Anyone who works in the NICU is more than familiar with the sad moment when you find out an infant has suffered a severe IVH (either grade III or IV) and the disclosure to the family. The family is in a state of shock with the fear of ventricular drainage a reality that will likely come to pass. We have spent many years trying to find ways to reduce this risk and antenatal steroids and delayed cord clamping are two relatively recent interventions that have had a real impact. Unfortunately we have not been able to eliminate this problem though. What if something as simple as an exclusive human milk diet could be that magic bullet to further reduce this problem in our NICUs?
Exclusive human milk diets
I have written about this topic before but as a refresher this generally refers to all sources of nutrition being derived from human milk. Ideally we would provide mothers own milk (MOM) but when this is not available units rely on pasteurized donor human milk (PDHM) as the base feed. Added to this is human derived human milk fortifier (H2HMF) as opposed to bovine powdered or liquid fortifier usually to provide a base caloric density of 24 cal/oz.
Reducing IVH Through Exclusive Human Milk Diets
It would be nice to have a prospective multicentre trial with this as the outcome but there is a significant problem when doing this type of study. The H2HMF is costly with a price tag of about $13-15000 per treatment course so to do a prospective RCT would not be easy for units that don’t use the product already. Moreover, for those units that are already sold on the product it would seem unethical if there was no equipoise to randomize to bovine or human fortifier. As such, when we talk about getting the best evidence it is most likely going to come in the form of a retrospective study as has been done here by Carome K et al in their paper Exclusive human milk diet reduces incidence of severe intraventricular hemorrhage in extremely low birth weight infants.
The authors in this study chose to look at three different time periods with different approaches to feeding of ELBW infants. They were as follows with all diets providing H2HMF going until 34 weeks. Aside from the source of nutrition, starting of and incremental advancement of feedings was protocolized as per unit approach.
2012 to 2014 – MOM was given when available. Preterm formula was the alternative as a supplement Fortification of was with bovine milk-derived liquid fortifier 2014 to 2015 – H2HMF used in those infants receiving exclusively MOM. All others received preterm formula as supplement or alternative. If MOM was available but in insufficient quantities for sole diet, it was fortified with bovine-HMF 2015 to 2017 – all ELBW infants received an EHM diet consisting of MOM if available and PDHM as a supplement to MOM or as full diet, each fortified with H2HMF
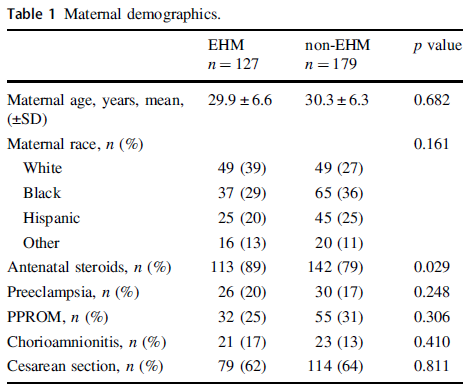
The maternal demographics were similar between those receiving exclusive human milk diets and those without except for a higher antenatal steroid provision in the EHM group. This of course bears consideration in the results as steroids have been shown to reduce IVH.
