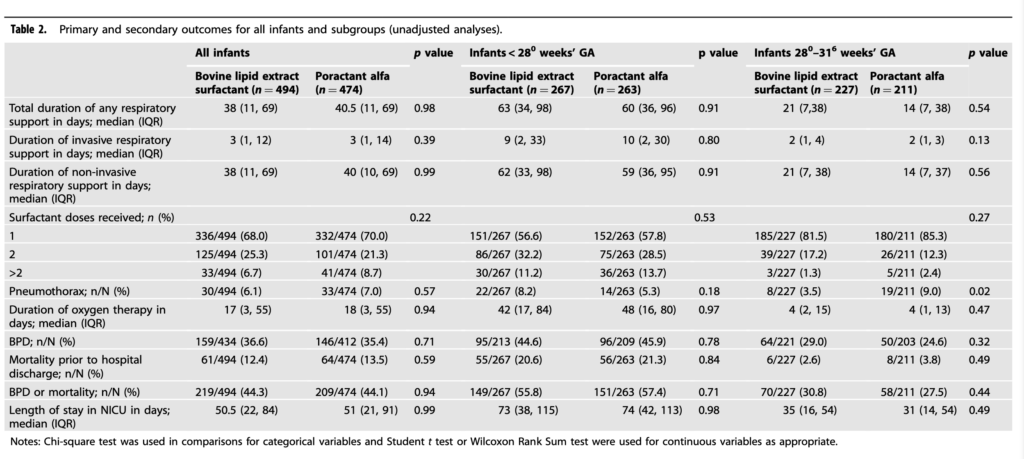
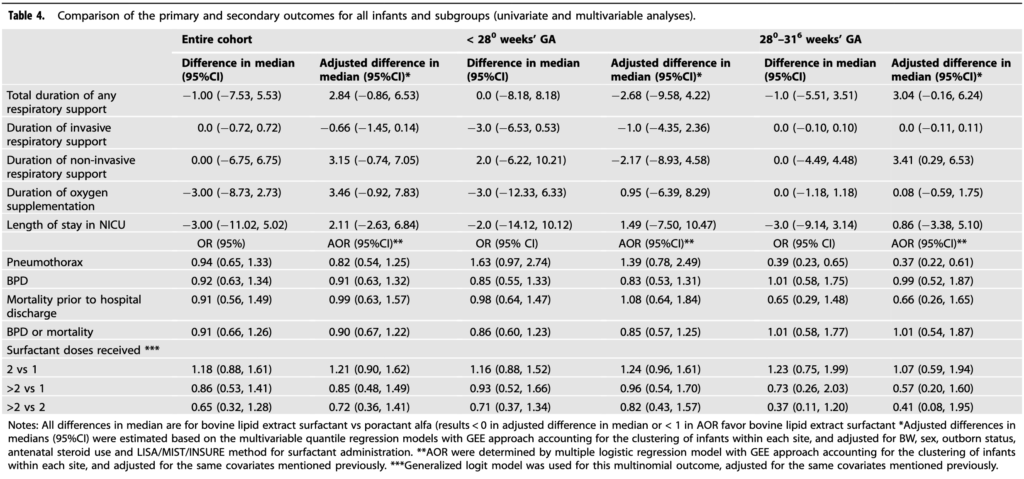
There was no difference in length of ventilation or for that matter some important outcomes like number of doses of surfactant needed (if one group needed more might they be less effective), BPD, mortality and length of stay. The authors did note a difference in rates of MIST/LISA favouring the poractant group but when they controlled for that variable still found no difference in outcomes. Important to note that though since use of MIST/LISA may reduce the outcome of interest itself but alas no difference.
As with many studies people start digging and looking at secondary outcomes to see if there is anything of interest that pops up. It is worth noting here that whatever is found based on this study design would be an association so one must be careful not to jump to causation which may or may not be at play. For fun though let’s look at a couple of things that cropped up.
