If you work in Neonatology or in Pediatrics for that matter there is no doubt that at some point you took the neonatal resuscitation program (NRP). Ideally you should be recertified every year or two years depending on your profession. In the course you are taught that the depth of chest compressions required to achieve the best chances of ROSC is 1/3 the diameter of the chest. The evidence to support this comes from a CT evaluation of neonatal thoraces in the paper Evaluation of the neonatal resuscitation program’s recommended chest compression depth using computerized tomography imaging. In this study the authors found that using a mathematic model the 1/3 chest compression recommendation should in theory yield the best hemodynamic outcome.
What about ROSC?
Hemodynamics is one thing in a model but what about real life? I don’t think you could reasonably do an RCT these days with the outcome of interest being ROSC in humans. What research ethics board would allow you to randomize to the outcome of death in babies and deviate from an international organizations recommendations for best practice? My former colleagues in Edmonton had an answer to this issue though by using a piglet model to test the hypothesis that 33% is indeed better than either 12.5%, 24% or 40% chest compression depth. Their paper Assessment of optimal chest compression depth during neonatal cardiopulmonary resuscitation: a randomised controlled animal trial tackles just that question.
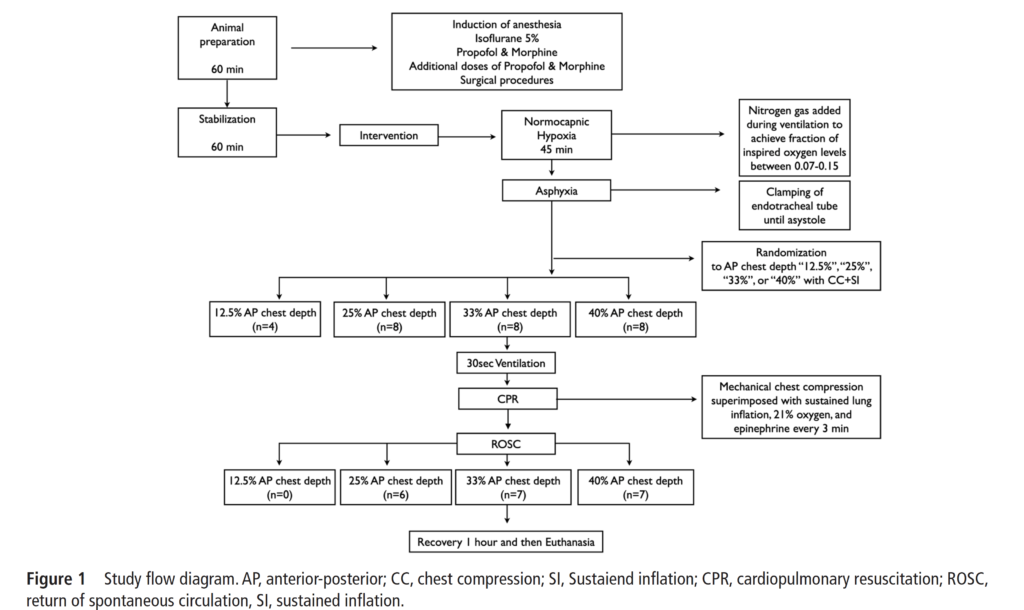
How did they do it? In an animal lab that is equipped with a mechanical device to simulate chest compressions they were able to instrument piglets and after asphyxiating them with an occluded ETT they began the process of trying to revive them. After being asphyxiated they initiated a combination of PPV with a neopuff and gave epinephrine (0.02 mg/kg/dose) intravenously2 min after the start of positive pressure ventilation and every 3 min until ROSC with a maximum of three doses, with a maximum resuscitation time of 10 min. The groups were divided in the following manner.
What did they find?