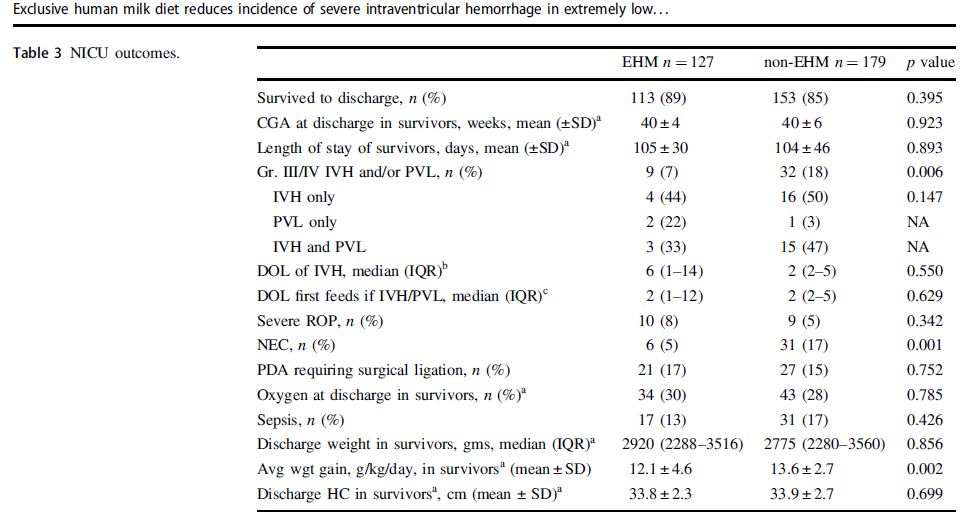
Looking at the results below shows some very promising findings. The incidence of Grade III/IV IVH and/or PVL was 7% in the EHM group and 18% in the non-EHM group. Also noted to be quite different was the incidence of NEC which was 5% in the EHM and 17% in the non group. The authors also did a subgroup analysis looking at the use of MOM vs PDHM and found no difference in outcomes regardless of source of human milk used. As the authors point out this might mean that the pasteurization process does not denature the components of milk responsible for these protective effects if the results are to be believed.
One strength of the study was that the authors performed a logistic regression to control for the higher rate of antenatal steroid use and lower rates of NEC in the EHM group since both would be expected to influence rates of IVH/PVL and found that the results remained significant after this analysis. The findings were an OR of 2.7 CI 1.2–6.0, p = 0.012 so that is promising!
What They Weren’t Able to Do
It’s possible I missed it in the article but like several other papers on this topic the babies who received formula and those who received human milk with bovine fortifier were grouped together. As such what we don’t know from this study is whether the addition of just the bovine fortifier vs H2HMF would have yielded the same results.
Nonetheless what the article does suggest is that use of EHM diets are protective against severe IVH/PVL regardless of the source of human milk when you compare it to receipt of any bovine sources. The caveats about retrospective studies of course exist as per usual but if this is the best evidence we have how do we use it? At the very least this calls out for strategies to maximize milk production for mothers and to use PDHM when MOM is not available. It certainly is suggestive that the use of H2HMF may confer benefit as well. What you unit does with this information I suppose will need to be determined based on the totality of the evidence. I suspect there is more of this story to be told and this adds yet another chapter in the tale of EHM.
Recently the practice of keeping ELBW infants with a midline head position for the first three days of life has been recommended to reduce IVH as part of a bundle in many units. The evidence that this helps to reduce IVH has been somewhat circumstantial thus far. Studies finding that decreased sagittal sinus blood flow, increased cerebral blood volume with increased intracranial pressure all occur after head turns would theoretically increase the risk of IVH. Raising the head of the bed would help in theory with drainage of the venous blood from the head and in fact systemic oxygenation has been shown to improve with such positioning. This presumably is related to increased cardiac output from better systemic venous return.
Bringing it to the bedside
Interestingly, some of the above studies are from over thirty years ago. We now have some evidence to look at involving this practice. Kochan M et al published Elevated midline head positioning of extremely low birth weight infants: effects on cardiopulmonary function and the incidence of
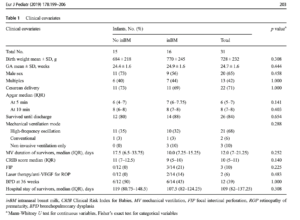
periventricular-intraventricular. The study involved maintaining ELBW infants in an elevated midline head position (ELEV- supine, head of bed elevated 30 degrees, head kept in midline) versus standard head positioning (FLAT–flat supine, head turned 180 degrees every 4 h) during the first 4 days of life to see if this would decrease in the incidence of IVH. Ninety infants were randomized into both arms of the study. In terms of baseline characteristics, BW of 725g in the FLAT vs 739 in ELEV were comparable as well as GA both at 25 weeks. Two differences on the maternal side existed of 40% ELEV vs 24.4% FLAT of mothers having preeclampsia and 23.3% FLAT vs 10% ELEV having prolonged rupture of membranes both of which were statistically significant.