When you look at the subgroup of babies 28 +0 to 31+6 weeks an increased rate of pneumothorax creeps into the picture if you received poractant. On the other hand a reduction in days of non-invasive ventilation in favour of poractant comes into play for the same cohort. There of course is the possibility given these are secondary outcomes that these came about by chance. I did find it interesting about the pneumothorax issue though as early in the study when our centre was using poractant questions came up from our staff about a perceived increase in pneumothoraces with use of poractant. In other words the findings are in keeping with what our own units experience was so I can’t help but wonder if there is something there!
What the study does in my mind is demonstrate that if you wish to use either surfactant you may. I suppose then it comes down to comfort and in part whether you believe that use of a lower volume surfactant is better for administration with MIST/LISA. If that is the case then your choice would be poractant. If you don’t care however then it may come down to cost. There has been a difference in cost but I do wonder if the gap may close with demonstration of similar efficacy in this study. If people are indifferent to utility of the two then cost will certainly be a variable to consider!
If there is a country that leads this site in terms of mentions it has to be Sweden. This isn’t just because I happen to know some Neonatologists from there who are fine people but because of the fantastic research that spills forth from their national registry of births. Surfactant is one of the oldest treatments we have in Neonatology and we know that in babies with RDS giving it early within 2 hours has benefits such as reduction in pneumothorax. The reality though is that as we have become familiar with the therapy its use has spilled over to other conditions. Years ago use of surfactant in meconium aspiration syndrome was shown to reduce need for ECMO. It has also been shown to imrove clinical condition in babies with pneumonia. Interestingly as a fellow I was criticised one call night for wanting to give a three day old baby with a history of RDS and high FiO2 requirements a repeat dose of surfactant. That was in 2001 and at that time no one could believe I was suggesting such an odd thing to give a dose after 48 hours yet now this is commonplace. Again as we have become more comfortable with surfactant such “off label” use spreads. I am not being critical of my colleagues back in 2001 as that was what the “conventional wisdom” was with respect to surfactant but that was then and this is now.
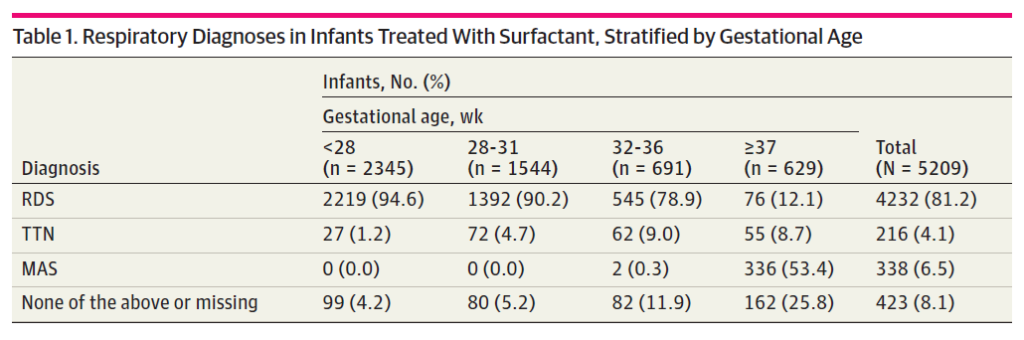
Looking at their registry data for 97377 infants born from 2009-2018 they found 7980 surfactant administrations to 5209 infants. The reasons for surfactant administration are shown in the table 1 below from the paper. Clearly and not surprisingly the bulk of surfactant administration is for RDS especially as gestational age declines. Given that so few preterm infants will pass meconium in-utero it also is understandable why MAS clusters in the more mature babies.
When it comes to multiple surfactant administrations they found 59.2% received 1 administration, 25.8% received 2, 7.3% had 3, and 2.8% had 4 or more administrations. Not surprisingly the more immature infants were more likely to receive multiple administrations. I have to say at this point that I feel vindicated with that suggestion for late surfactant administration all those years ago as these extra doses would have been given up to days after the first dosing.