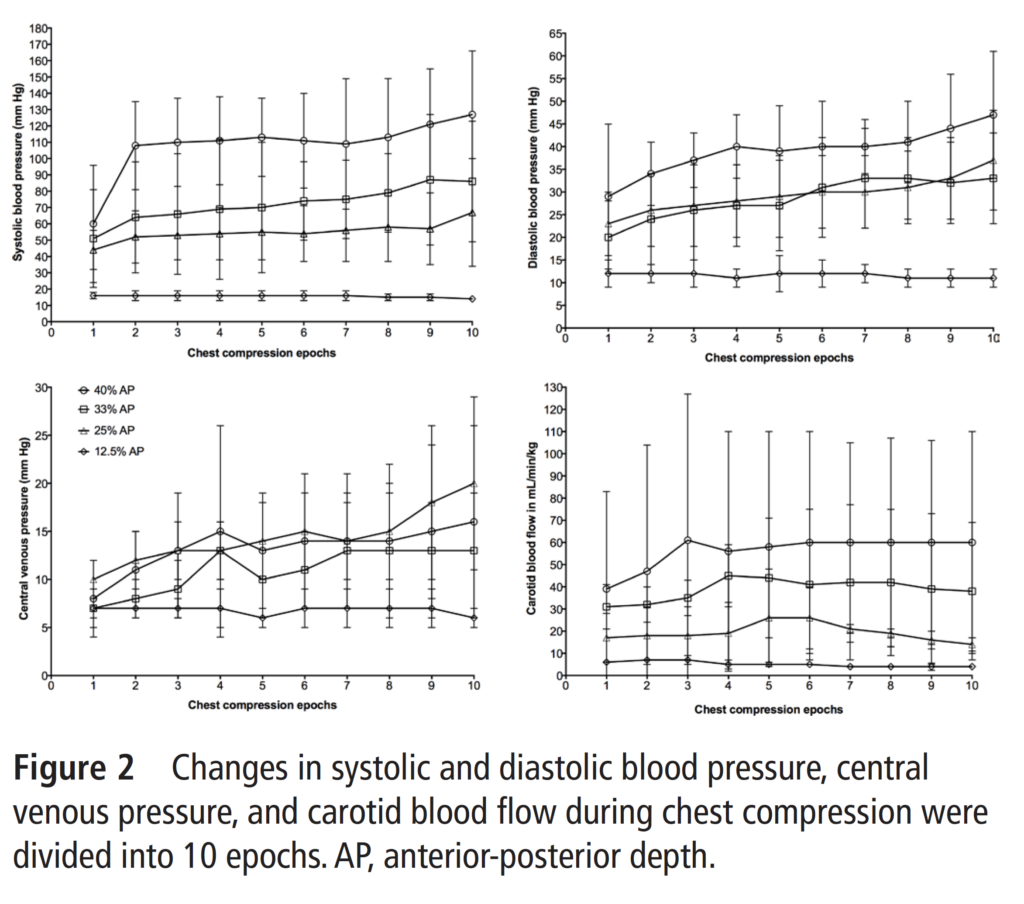
Two very interesting things came out of the study. The first was that they abandoned the 12.5% group early in the study when it became apparent that no piglet would survive using this depth. The other thing they found in support of greater depths of 33 and 40% compression depth is shown in the following graph.
The authors found that in terms of systolic and diastolic blood pressure the best chances in particular for systolic blood pressure were the 33 and 40% compression depths. Looking at the bottom right figure it is also evident that cerebral blood flow increases with increasing depth of compression.
With respect to the primary outcome they found this:
“The median (IQR) time to ROSC was 600 (600–600) s, 135 (90–589) s, 85 (71–158)* s and 116 (63–173)* s for the 12.5%, 25%, 33% and 40% AP depth groups, respectively (p<0.001 vs 12.5% AP depth group). The number of piglets that achieved ROSC was 0 (0%), 6 (75%), 7 (88%)** and 7 (88%)** in the 12.5%, 25%, 33% and 40% AP depth groups, respectively (*p<0.05 and **p<0.005 vs 12.5% AP depth group).
Of note, one of the piglets randomized to 40% depth of compression had pulmonary contusions at autopsy.
Putting it all together
The article supports the use of 33-40% chest compression but it raises an important point in my mind. The study used a mechanical device to ensure the percentage compression and it is clear that if you fall below these numbers the ROSC and hemodynamics is impaired while if you go to high you run the risk of damaging the lungs (I know it was just one but a previous study demonstrated harm at 50% compression depth as well).
This raises the question about failed resuscitations. Do we know how deep we are actually compressing during these situations? Sure, everyone can recite that we should be compressing to 1/3 of the chest diameter but what are we actually doing? In some cases are we not doing enough and in other cases doing way to much? I would imagine the answer to this question is yes. I do wonder as we continue to automate so much in our world through advances in technology if doing the same in neonatal resuscitation is not that far off. When our hands are sweaty and tremulous with adrenaline coursing through our veins how good are we really at controlling the precise depth of compression. Time will tell what happens but what is clear to me is that precision matters and really how precise can we be?
I recall the shock waves through the neonatal community when ILCOR changed its recommendation to stop routine intubation of non-vigorous infants born through meconium. The rationale again was that for most practitioners it would be better to give bag valve mask ventilation and establish a functional residual capacity than try and intubate and start with a collapsed lung.
