

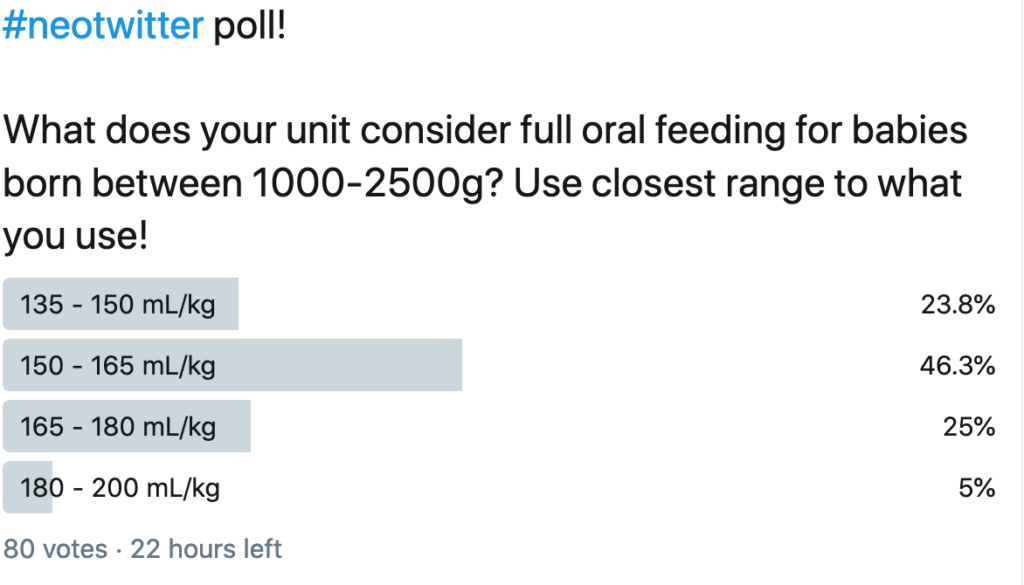
Since the dawn of my time in Neonatology there has been cibophobia! What is this you ask? It is the fear of food and with some flexibility in the definition I would apply this to large volumes of milk rather than the fear of food itself. Most units in the world seem to use a volume range of about 135 – 165 mL/kg/d as a range considered to mean “at full feeds”. As I was discussing this on rounds today I was quick to point out though that babies with neonatal opioid withdrawal syndrome (NOWS) frequently take in excess of 200 mL/kg/d and we don’t worry about it. The counter argument though is that these infants are “bigger” and should be able to tolerate a larger volume. As readers of this blog know I truly enjoy coming across papers that suggest a change to something considered dogma. Today is one of those days as I am choosing to explore in more depth an abstract that I posted to Twitter and Facebook last month.
On the day of this blog release I also took a poll on Twitter and found some interesting results that make this post all the more important to share. Take a look!
Are Bigger Volumes Better?
Travers CP et al chose to challenge this long held practice in their recent paper Higher or Usual Volume Feedings in Very Preterm Infants: A Randomized Clinical Trial. It was a simple yet wonderful trial that asked the question of whether for infants < 32 weeks GA at birth with BW from 1000-2500g would higher volume feedings of 180-200 vs 140-160 ml/kg/d help increase growth velocity. Randomization occurred after infants had reached 120 mL/kg/d of oral feedings. In both arms advancements from this point were the same and fortification occurrred as per usual practrice but in each arm strategies targeted individual fortification to weight gain.
The authors were seeking a 3 g/kg/d difference in growth and needed 224 infants to demonstrate this difference. They enrolled the same at a mean GA of 30.5 weeks and a BW of 1445 grams. Birth characteristics including gestational age, weight, sex, race/ethnicity, Apgar scores, head circumference, length,
and proportion of infants with a weight <10th percentile at birth did not differ between groups.
The outcomes showed differences as shown below.
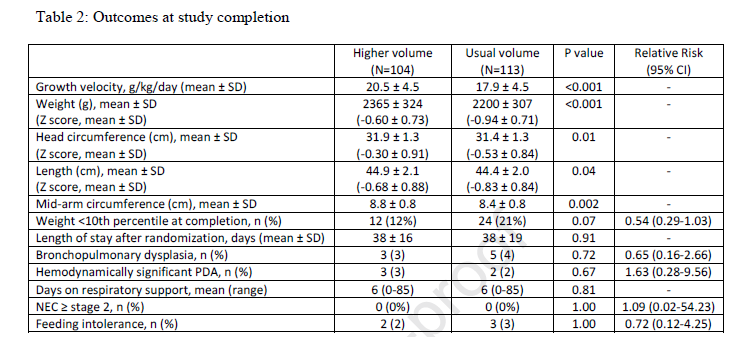
Looking at the results
All in all I would say the results are a smashing success. Growth velocity was improved and not just in weight but in head circumference and length. What I find interesting is that if fortification of milk was targeted regardless of the volume used I am a bit baffled as to why the growth rate would still be better but it was. The difference in caloric intake received between groups was approximately 9 kcal/kg/day at day 7 after study entry (126 kcal/kg/day versus 117 kcal/kg/day) and 16 kcal/kg/day from day 14 after study entry onwards (139 kcal/kg/day versus 123 kcal/kg/day).
Blinding here would have been a challenge as nurses and other health care providers would have been able to calculate the expected volumes at different fluid administration levels. Nonetheless there was a difference.
The question though that many would ask is whether this better growth came at the expense of greater morbidity. Let’s be clear here that the study was not powered to look at adverse outcomes and the numbers in the above table are small but no difference was seen nonetheless. To appease the most cautious of Neonatologists I suspect a larger study powered to look at adverse outcomes will be needed. What this study does though is raise the question of whether we can and should try larger volumes. As the title suggests I wonder about getting bigger faster so one can go home. With this more rapid rate of growth can we expect a faster maturation as well? I doubt it but it is something to certainly question in a larger study!