

It’s Father’s Day so why not put out a post about a role for father’s in resuscitation. Given that we are talking about a parent being present for resuscitation after delivery and the mother will have just delivered, what follows is a discussion about having the other parent present at the ensuing resuscitation if needed. This will of course not always be a father as in female same sex parenting so what follows could apply to any situation in which there are two parents present and one has just delivered.
Since I was a resident this question has been batted around. During a resuscitation is it better to have families present or not? Certainly work has been done in this area which has demonstrated that from the families perspective this is a worthwhile pursuit. Families wish to be present and as a parent myself I would say it would be far more frightening to be kept out of the room than invited in to see what is going on. A mind can often conjure up scenarios that are far worse than actually exist if left to ourselves. I think in many centres now this is the case that families are invited into the room when their infant is being resuscitated but looking at things from another standpoint the question becomes what effect this has on the team doing the work? Does the team perceive that their workload is increased and if so could this affect performance?
An Answer to this question?
Dr. Schmölzer and his team in Edmonton (my former place of work) have atttempted to answer this question by looking at initial resuscitations in the delivery suite. Their study Does parental presence affect workload during neonatal resuscitation? used a tool I was unfamiliar with called the multidimensional National Aeronautics and Space Administration Task Load Index (TLX) survey to assess workload. After a resuscitation team members were invited to fill out the survey anonymously and in total 204 submissions were done. Degree of intervention after delivery included requiring stimulation 149 (73%) and suction 130 (64%), 120 (59%) continuous positive airway pressure, 105 (52%) positive pressure ventilation, 33 (16%) intubation, 10 (5%) chest compression, and 4 (2%) reported administration of epinephrine during resuscitation.
Results and Thoughts
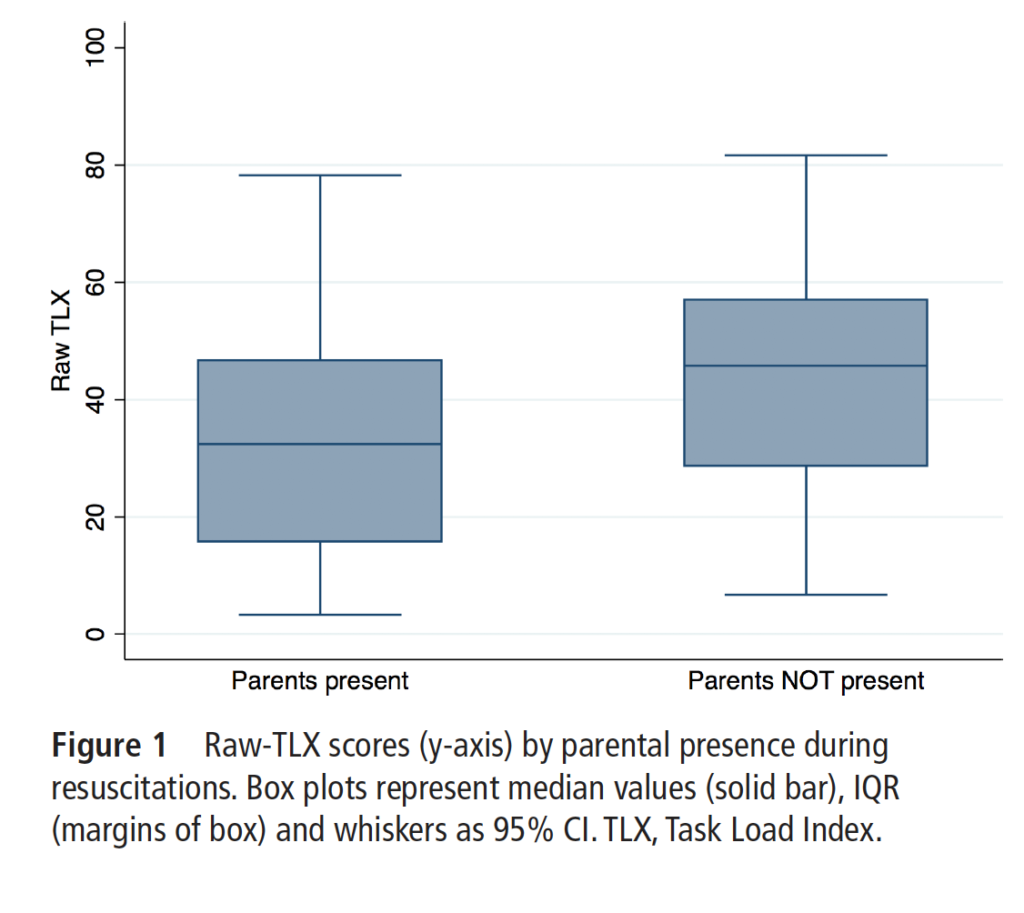
Looking at the raw scores on the TLX the difference was highly significant in favour of having a parent present.
