As awful as COVID19 has been over the last year and a half one thing has continued to perplex myself and others. Why do babies whethe term or preterm so rarely acquire the virus? Numerous studies have been able to document placental changes and infection of these tissues. On rare occasions reports have come out with evidence of neonatal infection but fortunately most are mild.
These findings have in large part contributed to the Canadian Pediatric Society practice points on three topics.
In this post an argument was made that the reason these infants are resistant is due to low levels of ACE-2 receptors in the nasal mucosa of children. In this study children as young as 4 years of age were found to have very low levels of this receptor (portal of entry for SARS-CoV-2) into the host. I speculated at the time that if one carried forward the findings to younger children and infants you might find there were hardly any receptors at all.
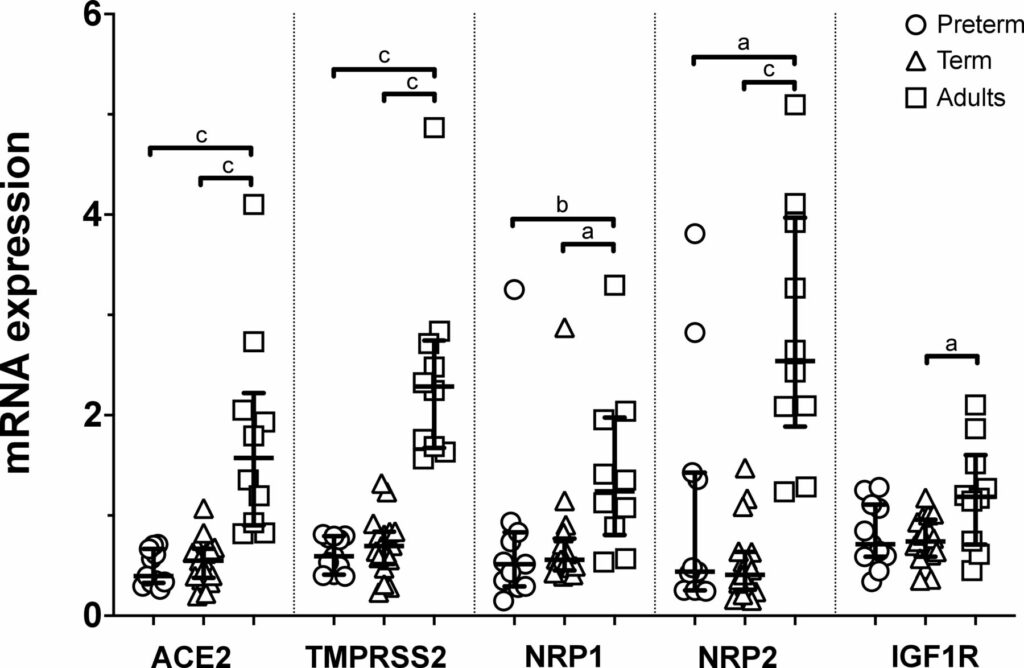
Well, someone finally did the study and confirmed what I suspected. The study report is entitled Nasal expression of SARS-CoV-2 entry receptors in newborns by Heinonen S et al. It’s not a big study but the results are consistent across 28 newborns (17 term and 11 preterm) and 10 adults. In each newborn whether term or preterm a nasal mucosal scraping was performed at 24 hours of age and used to measure by reverse-transcription quantitative PCR mRNA expression of ACE2, transmembrane serine protease 2 (TMPRSS2), neuropilin 1 (NRP1) and neuropilin 2 (NRP2) and insulin-like growth factor 1 receptor (IGF1R).
What the results show you is that babies are not just small adults. They are different yet preterm do not seem to be that different than term infants in terms of receptors. While ACE2 has garnered most of the attention when it comes to receptors for SARS-CoV-2 the others also play a role and are in general expressed to a lesser degree in neonates than adults.
Conclusions
In the previous post I argued what was in your nose makes a difference to your risk of contracting SARS-CoV-2. Really the point is what is not in your nose. Thankfully neonates do not have good expression of these receptors and that may be the biggest reason for the general protection they have from this pandemic. It has certainly a good time to be in the “have not” group!
