

I recently had the honour of being asked to present grand rounds at the University of Manitoba. My former Department Head during the question period stumped me when he asked me what role angiotensin converting enzyme 2 receptor (ACE2) has in pediatric COVID19. Like all great teachers, after I floundered and had to confess that while I was aware there is a role in COVID19 I wasn’t sure of the answer, he sent me a paper on the subject. The reality is that a very small percentage of COVID19 illness is found in children. Some estimates have it at 2%. Why might that be?
It’s what’s in the nose that matters
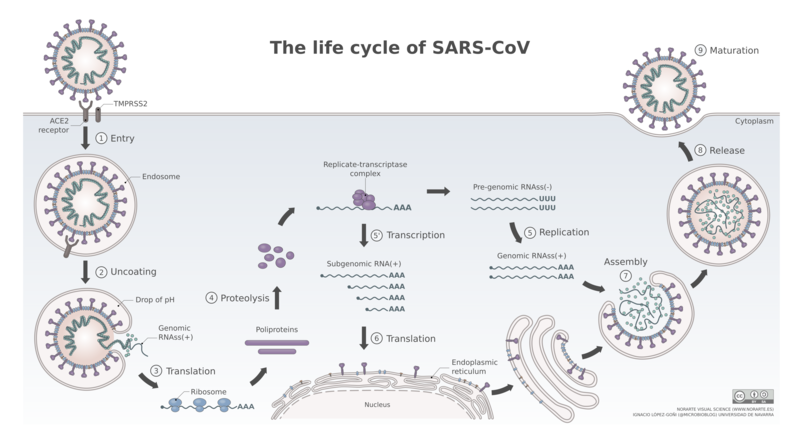
What has been known for some time know is that the point of entry for SARS-CoV-2 is the nasal epithelium. What is also known is that the receptor that the virus binds to in order to gain access to the host. Such binding and what happens after the virus gains entry to the body is shown in this figure depicting the life cycle of SARS-CoV-2.
In a research letter by Bunyavanich et al Nasal Gene Expression of Angiotensin-Converting Enzyme 2 in Children and Adults looked at 305 patients from ages 4-60 years to examine biomarkers of asthma. In the course of looking at the nasal epithelium of these patients, they found age related differences in the expression of ACE2 receptors as shown in the following figure.
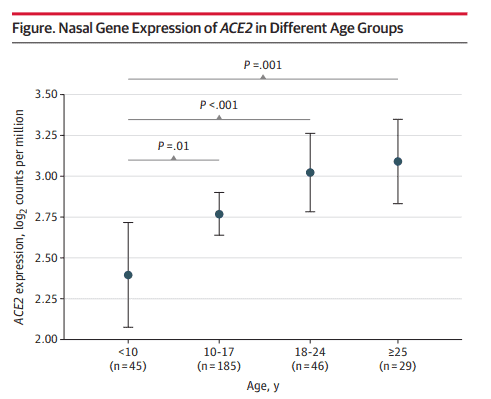
I think the results somewhat speak for themselves. The younger you are the less receptors you have. If you have less receptors maybe you are less likely to contract the virus!
What we don’t know
This research leads to some interesting questions. Drugs such as losartan and valsartan already exist and function by blocking he ACE2 receptor. Could blockade help to limit the spread of infection? I am not aware of any such trials going on at the moment but something worth looking at.
The other point that needs to be raised is that the most vulnerable group of ages >60 were not looked at in this study. The trend would certainly indicate that with age we would expect the receptor numbers to increase but since we don’t actually have the data in the older groups we don’t know if receptor numbers start to fall again with age. Similarly we don’t know below the age of 4 what receptor numbers are like. In examining risk of vertical transmission it is worth noting that the recent placental positive RT-PCRs as in Detection of SARS-COV-2 in Placental and Fetal Membrane Samples. In that study while 3 of 11 placental membranes tested positive, none of the newborns were infected. Could it be the fetus and newborn is protected by having very little density of ACE2 receptors? Something to look at and will be no doubt.
Regardless, in the fight against COVID19 maybe one direction for therapeutic targeting should be addressing this receptor and seeing if there is something we can’t do to make it less susceptible to binding.
For more Neonatal subjects be sure to see my Facebook page at https://www.facebook.com/allthingsneonatal2