When further subdividing by apgar scores an interesting finding emerges in that as the apgar score increases the workload decreases. Even in the lowest apgar range the workload though appears to be equivalent.
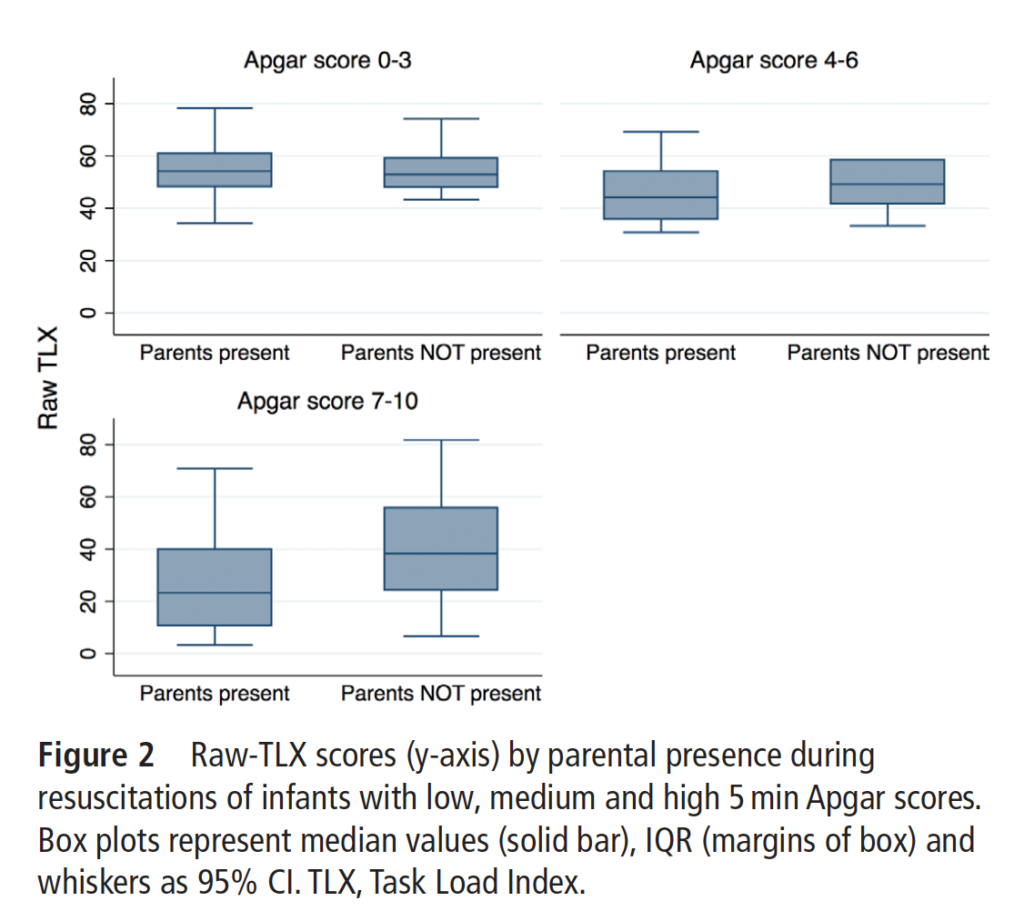
I wonder if the finding results from being able to kill two birds with one stone? Part of the duty for any health care provider performing a resuscitation is to inform the parent of what is happening. When a patient is not doing well a provider might feel distracted and torn between providing the immediate care required and keeping the family abreast of what is happening. Having the family member present to see exactly what is going on reduces the amount of communication using descriptions and having to explain what they mean. Being able to point at an infant on CPAP and having respiratory distress for example is far easier with the parent present to point at the finding of indrawing than taking the time to explain it. I suppose the number of questions might even be lower in that circumstance. If a baby is quite ill at birth though and receiving chest compressions or epinephrine I would imagine it would be difficult to educate the family concurrently so explaining in detail what has been happening might be deferred to a later time point and hence the workload might be no different. What the data does suggest to me though is that in addition to previous research demonstrating benefits of families being part of the resuscitation for themselves, the team is no worse off in terms of workload and might even benefit from having them there as well.
The next logical study will look at resuscitations on the unit rather than in the case room but I think the question that was talked about as a resident can be put to rest.