What did they find?
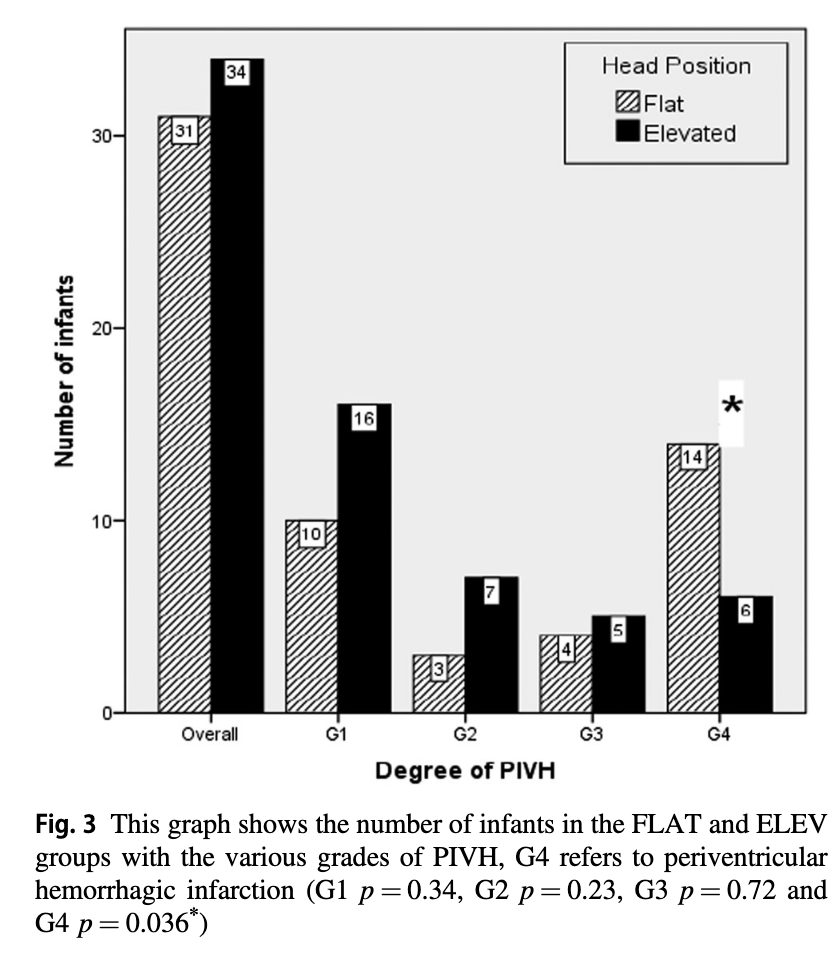
Ultrasounds were performed at entry into the study and then daily for days 1-4 and then on day 7 with abnormal scans repeated weekly. In terms of IVH the authors noted no overall difference in rate of IVH. What they did find however was a statistically significant reduction in the rate of Grade IV IVH.
The p value for the finding of lower rates of Grade IV IVH was 0.036 so not strikingly significant but different nonetheless. Given that the venous drainage of the head is also dependent on the resistance to flow from the pressure in the thorax one can’t infer that the intervention alone is responsible for this without ensuring that that respiratory findings are similar as well. Similarly without knowing inflow of blood into the head as measured by blood pressure it is difficult to say that the reduction in IVH isn’t related to differences in blood pressure.