Oommen VI et al wrote a brief report on their experience in the UK with the change as recommended for these infants. Their brief publication has a large cohort that is looked at and one result in particular I found interesting enough to share with you today. The publication is Resuscitation of non-vigorous neonates born through meconium-stained amniotic fluid: post policy change impact analysis. The authors looked prospectively at the “new approach” group from October 2016-September 2017 and compared their outcomes to the retrospecitve cohort in the same hospital from August 2015-July 2016 as the “old approach” group.
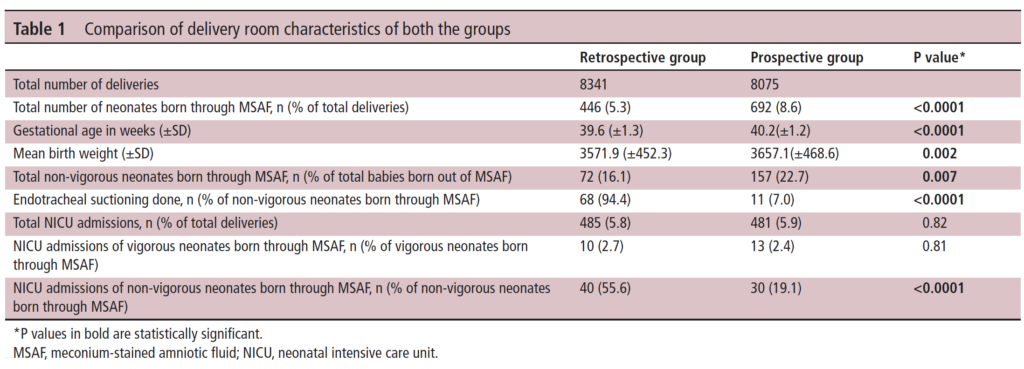
As you can see in Table 1 they saw a lot of deliveries during this time that were complicated by meconium. This gives us a good before and after comparison and while not all prospective and ensuring that practices were otherwise the same it is a pretty decent sample to look at. I like seeing that 7% of the group in the new approach still received endotracheal suctioning. It is worth remembering that what the recommendation says is to not do this routinely but if the resuscitation is not going well and the baby not responding to ventilation it is reasonable to apply suctioning as they would have done to see if there is any obstructive material in the airway.
It is the last comparison in Table 1 though that drew my attention. Over 50% of the non-vigorous babies needing routine suctioning in the retrospective arm needed NICU admission compared to 19.1% of the new approach group which was quite significant. More on this later.
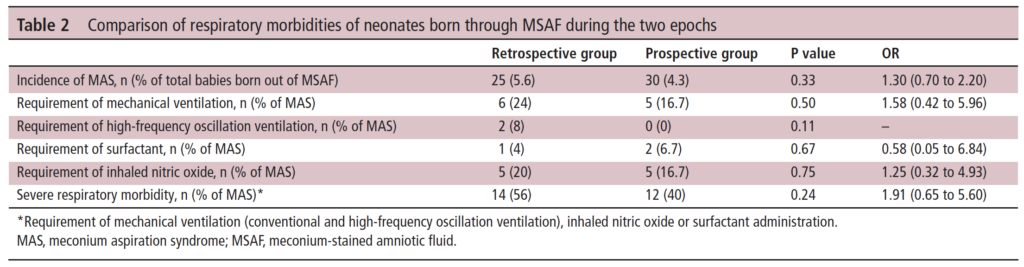
In Table 2 the authors compare the respiratory morbidities showing no difference in rates of ventilation, HFOV, surfactant or iNO. What they are demonstrating is that to the best of their abilities the babies were similar in terms of respiratory morbidiites in a binary sense. What I mean here is that when you ask the question did they need any of these aforementioned things it is a yes or no. What is not easy to pick up from the table is the quality of the respiratory disease. In the table they make it clear that severe respiratory disease was the same at 56% pre and 40% post and of course all of these babies would have needed admission. What we don’t know is what happened to the mild to moderate group.
A Theory
The whole point of giving PPV for the non-vigorous infant is to establish FRC. In the old approach it is conceivable that some of the infants could have lost volume during attempted intubation. The resultant delay in oxygenation could exacerabate any tendency to pulmonary hypertension. It could also turn a baby from one that could have had mild grunting to one that needed CPAP. Put another way it could have changed the outcome from a baby that needed observation and some prone positioning for a few hours to one that is committed to admission.
What these results show is basically what the intent of doing away with routine suctioning was supposed to do. The vast majority of severe disease in meconium aspiration syndrome is acquired in-utreo. Hypoxia and acidosis contribute to pulmonary hypertension while gasping respirations lead to inhalation of meconium deep into the airways. Suctioning after birth is not really going to help this cohort much. Providing positive pressure ventilation to the more mildly affected infants however may help open their lungs whereas delays in initiating would have the opposite effect.
