Giving bronchodilators to preemies on a ventilator has certainly been tried before. The major issue to contend with is getting the drug to where it is supposed to be. Anyone reading who has a child with asthma knows that you should use an aerochamber when taking a puff to help with better distribution to the lung. Giving a puff or two without it largely ends up on the back of the throat. Similarly, giving puffs through an endotracheal tuberaises questions about how much of the medication winds up on the plastic tube rather than the smooth muscle of the airways where the medication is intended to be. This has been looked at in a cochrane review as well entitled Bronchodilators for the prevention and treatment of chronic lung disease in preterm infants
Can Albuterol Save The Day?
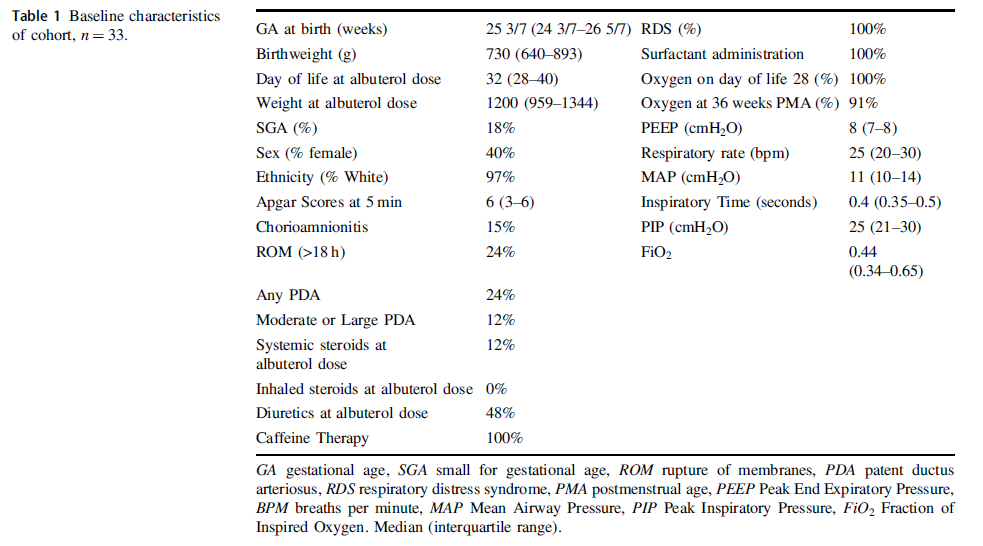
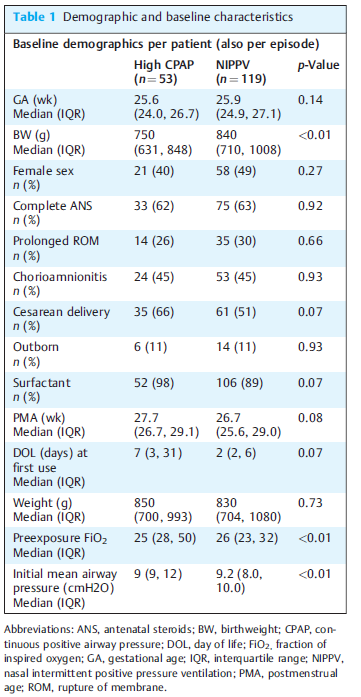
Albuterol is a beta agonist much like ventolin that can act on the smooth muscle of airways to achieve bronchodilation. Considering that preemies with immature lungs may have issues with both resistance and compliance, Raffay TM et al in their paper Response to first dose of inhaled albuterol in mechanically ventilated preterm infants chose to examine responsiveness in a group of 33 infants (all < 30 weeks at birth) to albuterol. Ideally, responsiveness would be done by pulmonary function testing but given that this was not possible in these infants they chose to examine other indicators of impact. After giving two puffs of 90 mcg of albeterol via a metered dose inhaler without an aerochamber the authors looked at changes in FiO2 as well as compliance and resistance measurements on the ventilator as a means of determining responsiveness. Ultimately, could they get drug into the distal airway in patients who were ventilated at about a month of age as shown in table 1 along with other baseline characteristics?
What makes this different than other studies I suppose is the use of the ventilator measurements and their use of histogram data on oxygen saturation to ascertain responsiveness to treatment. This was an observational study based on a secondary analysis of a previous study so we don’t have sham controls to compare to. Having said that by administering the medication and seeing what happens immediately afterwards it is possibile to get a sense of whether the drug had an effect.
So What if Any Effect Did It Have?