Testing for COVID19 has become so much the norm in society that in casual conversation you might ask someone if they have been tested. Chances are you know someone who has and even more likely that it is many people at this point. If you have been following this blog for awhile you would know that one of the issues with testing is that it is extremely sensitive. The RT-PCR test can pick up even trace viral particles whether alive or dead and therefore a test in and of itself tells you one thing. There is virus present but whether it is alive or dead is another matter. Virus can be shed for weeks after symptoms develop so what information can we obtain that might tell us whether the patient is at risk of infecting another person. Moreover, when can we relax precautions around the patient themselves and no longer worry that they are a risk to others?
Winnipeg Researchers May Have the Answer
Given that I know many of the authors of the paper personally that I will discuss and the quality of the work they do I am delighted to cover this important work. The paper Predicting Infectious Severe Acute Respiratory Syndrome Coronavirus 2 From Diagnostic Samples by Bullard J et al tackles the question above using cycle times and times to positivity after initial symptoms. First off it is important to understand the concept of cycle time. When you use RT-PCR to amplify pieces of RNA there are 40 cycles of amplification that a sample is put through. The lower the number of cycles required to detect the RNA the more viral material was present to begin with. As the cycle times get well into the 30s the possibility of there being just trace amounts of virus exists or that the patient themselves had no virus present but the sample was contaminated with a very small quantity of virus. The time to positivity is the amount of hours/ days it takes after initial symptoms develop until an RT-PCR test becomes positive.
The authors analyzed 90 samples either from naso-pharyngeal swab or ETT secretions with a median age of 45 years (I know not neonatal). Collected samples included from day 0 to day 21 after symptom onset. What the authors did that was interesting in this paper was that in addition to the samples being tested by RT-PCR, for each positive sample they went through the laborious task of performing tissue culture to attempt to grow the virus. By doing so the authors were then able to compare the time to positivity (STT) and Ct thesholds to determine if there were numbers for each that could be used to predict which samples would have live virus that could be grown,
The Results Please
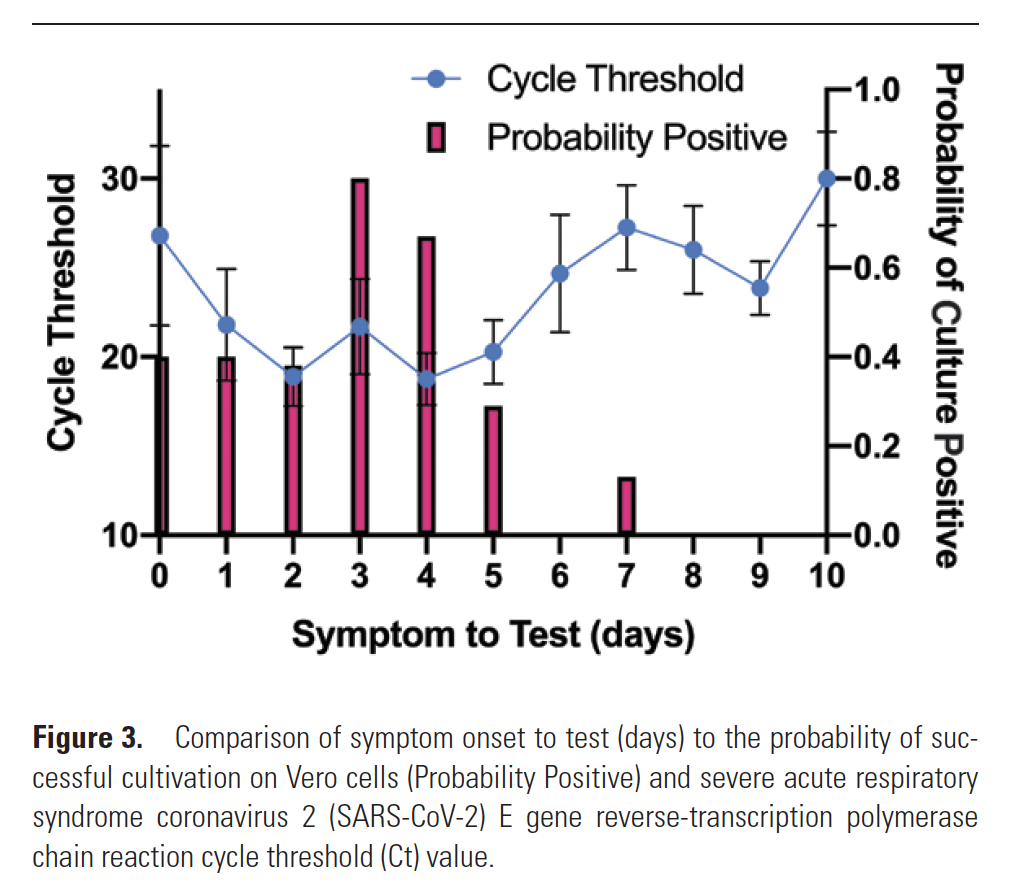
The two main findings in the paper were that no patient after day 8 from symptom onset with a positive RT-PCR could actually have live virus grown in tissue culture. This is shown in Figure 3 from the paper
Secondly, no patient with a cycle time greater than 24 could also have live virus grown. In fact for every 1 unit increase of Ct the odds ratio for infectivity decreased by 32%.