In the end routine suctioning was a dogma that was in need of a challenge. The authors in the body of the paper go through other similar studies and in all but one the findings are similar. I commend the authors here for their humility as they do add at the end of the report all the potential shortcomings of the research. I for one don’t think it was necessary, as well designed research and thought went into taking down the dogma of routine suctioning. There is complete biological plausability for the findings presented here and I for one am glad to see that research in this case informed practice change that I believe was for the better.
Let me start off by giving thanks to John Minski for this article and in fact for many others that have been reviewed on this blog. John is a registered respiratory therapist in Winnipeg with a passion for respiratory care like no other. John frequently sends articles my way to think about for our unit and this one was quite sensational to me. As readers of this blog I thought you might find it pretty interesting as well.
Why Would A Mask Cause Apnea
To begin with this seems counterintuitive as don’t we use masks when babies are apneic to help them breathe? While this is true and they are great for support, what if a baby is breathing already but has laboured respirations and you choose to apply a mask and provide PEEP to support their breathing efforts. Surprisingly there is evidence that this may induce apnea. The evidence comes from studies in term infants and one such study to demonstrate this finding was Effects of a face mask and pneumotachograph on breathing in sleeping infants by Dolfin T et al. While tidal volumes improved with facemask application, respiratory frequency after mask application dropped by 6 breaths a minute. This may have been offset by a rise in tidal volume as minute ventilation was unchanged. Regardless there was a slowing of the respiratory rate which was found in other studies as well.
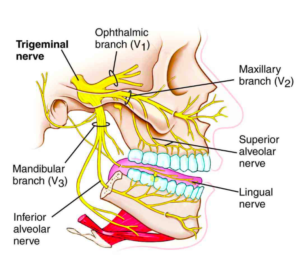
The cause of this slowing has been attributed to the Trigemiocardiac Reflex (TCR). The trigeminal nerve branches all pass through the area around the mouth and nose as shown in this figure.
Applying the mask can cover these nerves and as they become compressed, This can trigger the TCR leading to apnea & reductions in HR and blood pressure (in the case of V1).
What About In Preterm Infants?
Preterm infants are a good group to study this phenomenon in as they as a group are more apt to need respiratory support after birth and have increased tendency towards apena and bradycardia compared to their term counterparts. That is what was done in a retrospective fashion by researchers from the Czech Republic who restarted research that largely occured in the early 1980s on the TCR so congratulations to them for digging this up and deciding to look at this in preterm infants.
The Study
Kypers KL et al published The effect of a face mask for respiratory support on breathing in preterm infants at birth in Resuscitation in late 2019. The study retrospecitively looked at the immediate delivery room outcomes for 429 infants (median (IQR) gestational age of 28+6 (27+1-30+4) weeks and divided them into those born who breathed but needed respiratory support with a mask and those who were apneic at birth.
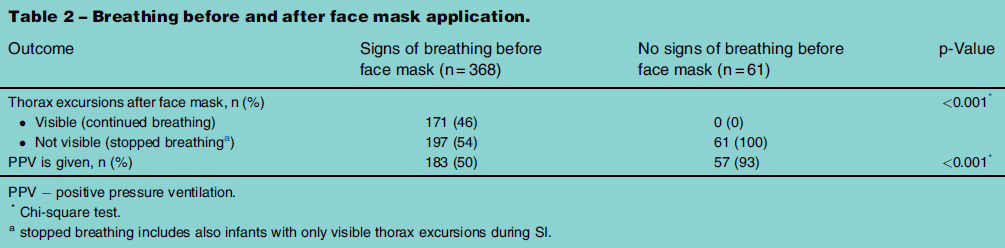
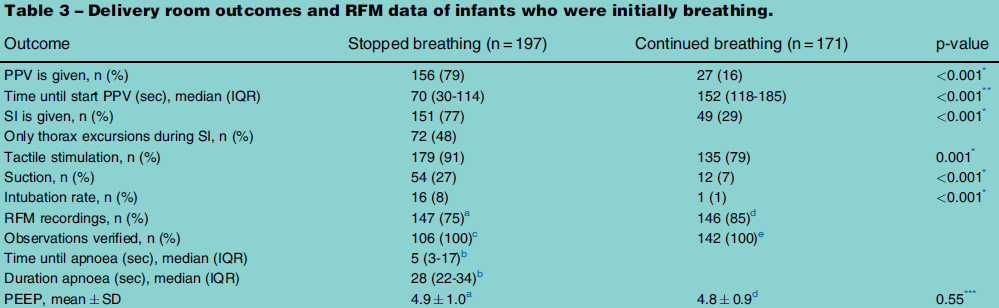
As shown in the above table of the 368 babies who showed signs of breathing but had a facemask applied to provide either PEEP or anticipate the need for PPV about half stopped breathing after facemask application. In the figure below it is worth noting that the median time for this to happen was only 5 seconds and the duration of apnea was almost half a minute with 80% of these babies needing PPV to come out of it. Of those who continued breathing there were marked differences in timing of respiratory support and whether sustained inflations were employed. You were also more likely to intubate the infant if they had stopped breathing.