The authors helpfully looked at both of these things. For those infants on high frequency ventilation the mean airway pressure was higher on day one being 11.5 cm H2O (FLAT) vs 9.9 cm H2O (ELEV) neither of which are high although different. The rest of the three days were no different. For those on conventional ventilation the only difference was on day 4 where the MAP was higher for ELEV at 8 vs 7.4 cm H2O which again is fairly mild. Interestingly, as was found in other studies that oxygenation was improved with elevation of the head, the maximum FiO2 for the two groups was different on day 1 being 46% in the FLAT vs 37.5% in the ELEV.
Looking at the hemodynamic side of things there were differences in the lowest mean BP recorded on day 1 and 3 but otherwise the groups were similar. It would have been nice to see mean results during this time rather than lowest but this is what we have.
In terms of complications of preterm birth there were no differences found in rates of sepsis (important given the increase rate of prolonged rupture in the FLAT group), NEC or ROP.
Although length of stay was no different 92 vs 109 days ELEV (NS), survival to discharge was at 88% vs 76% (p=0.033) which also may explain the longer length of stay.
What Can We Learn From This
Don’t worry. I am not about to throw the results out. There are a couple observations though that need to be addressed. The first is the increased rate of preecampsia in the ELEV group. This finding could have impacted the results. We know that fetuses exposed to this condition are stressed and are often born with better lungs than their non-exposed counterparts. The endogenous increase in steroids due to this stress is attributable and may explain the better oxygenation and lower mean airway pressures needed in the ELEV group rather than improvements in flow alone from positioning. The second issue is adherence to the protocol as there were some infants in the ELEV group who were placed flat for the final 1-2 days of the study. Having said that, this would serve to dilute the effect rather than strengthen it so perhaps it makes the results more believable.
So where does this leave us? This study demonstrates improved survival and a reduction in Grade IV IVH without an overall reduction in IVH. There was nothing found to suggest that the intervention is harmful. Given the background studies demonstrating improved systemic oxygenation, reductions in ICP and cerebral blood volume the finding of reduced severe IVH seems plausible to me. This could be a practice changing study for some units who have perhaps only adopted midline positioning in the first few days of life. It will be interesting to see if this takes off but is certainly worth a good look at.
It isn’t often in Neonatology these days that something truly innovative comes along. While the study I will be discussing is certainly small I think it represents the start of something bigger that we will see evolve over the coming years.
There is no question that the benefits of mother’s own milk are extensive and include such positive outcomes as improved cognition in preterm infants and reductions in NEC. The benefits come from the immunological properties as well as the microbiome modifying nature of this source of nutrition and have been discussed many times over. Mother’s own milk contains a couple of very special things that form the basis of the reason for the study to be presented.
What are neurotrophins and stem cells?
Before discussing the study it is important to understand what these two classes of molecules and cells are capable of. Neurotrophins are molecules that have the capability of promoting growth and survival of neural cells. Included in this class are EGF, brain-derived neurotrophic factor, glial derived neurotrophic factor, nerve growth factor, insulin-like growth factor-1, and hepatic growth factor. It turns out that not only are these found in high concentrations in breast milk but that a woman who produces breast milk at early gestational ages has higher amounts of these substances in her milk. Pretty convenient that substances promoting development of the brain and survival of brain cells increase the earlier you deliver! Stem cells are pluripotent cells meaning that they can develop into pretty much any cell type that they need to in the body. This would come in handy for example if you needed some new cells in the brain after a neurological insult. These are also present in mother’s milk and in fact can represent as much as 30% of the population of cells in breast milk.
The Nasal Cavity and the Brain
Clearly, the distance from the nasal cavity to the brain is relatively short. Without going into exhaustive detail it has been demonstrated in animal models that provision of medications intranasally can reach the brain without traversing the blood stream. This affords the opportunity to provide substances to the neonate through the nasal cavity in the hopes that it will reach the brain and achieve the desired effect. When you think about it, newborns when feeding have contact between the whole nasopharyngeal cavity and milk (as evidenced by milk occasionally dripping out of the nose when feeding) so using an NG as we do in the NICU bypasses this part of the body. Is that a good thing?