The size of the study is fairly large when it comes to COVID19 studies like this but as the authors say the results are for adults and given how few children have been infected especially in our location in Canada we should be hesitant to generalize to children and in particular neonates.
What the study does give us
This study I felt was worth sharing with you for the reassurance that I think it may give especially if it leads to further validation by even larger studies including children and those who are immunocompromised who may have prolonged shedding. What it suggests though is that the next time you encounter a patient who you are told tests positive there are a couple important questions to ask from your lab. The first is how many days from the start of symptoms was the RT-PCR done? Secondly, ask them for the Ct value. As per the authors
“Receiver operating characteristic curves constructed using Ct vs positive culture showed an area of 0.91 (95% CI, .85–.97; P < .001) with 97% specificity obtained at a Ct of > 24. Similarly, STT vs positive culture showed an area of 0.81 (95% CI .73–.90; P < .001), with 96% specificity at > 8 days”
In other words, if the answers to those questions are >8 days and a value for Ct >24 you should be able to leave the patient with reasonable expectation that they are either no longer infectious or at worst almost clear of live virus.
Interesting work that I hope will be helpful to someone out there!
Regardless of where you live, you may have noticed that this year’s flu and RSV season has not been as bad as in previous years. I recall early in the pandemic hearing that Australia had virtually no flu season at all this year. The question therefore is where did these viruses go? Many people have attributed the drop is other viral illnesses to the fact that we are wearing masks and washing our hands a lot more. This no doubt has something to do with it but the reality is that many have chosen not to wear masks and additionally we know that others have failed to use PPE appropriately. Let’s face it, COVID has spread far and wide and yet the other viruses have not. So where did they go?
Viral Interference
This is a subject I had never heard of or really considered as an entity until I began looking at COVID19 as part of a talk I gave this year. The concept has been known since the 1930s or even earlier. The first reference I found for this was by Findlay GM An interference phenomenon in relation to yellow fever and other viruses from 1937 (sorry no link to the paper) and then Lennette EH, Koprowski H. INTERFERENCE BETWEEN VIRUSES IN TISSUE CULTURE. J Exp Med. 1946 Feb 28;83(3):195-219. In this latter study innoculation of yellow fever virus and the West Nile virus produced either partial or complete suppression of growth of the Venezuelan equine encephalomyelitis virus. In other words, the idea here is that once one virus takes hold of a cell it becomes quite difficult (but not impossible) for another virus to also grow at the same time. Looking at how SARS-CoV-2 and RSV might interact is interesting as in tissue culture RSV is the slower replicating virus. SARS-CoV-2 seems to grow in cell culture in the order of 3-5 days while RSV tends to be longer at 5-14 days. In vivo of course things can be different as the host can influence rapidity of growth but the if SARS-CoV-2 is spreading rapidly through the community it could be that by infecting the host first and being the faster growing virus it effectively and strangely protects the host against other viruses such as RSV. If there is anything about this pandemic that maybe we can take some comfort it it is maybe that!