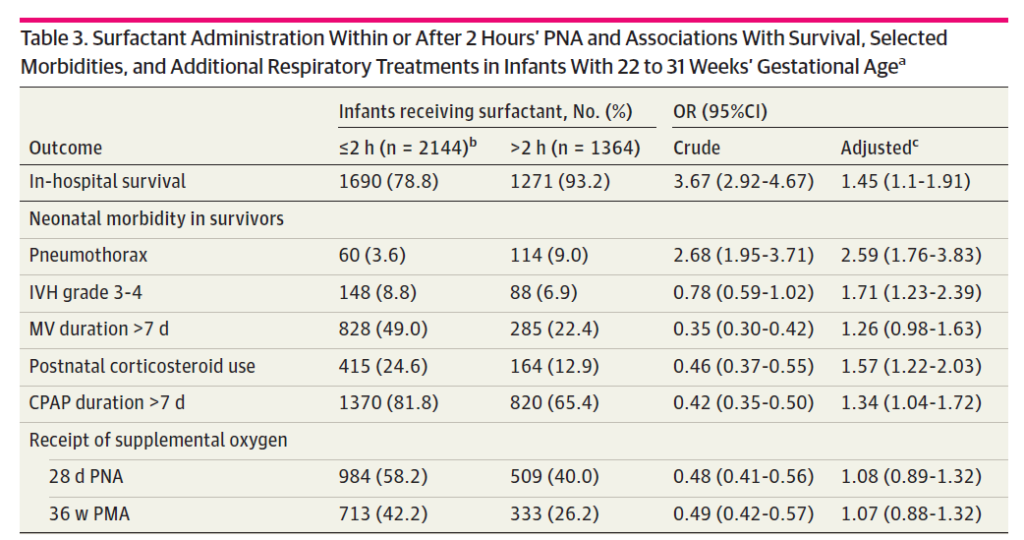
Now Here Comes The Interesting Part
Much like previous work before this study, delivery of surfactant within the first 2 hours of age was associated with a reduction in very important outcomes of pneumothorax, IVH and need for ventilation beyond 7 days.. In short, improving compliance has a lot of benefits! The surprise was the in-hospital survival which favoured giving surfactant late. Put another way, if you receive surfactant in the first two hours you are more likely to die in hospital.
How can that possibly be if provision of surfactant has all those benefits outlined in table 3? More on that in a bit.
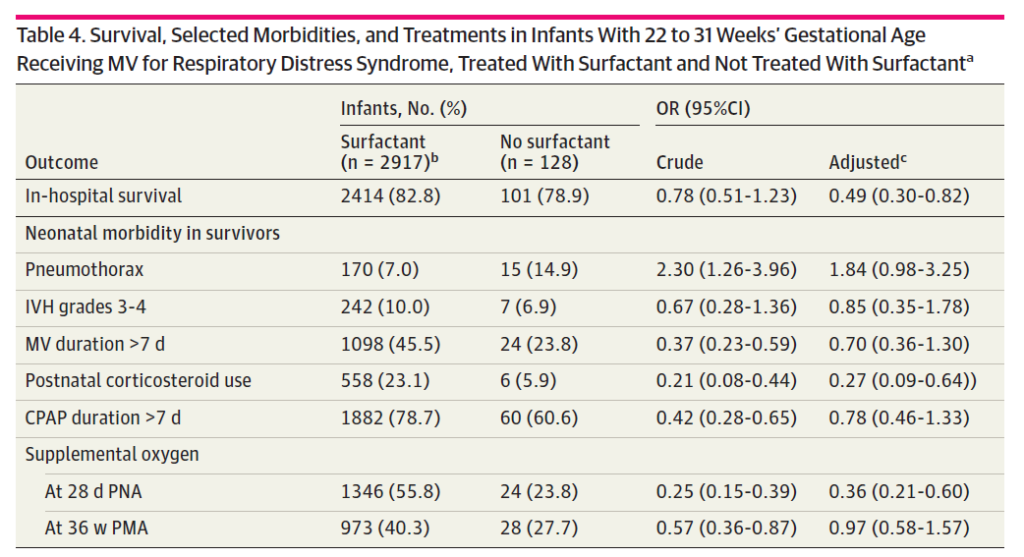
The next table addresses another question which is what if you don’t get surfactant at all? Interestinly the in-hospital survival is better for that group as well. On the other hand no difference exists for pneumothorax or IVH and ventilation beyong 7 days is improved with no surfactant at all!