Lastly, there was an inverse correlation seen between gestational age and likelihood of apnea after facemask application of 1.424 (1.281 – 1.583 95% CI)
What are the implications here?
The TCR appears to happen in preterm infants when you apply a mask to support respiration more commonly than at term and the risk increases as GA decreases. This is not a good combination as it means that those that are at increasing risk of lung injury from positive pressure ventilation may be at higher risk of going apneic soley from placement of a mask over the mouth and nose. Yet this has been a staple of neonatal resuscitation for as long as I and I suspect almost anyone can remember.
What I think this really begs for is a follow-up study on the use of nasal prongs placed in the nares to provide CPAP right after delivery. This approach is what we in our centre strive to do anyway but there are many centres I suspect that still employ the mask and bag to provide CPAP either through a PEEP valve or manually compressing the exit flow end of the anaesthesia bag. If compression of the tissues around the mouth and nose could be averted, could the TCR be avoided as well with the use of prongs in this fashion. If a patient goes apneic after a mask is placed over the mouth and nose and then goes on to require PPV with provision of large tidal volumes to a 26 week infants lungs the damage is likely done and the die cast that this infant will develop enough lung injury to potentially be labelled as having BPD down the road.
I would like to thank the authors again for picking up on research that is over 35 years old and sparking new life into this area of Neonatology!
It’s Father’s Day so why not put out a post about a role for father’s in resuscitation. Given that we are talking about a parent being present for resuscitation after delivery and the mother will have just delivered, what follows is a discussion about having the other parent present at the ensuing resuscitation if needed. This will of course not always be a father as in female same sex parenting so what follows could apply to any situation in which there are two parents present and one has just delivered.