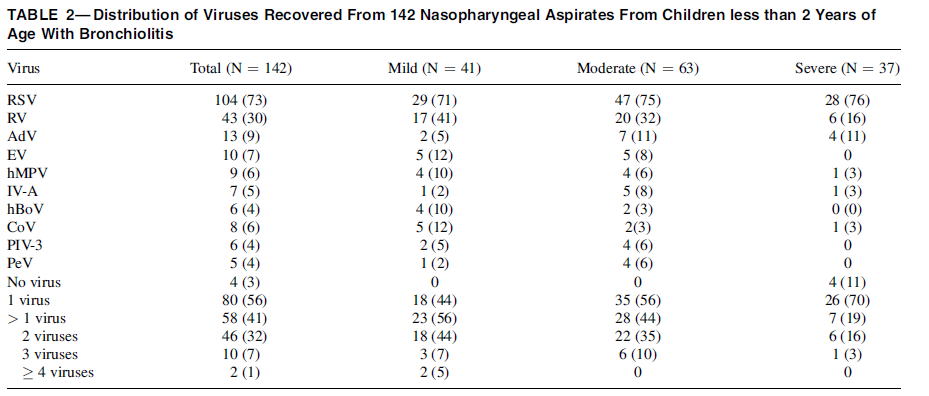
What about disease severtiy when two viruses take hold?
You would think if you were unlucky enough to get RSV and COVID19 at the same time your symptoms would be worse than getting RSV alone but the evidence suggests otherwise. Having two viruses competing for the same host may lessen the severity of the disease. This was demonstrated by Kim Brand H et al in Infection with multiple viruses is not associated with increased disease severity in children with bronchiolitis Pediatr Pulmonol 2012 Apr;47(4):393-400, In this study the authors examined 142 nasal aspirates of children with bronchiolitis and grouped them into categories of mild, moderate and severe disease. What they found suggests that two or more viruses infecting the same host may reduce the severity of the illness usually ascribed to the virus compared to when it affects the host alone. In the case of RSV from Table 2 above, with severe bronciolitis, RSV was found 76% of the time. Bronchiolitis may be caused by other viruses of course and towards the bottom of the table when severe disease was present one virus was found 70% of the time. Howeve as the number of viruses in the host increased the likelihood of severe diease dropped while mild diease increased.
What to expect then?
I am just a Neonatologist but based on the above research I am expecting a couple things this winter season. I predict we will continue to see lower rates of RSV infection and perhaps influenza as the domination of SARS-CoV-2 continues. The other thing that will be interestin to look at retrospectively will be what the distribution of disease spectrum for RSV is this season as if the above is correct we should see less severe disease when looking at emergency visits and hospitalizations. Will be an interesting story for 2021 and I suspect much will be written about the impacts of COVID19 on many fronts. Look forward to no longer talkign about that virus at some point later in 2021 when we all start saying “remember when…”
I recently had the honour of being asked to present grand rounds at the University of Manitoba. My former Department Head during the question period stumped me when he asked me what role angiotensin converting enzyme 2 receptor (ACE2) has in pediatric COVID19. Like all great teachers, after I floundered and had to confess that while I was aware there is a role in COVID19 I wasn’t sure of the answer, he sent me a paper on the subject. The reality is that a very small percentage of COVID19 illness is found in children. Some estimates have it at 2%. Why might that be?
It’s what’s in the nose that matters
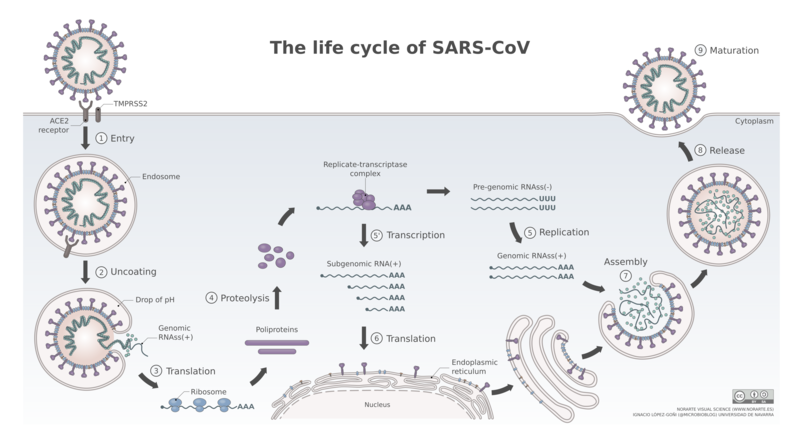
What has been known for some time know is that the point of entry for SARS-CoV-2 is the nasal epithelium. What is also known is that the receptor that the virus binds to in order to gain access to the host. Such binding and what happens after the virus gains entry to the body is shown in this figure depicting the life cycle of SARS-CoV-2.