The Difference Between Association and Causation
Ultimately that is what I think is at play here. You could look at the information quickly and conclude that giving surfactant late or not at all improves your chances of survival! Maybe aggressive use of surfactant isn’t such a good thing after all. I think you would be wrong there though based on prospective randomized trials. What is happening here is that the baseline characteristics are not likely equal and you are really looking at three different groups of patients.
Group 1 – These are the ones who get surfactant early within 2 hours of life. My suspicion is that the number of babies in this group that are really sick who may also have other comorbid issues is higher. There might be some babies with servere IUGR, pulmonary hypoplasia, meconium aspiration or pleural effusions that made the resuscitating team so nervous that they in advance of delivery had surfactant thawing and ready to go. Yes overall this group might benefit from better compliance and have less pneumothoraces for example but their comorbid conditions put them at higher risk of death.
Group 2 – Surfactant given after 2 hours of age. These are likely babies who are not as sick as group 1. Maybe they are babies initially managed with CPAP or NIPPV who due to escalating FiO2 requirements get surfactant. Much less likely to die.
Group 3 – No surfactant needed at all. The reason there might not be a difference in the major morbidities is that while they have RDS, TTN or MAS they are mild in nature. Clearly very low risk of death here and for that matter complications.
It might have been helpful to have some meaures of acuity documented such as SNAPPE-II (Score for Neonatal Acute Physiology with Perinatal Extension-II) used as it would help us in figuring out such differences.
Overall I think the message remains the same. Give surfactant early for those with significant lung disease. What I think it adds is an awareness that repeat dosing even if off-label is being done in Neonatology. The next question will be whether this repeat dosing makes the babies better or just us!
Intubate-Surfactant- Extubate or INSURE has been around for awhile. The concept is to place an ETT while an infant is first on CPAP and then after pushing surfactant in quickly remove the ETT and put back on CPAP. This does not always go as planned though. If after surfactant the FiO2 remains above 30% many people would keep the ETT in place as they would surmise that the infant would fail if the tube was removed. They would probably be right.
Sustained inflations have fallen out of favour ever since the SAIL trial results were published and written about here . Having said that, the concept of using sustained inflation is to open the lung and expand closed alveoli to improve both oxygenation and gas exchange. Much like giving inhale nitric oxide to a collapsed lung is unlikely to make much difference, the question could be asked whether giving surfactant to a lung that is most collapsed will fail to deliver this compliance improving medication to the areas of the lung that most sorely need it. Our Italian colleagues therefore decided to undertake a study to look at providing surfactant to lungs after a recruitment manouver and see if this made a difference to the meaningful outcome of extubation failure after surfactant provision. The results are intriguing and as such here we go in looking at the study.