Since I was a resident this question has been batted around. During a resuscitation is it better to have families present or not? Certainly work has been done in this area which has demonstrated that from the families perspective this is a worthwhile pursuit. Families wish to be present and as a parent myself I would say it would be far more frightening to be kept out of the room than invited in to see what is going on. A mind can often conjure up scenarios that are far worse than actually exist if left to ourselves. I think in many centres now this is the case that families are invited into the room when their infant is being resuscitated but looking at things from another standpoint the question becomes what effect this has on the team doing the work? Does the team perceive that their workload is increased and if so could this affect performance?
An Answer to this question?
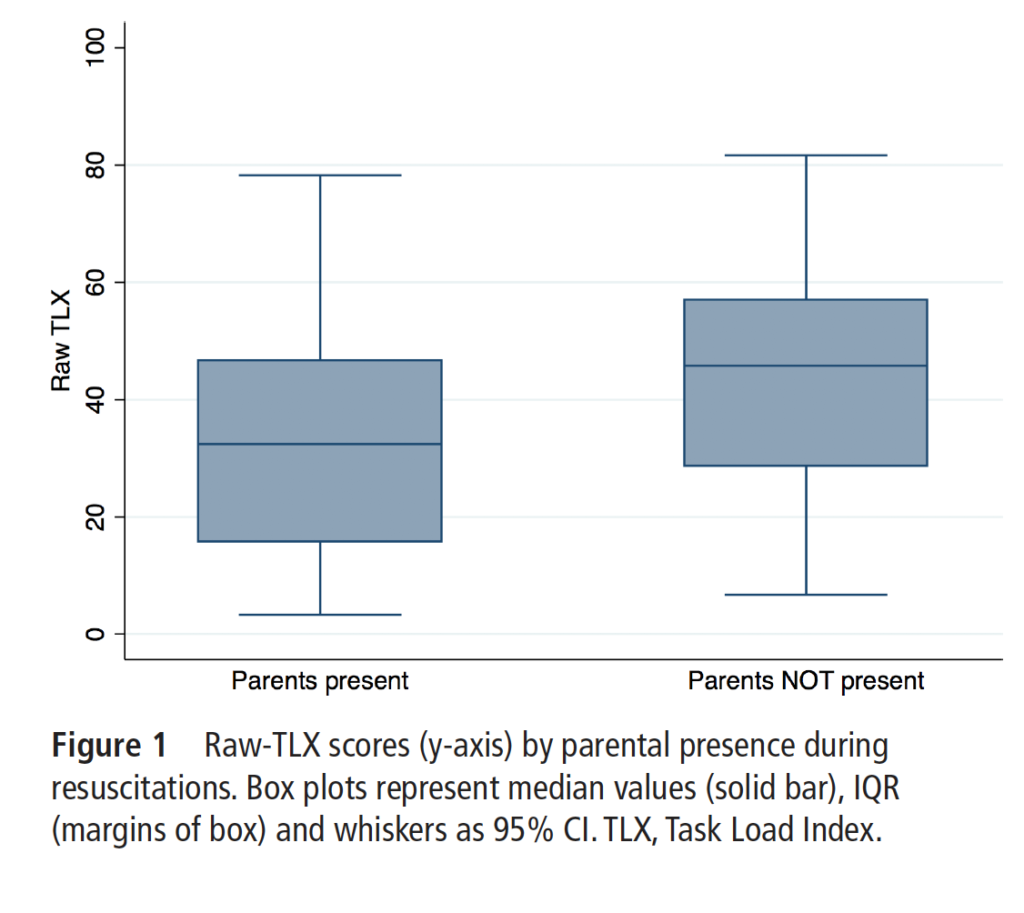
Dr. Schmölzer and his team in Edmonton (my former place of work) have atttempted to answer this question by looking at initial resuscitations in the delivery suite. Their study Does parental presence affect workload during neonatal resuscitation? used a tool I was unfamiliar with called the multidimensional National Aeronautics and Space Administration Task Load Index (TLX) survey to assess workload. After a resuscitation team members were invited to fill out the survey anonymously and in total 204 submissions were done. Degree of intervention after delivery included requiring stimulation 149 (73%) and suction 130 (64%), 120 (59%) continuous positive airway pressure, 105 (52%) positive pressure ventilation, 33 (16%) intubation, 10 (5%) chest compression, and 4 (2%) reported administration of epinephrine during resuscitation.
Results and Thoughts
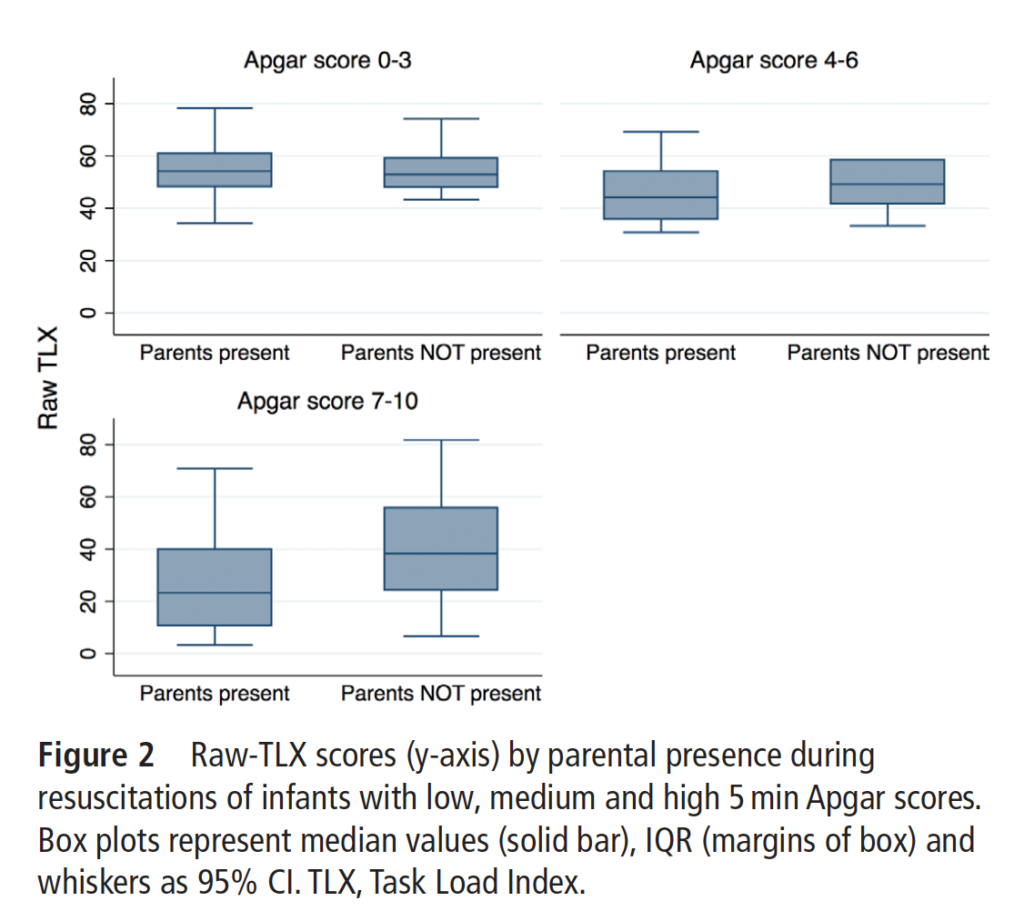
Looking at the raw scores on the TLX the difference was highly significant in favour of having a parent present.