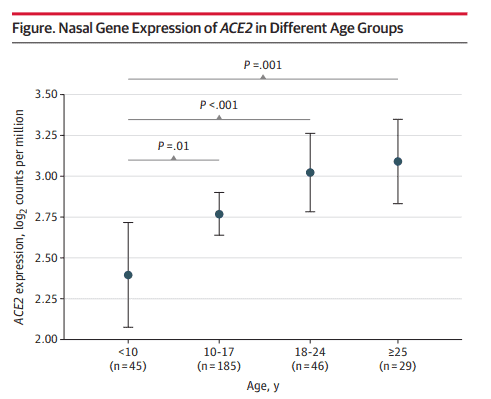
In a research letter by Bunyavanich et al Nasal Gene Expression of Angiotensin-Converting Enzyme 2 in Children and Adults looked at 305 patients from ages 4-60 years to examine biomarkers of asthma. In the course of looking at the nasal epithelium of these patients, they found age related differences in the expression of ACE2 receptors as shown in the following figure.
I think the results somewhat speak for themselves. The younger you are the less receptors you have. If you have less receptors maybe you are less likely to contract the virus!
What we don’t know
This research leads to some interesting questions. Drugs such as losartan and valsartan already exist and function by blocking he ACE2 receptor. Could blockade help to limit the spread of infection? I am not aware of any such trials going on at the moment but something worth looking at.
The other point that needs to be raised is that the most vulnerable group of ages >60 were not looked at in this study. The trend would certainly indicate that with age we would expect the receptor numbers to increase but since we don’t actually have the data in the older groups we don’t know if receptor numbers start to fall again with age. Similarly we don’t know below the age of 4 what receptor numbers are like. In examining risk of vertical transmission it is worth noting that the recent placental positive RT-PCRs as in Detection of SARS-COV-2 in Placental and Fetal Membrane Samples. In that study while 3 of 11 placental membranes tested positive, none of the newborns were infected. Could it be the fetus and newborn is protected by having very little density of ACE2 receptors? Something to look at and will be no doubt.
Regardless, in the fight against COVID19 maybe one direction for therapeutic targeting should be addressing this receptor and seeing if there is something we can’t do to make it less susceptible to binding.
For more Neonatal subjects be sure to see my Facebook page at https://www.facebook.com/allthingsneonatal2
After several reports providing reassurance to breastfeeding mothers, two very recent reports are giving me reason to pause. The Canadian Pediatric Society has been recommending breastfeeding if a mother has COVID19 with precautions in place; Breastfeeding when mothers have suspected or proven COVID-19. It would be heresy to suggest that a mother not be permitted to breastfeed her infant but what follows are two reports that at the very least may need to enter the discussion when a COVID19 positive mother gives birth and is deciding about route of feeding.
Toronto Case Report
The first report was notable not so much for breastmilk but rather that a mother with a chronic immunodeficiency and pneumonia from COVID19 had placental surfaces that tested positive on PCR for COVID19. This was the main focus of the paper Probable congenital SARS-CoV-2 infection in a neonate born to a woman with active SARS-CoV-2 infection. In the same paper though, testing of breastmilk in this mother demonstrated a positive PCR with a semi-quantitative cycle time result (there are 40 cycles of amplification of RNA in PCR testing- the further away from 40 cycles the more likely it is a true positive).
The results above were positive at 2 days and negative at 7 days. One could possibly excuse this case as an anomaly since the mother in this case not only was sick but also has chronic neutropenia but then along comes another report.