Intranasal application of breast milk
Researchers in Germany led by Dr. Kribs published an early experience with this strategy in their article Intranasal breast milk for premature infants with severe intraventricular hemorrhage—an observation. In this paper the strategy;follows; 2 × 0.1 ml of his or her mother’s milk 3 to 8 times a day (0.6 to 1.6 ml total per day). The breast milk was freshly expressed, which means the milk was used within 2 h after expression. The daily application started within the first 5 days of life and was continued for at least 28 days to a maximum of 105 days.
The outcome of interest was whether the severe IVH would improve over time compared to a cohort of infants with severe IVH who did not receive this treatment. Importantly this was not a randomized trial and the numbers are small. A total of 31 infants were included with 16 receiving this treatment and 15 not. The two groups were compared with the results as follows.
The results don’t reach statistical significance but there is a trend at the bottom of the table above to having less progressive ventricular dilatation and surgery for the same. Again this is a very small study so take the results with a grain of salt!
Is this practice changing? Not yet but it does beg the question of what a properly designed RCT might look like. The authors predict what it might look like with a sham nasal application versus fresh mother’s milk. I do wonder though if it may become a study that would be hard to recruit into as when families are approached and the potential benefit explained it may be hard to get them to say anything other than “Just give my baby the breast milk!” Such is the challenge with RCTs so it may be that a larger retrospective study will have to do first. Regardless, be on the lookout for this research as I suspect we may see more studies such as this coming and soon!
* Featured image from the open access paper. (There couldn’t be a better picture of this out there!)


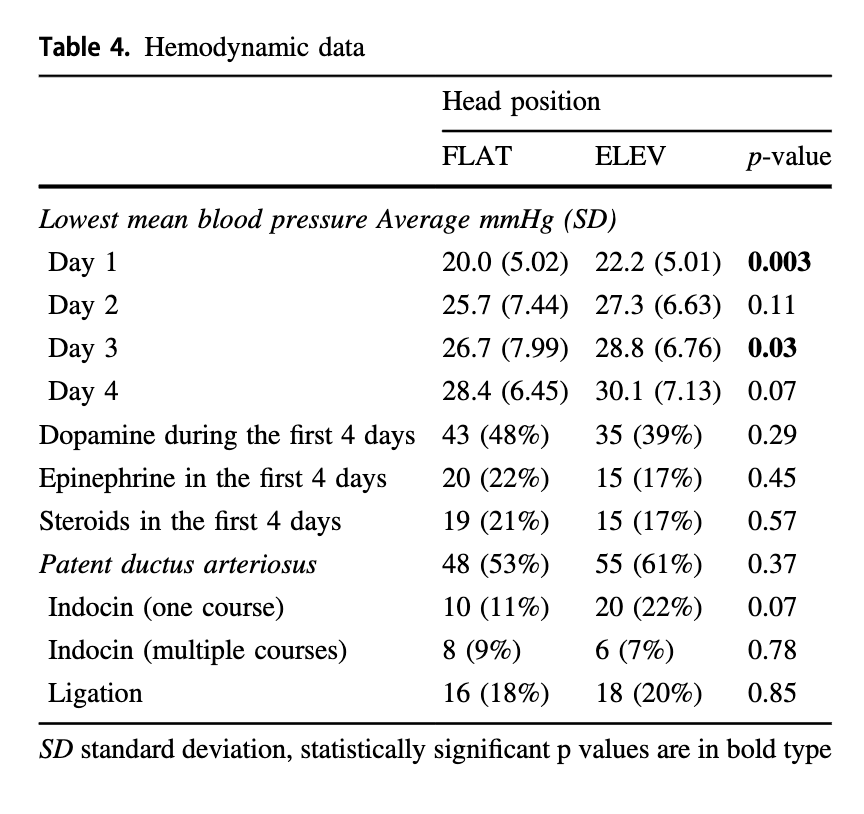 It would have been nice to see mean results during this time rather than lowest but this is what we have.
It would have been nice to see mean results during this time rather than lowest but this is what we have.