When further subdividing by apgar scores an interesting finding emerges in that as the apgar score increases the workload decreases. Even in the lowest apgar range the workload though appears to be equivalent.
I wonder if the finding results from being able to kill two birds with one stone? Part of the duty for any health care provider performing a resuscitation is to inform the parent of what is happening. When a patient is not doing well a provider might feel distracted and torn between providing the immediate care required and keeping the family abreast of what is happening. Having the family member present to see exactly what is going on reduces the amount of communication using descriptions and having to explain what they mean. Being able to point at an infant on CPAP and having respiratory distress for example is far easier with the parent present to point at the finding of indrawing than taking the time to explain it. I suppose the number of questions might even be lower in that circumstance. If a baby is quite ill at birth though and receiving chest compressions or epinephrine I would imagine it would be difficult to educate the family concurrently so explaining in detail what has been happening might be deferred to a later time point and hence the workload might be no different. What the data does suggest to me though is that in addition to previous research demonstrating benefits of families being part of the resuscitation for themselves, the team is no worse off in terms of workload and might even benefit from having them there as well.
The next logical study will look at resuscitations on the unit rather than in the case room but I think the question that was talked about as a resident can be put to rest.
If you have been following this blog for awhile you may recall a post from a couple years back on Physiological based cord clamping. The premise of that paper was that rather than arbitrarily choosing a time to clamp the cord, one should look for the following three features that indicate adequate pulmonary blood flow has been established:
1. Establishment of adequate breathing(average tidal volume > 4 ml/kg) on CPAP – using a mask capable of measuring expired volumes
2. HR above 100 BPM
3. SpO2 above the 25th percentile using an FiO2 <0.4
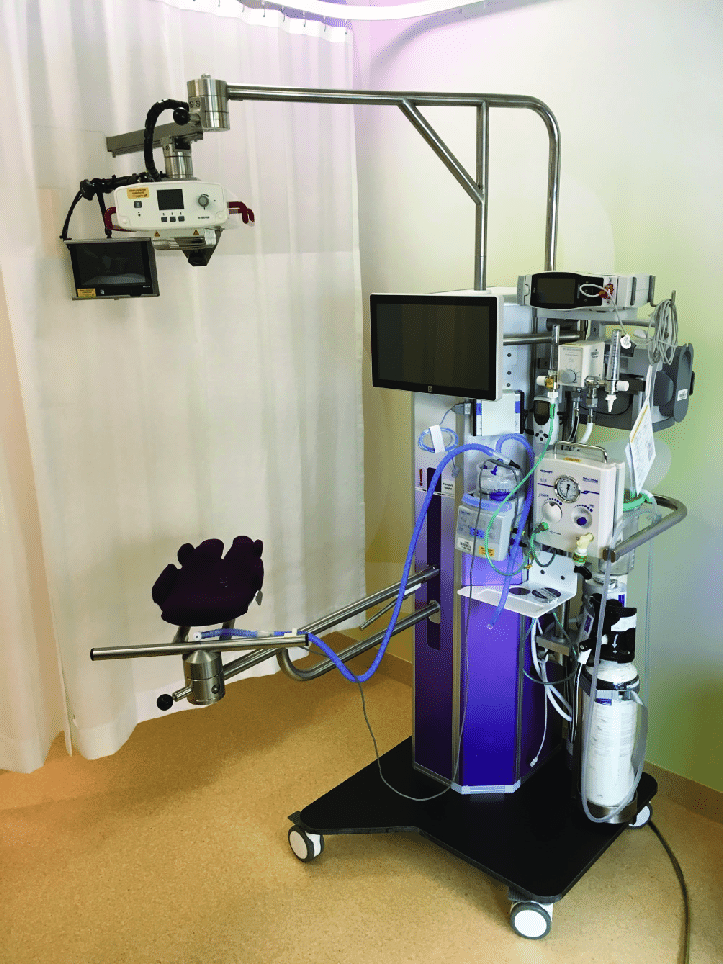
In the original trial it was a proof of concept design that sought to determine if resuscitation on their “Concord” table was feasible and how long would it take for the above criteria to be met so the cord could be clamped.