Optimizing Lung Expansion
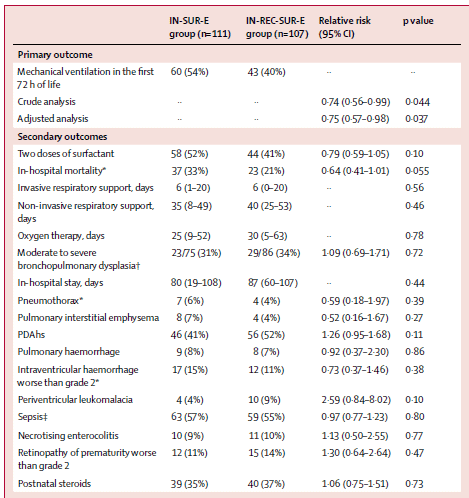
The trial is the Lung recruitment before surfactant administration in extremely preterm neonates with respiratory distress syndrome (IN-REC-SUR-E): a randomised, unblinded, controlled trial and involved 35 NICUs in Italy. All infants enrolled were born from 24 + 0 weeks to 27 6/7 weeks gestational age at birth and all < 24 hours of age at enrollment. Each baby had to be on CPAP at the time of randomization and meet prespecified failure criteria of FiO2 of 0·30 or greater for target SpO2 of 87% to 94% for at least 30 min or in 10 Infants for rapid deterioration of clinical status or if pCO2 was > 65 mm Hg with a pH less than 7·20. Regardless of which arm they were randomized to all infants received 1-2 sustained inflation breaths using 25 cm H2O for 10-15 secs using a t-piece resuscitator after being started on CPAP as was the practice at the time. After randomization which could not be blinded, patients were then either given surfactant via INSURE without any further strategy for opening the lung or received the IN-REC-SUR-E approach. The latter involved putting the infant on high frequency oscillation starting with settings of mean airway pressure 8 cm H2O; frequency 15 Hz; ΔP15 cm H2O; and inspiration to expiration ratio of 1:2. Using this modality infants underwent stepwise recruitment methods prior to administering surfactant (poractant). The primary outome was the need for mechanical ventilation within the first 72 h of life. Infants met the primary outcome if they were not extubated within 30 min after surfactant administration or required reintubation before 72 h of life.
The Results
Based on a power calculation the authors needed 103 infants in each arm and they recruited 107 in the treatment and 111 in the control arm. In the per-protcol allocation 101 received the treatment and 111 the contol. While the strategies for extubation were not set out to be equal (units were allowed to extubate to anywhere from +6 to +8 for pressure levels), the groups were not different 7·0 cm H2O, SD 0·4 for the experimental group and control arms. Given the steps taken to open the lung in the lung recruitment arm, the FiO2 was lower at 28% prior to surfactant provision in the treatment group than in the usual INSURE approach at 42% prior to surfactant provision. All infants were extubated within 30 minutes of receiving surfactant. As the results demonstrate, whether there was an intention to treat analysis or per-protocol analysis the babies who received the intervention were more likely to remain extubated. The number needed to treat was 7 which is a pretty powerful measure. Interestingly, looking at secondary outcomes there are some interesting trends as well including less mortality which on a per-protocol analysis was significant but also a trend towards more PVL at 9% in the treatment arm and 4% in the control. The mean times to surfactant administration were 4 hours in the treatment group and 3 hours in the control but the high frequency manoeuvre had a mean duration of only 30 minutes. It is possible that the use of high frequency could have blown off CO2 to very low levels but I am uncertain if the short reduction in pCO2 could have contributed significantly to reduced cerebral perfusion if that trend is representative of something. Interestingly, pneumothroaces were not different between groups as no doubt as a reader you might wonder if use of high pressures to recruit the lungs when they are non compliant might have led to air leaks.
So it worked, now what?
First of all, the results to me make a lot of sense. Opening the lung before delivering surfactant and then seeing better chances of staying extubated doesn’t really surprise me. Some questions that come up now for me would be how this strategy would fare in those who are older at birth. I suspect given the greater chest wall support and lower likelihood of severe RDS this strategy might be even more effective at reducing FiO2 or perhaps CPAP need in terms of duration after extubation. I would think it unlikely to make a difference in reintubation though as most would remain extubated regardless. That is for another study though with a different outcome.
There will be centres that don’t like the use of HFOV for recruitment so what other strategies could be used in lieu of this? I hate to say it but there will also be calls to have a much larger study specifically designed to look at the secondary outcomes. Would a larger study find a significant increase in PVL or demonstrate that it was just a random finding? Might mortality be proven to be lower and even more so?
Regardless of the above what I think this paper does is give us reason to pause before giving INSURE and ask ourselves if we have done what we can to open the lung after intubating before rushing to squirt the surfactant in. Maybe increasing the provided PEEP and lowering the FiO2 somewhat before giving surfactant will help with distribution and increase your chances of first being able to extubate and secondly when you do keeping the tube out!
I have written about non-traditional methods of providing surfactant to newborns previously. The practice of intubating a preterm infant to administer surfactant and leaving the endotracheal tube in with a slow wean of ventilation is mostly a thing of the past (at least in my units). Strategies have evolved and have seen the development of the INSURE technique, LISA methods, use of an LMA to delivery surfactant and even simple deposition into the pharynx all with variable success.