Second Research Report
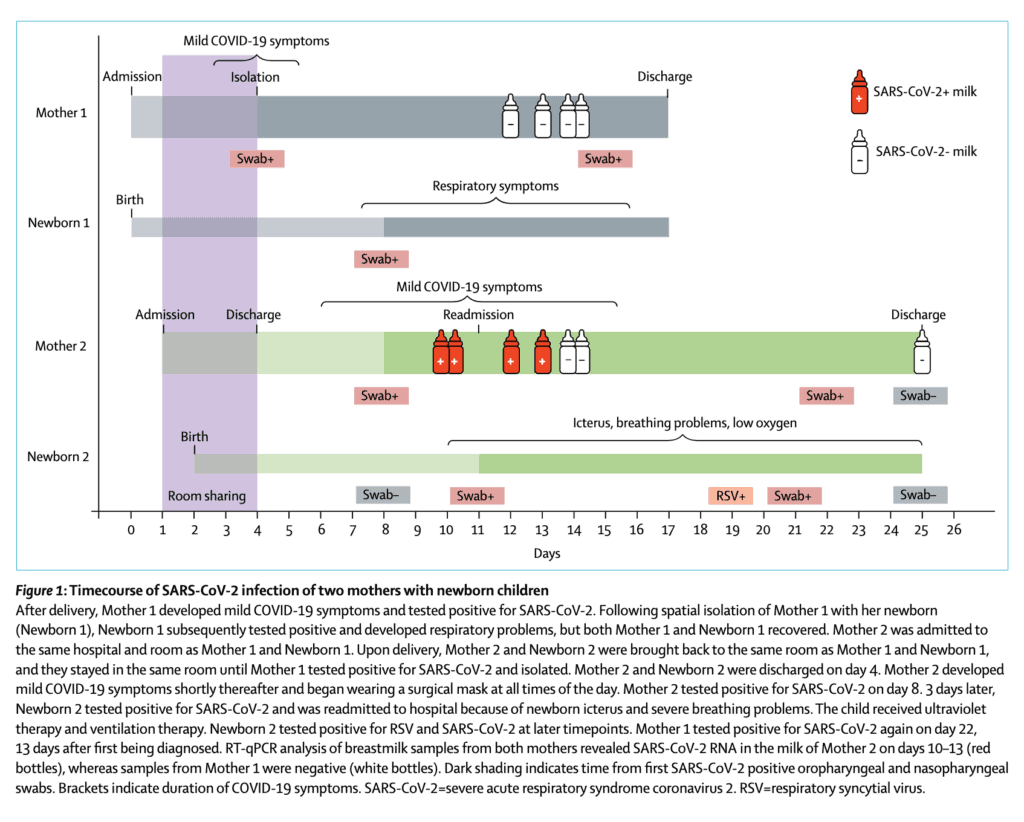
This week a second report emerged that adds to the uncertainty around breastmilk. Detection of SARS-CoV-2 in human breastmilk looks at two mothers one of whom was negative on testing of breastmilk but the other unfortunately tested positive. The authors included the following timeline which is very informative.
From the timeline above you will note that in the second case the mother becomes positive at 11 days of age and the infant tests positive around the same time the milk comes back positive. The infant in this case also develops RSV which likely explains the symptoms they developed later in the course. What is concerning to me though is that in this case while the mother was COVID19 positive, she was not acutely ill. When thinking of vertical transmission this has been something that has been postulated in suspecting that those with more severe illness have higher viral loads and therefore may be capable of vertical transmission. Not the case here if the results are to be believed. Adding to the strength of the result are Ct values for SARSCoV2 N peaked at 29∙8 and 30∙4 in whole milk and skimmed milk respectively so this seems real.
How does this differ than past testing?
What intrigues me about this study in particular is that past research on transmission into breastmilk has failed to detect the virus. It could be that previous testing close to delivery was negative and that with time might the virus enter breastmilk? At eleven days I think this may be the latest testing done. In virtually all cases reported about COVID19 positives in newborns the authors have always explained the painstaking steps they took to prevent postnatal infection. I do wonder now if some of these cases may be related to a small percentage of women carrying the virus in their breastmilk. This leaves us in a tough spot. What do we tell women who are thinking of breastfeeding and have COVID19? There will need to be discussion on this but one option is to proceed with feeding accepting there may be a small risk of transmission. A second option would be to test milk but if the transmission occurs late you may miss it in hospital on initial sampling Finally it may be worth pumping and discarding milk until mothers test negative and using donor breastmilk in the meantime (or formula for those who don’t have DBM).
Regardless I think this information coming out will need to be digested and centres think about how they will approach this issue. My guess is these will not be the last reports on this.