The mean time for cord clamping in that trial was 4 minutes and 23 seconds. This is much longer than the typical delayed clamping of 30 -60 seconds and even longer than the few studies that have looked at delays of 1- 3 minutes.
The Next Phase
The same group now sought to compare DCC of 30 – 60 seconds with the PBCC approach for infants <32 weeks gestational age in the paper Physiological-based cord clamping in very preterm infants – Randomised controlled trial on effectiveness of stabilisation. This trial was set up as a non-inferiority trial to see if the pre-defined difference in time to stability of 75 seconds would be crossed. A power calculation was performed that indicated the authors would need to recruit 64 infants with 32 in each arm. Due to poor recruitment the authors chose to stop the trial early with only 17 infants in the DCC group and 22 infants in the PBCC arm. An analysis with those patients identified that the non-inferiority limit had been met already.
Difference in resuscitation
Infants randomised to the DCC group had their cords clamped at 30-60 seconds and had their resuscitation started on a resuscitation table. Infants in the PBCC arm were placed on the Concord after delivery and had their resuscitation performed there. Care afterwards would have been similar.
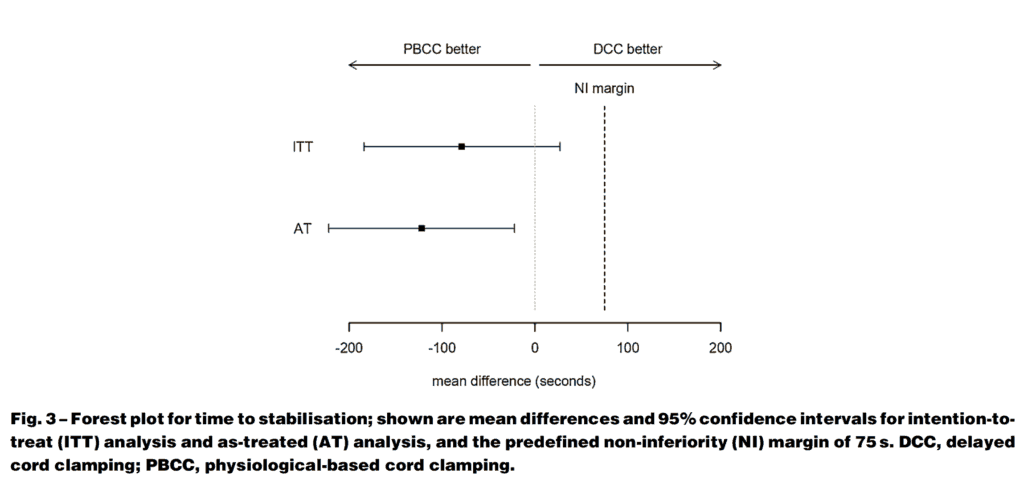
They found that the mean time to stabilisation was 5:54 +/- 2:27 in the PBCC group and 7:07 +/-2:54 in the DCC groups. The mean difference was 1:19 min (95% CI -3:04 to 0:27 min). The results clearly demonstrated a finding of shorter time to stabilisation in the PBCC arm as shown in the figure.
As the confidence interval crossed 0 though in the intention to treat analysis we can say that PBCC is no worse than DCC but can’t say it is superior as a strategy overall. Perhaps larger numbers may have shown something different but at least we know it isn’t worse.
Other Findings
One thing that I would imagine Obstetricians would be concerned with here is the potential for significant blood loss since uterotonics were not provided until the cord was clamped which in PBCC was quite a bit longer, Opposite to what one would have expected the mean blood loss in the DCC group was 450 mL compared to 300 mL in the PBCC arm. Not different statistically though given the small numbers.
There were almost twice the number of females in the PBCC group which could account for some of the findings here. Another difference worth noting was that respiratory support was initiated earlier on the concord than on the standard resuscitation table which the authors acknowledge may be due to familiarity with doing so from experience with the specialized set up. Earlier ventilation (1:11 min vs 2 min in the DCC) could indeed lead to earlier reaching of the end points of the stabilisation criteria.
Regardless of the last couple points, what is needed now is a much larger study to look at clinical outcomes. The numbers were so small here to really examine such clinical points but this is where I believe we are now headed. If the pattern continues I guess we will see another study coming from this group in a couple years so stay tuned!