Poractant alfa at 200 mg/kg was used in this study and delivered via aerosolization using a vibrating membrane called the eFlow. The authors chose to look at infants from 29 0/7 to 33 6/7 weeks at birth and stratified them into two groups of 29 0/7 to 31 6/7 and 32 0/7 to 33 6/7 weeks. They estimated a need for 70 babies based on an anticipated failure rate of 30% in the control group vs 5% in the treatment group. Unfortunately, due to several reasons the study was only able to recruit 64 babies for randomization before being stopped due to the recruitment issues. The design of the study included adequate blinding with a sham procedure and there were predefined “failure criteria” necessitating intubation at the outset of the study. These criteria are acceptable to me as they are similar enough to my own practice and were:
1. FiO2 >0.35 over more than 30 min OR FiO2 >0.45 at
anytime.
2. More than four apnoeas/hour OR two apnoeas requiring bag
and mask ventilation.
3. Two capillary blood gas samples with a pH <7.2 and partial pressure of carbon dioxide >65 mm Hg (or partial pressure
of carbon dioxide in arterial blood (PaCO2) >60 mm Hg if
arterial blood gas sample).
4. Intubation deemed necessary by the attending physician.
What did they find?
The primary outcome CPAP failure within 72 hours of birth was indeed different in the two groups.
CPAP failure by 72 hours
CPAP + surfactant
11/32 (34%)
CPAP
22/32 (69%)
(RR (95% CI)=0.526 (0.292 to 0.950))
Clearly the event rates were quite off from what they expected in the power calculation but given that they found a difference as opposed to no difference at all the fact that they didn’t recruit the numbers they planned is of less importance.
However, what is interesting is when they looked at the planned analysis by stratification an interesting finding emerged.
Group 1 (29 0/7 to 31 6/7)
CPAP failure by 72 hours
CPAP + surfactant
12/21 (57%)
CPAP
12/19 (63%)
(RR (95% CI)=0.860 (0.389 to 1.90))
Group 2 (32 0/7 to 33 6/7
CPAP failure by 72 hours
CPAP + surfactant
1/11 (9%)
CPAP
10/13 (77%)
(RR (95% CI)=0.254 (0.089 to 0.727))
There were a number of secondary outcomes looked at as well which may be of interest to you but as the numbers here are quite small I will not comment other than to say there was no increased incidence of complications with surfactant administration in this fashion. Also for those who ultimately failed CPAP the time when they did so was quite delayed compared to CPAP alone. Age at intubation for nCPAP failure, hours 4.9 (2.7–10.6) 11.6 (9.0–31.1) 0.008*
What can we take from this?
I believe these results are encouraging even if the study is a small one. The message I take from this study is that aerosolization of surfactant delivers some amount of product to the lungs. Those with more significant RDS or smaller lungs (those in the 29 0/7 to 31 6/7 group) may not get enough surfactant to treat their RDS sufficiently to avoid intubation. Those with less significant RDS or a larger number of alveoli get “enough” of a dose delivered to the alveoli to make a difference and avoid intubation. It is worth stressing that there can be no specific comment about using this strategy in even more immature infants as they weren’t tested. If I had to guess though, I would expect no difference given the findings in the smaller group.
As a physician responsible for transport though I am interested in the potential benefits to those born in non-tertiary centres. Many centres lack individuals with the confidence and skill to regularly place endotracheal tubes. For these centres it may be that providing nebulized surfactant could delay the time to treatment failure, allowing more time for a trained transport team to arrive. Training of course would be needed in these centres on how to administer surfactant in this way but it is an interesting concept to consider. With a near tripling of the average time to treatment failure the extra hours on CPAP would be much appreciated when weather delays or difficulty securing air assets means long delays in transport team arrivals.
To be sure this isn’t the last study of this kind but it certainly is an interesting start and one that will no doubt produce questions that will help formulate the next study design.