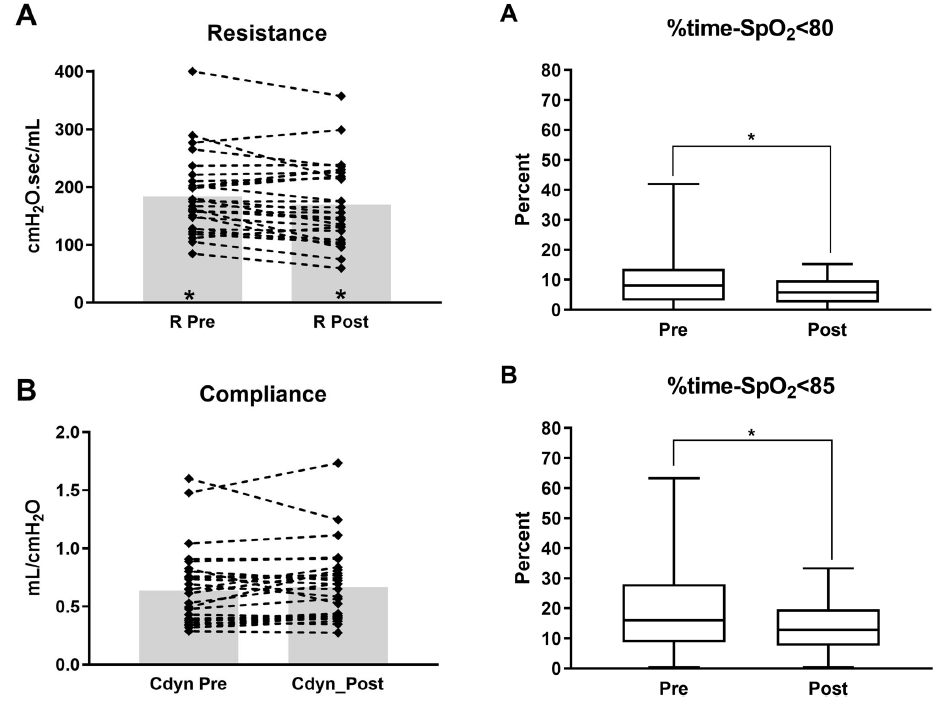
From the figure in the paper the answer is some effect. Overall, post albuterol resistance for the 33 patients overall was found to decrease. Compliance and FiO2 (not shown in the graphs below) did not change though. What did change however was the percentage of time spent below 80 and 85% respectively comparing a 4 hour window pre and a 4 hour window post with respect to histograms from the patient monitor.
Putting it together
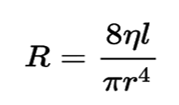
Ok so this isn’t a gold standard RCT looking at placebo treatments vs albuterol. It is hypothesis generating though as if resistance was decreased by albuterol one could expect improved delivery of O2 to the distal alveoli and therefore better oxygenation which is what is seen here. Should we be surprised that no difference in compliance is seen with albuterol therapy? I don’t think so as the effect of the drug is not on the distal alveoli and parenchyma but rather the more proximal branching airways. SInce airway resistance is governed by Poiseuille’s Law (you thought physics was over in high school?!) you can see that resistance (R) is directly proportional to the viscosity (n) and length (l) of the airway but inversely affected by the radius (r) to the 4th power. In other words if the radius of the airway after albuterol increases by 25% that effect is amplified to the 4th power in terms of reducing resistance.
I suppose I am buying what they are selling here but again the key is finding a method of getting the drug to deposit not in the trachea or proximal bronchi but to the lower airways. I can’t help but wonder if use of high frequency jet ventilation which carries flow down the centre of the airway might be a very effective way of getting such puffs further into the lung. Speculation of course but perhaps someone a little more creative than I can figure out how to do that and test deposition.
Should we use this routinely? Probably not as an everyday approach but it does make me wonder about those babies who are having a bad day so to speak. If one can glean from the ventilator that resistance has increased from one day to another might this be something worth trying? The authors found that the first treatment was effective but second and third not so much so to me this may just be a “hail mary” that is worth trying when nothing else seems to be working to reduce FiO2 in the presence of increased resistance.
If anyone is doing this routinely I would be curious in hearing your own experiences.
If you work in Neonatology you talk about caffeine endlessly whether addressing your own consumption or that of your patients. Our unit like many others typically starts caffeine early in a prophylactic fashion for babies under 32 weeks. The reason for this is due to the high incidence of apnea (AOP) in this population. The incidence of AOP follows an inverse relationship with GA, affecting 50% of those born at 30 weeks versus 7% at 34-35 weeks. Using caffeine in a more therapeutic approach is certainly sensible for babies older than 32 weeks given the lower likelihood of events. People who argue for a prophylactic strategy cite lower incidence of BPD and PDA from the CAP study while those on the side of reserving treatment for those who really need it put more emphasis on potential adverse effects such as polyuria, tachycardia and electrolyte disturbances. I have already revealed my bias as our centre takes a prophylactic approach but the question is whether it is still right given that the CAP study was many years ago now. A new study emerged this week that was shared on Twitter and generated some interesting discussion. So interesting in fact that I thought there was no better place to discuss this paper than here.
Head to Head Comparison
Elmowafi M et al published Prophylactic versus therapeutic caffeine for apnea of prematurity: a randomized controlled trial this month. This trial included 90 infants in the prophylactic arm (caffeine started < 72 hours of age) vs 91 in the therapeutic arm (only started in presence of apnea or if a baby needed mechanical ventilation and all infants were under 32 weeks of age at birth. Unfortunately, while the study was prospecitve it was not blinded although the authors state that in the therapeutic arm a neonatologist who was not part of the study team made the diagnosis of AOP. Caffeine dosing was standardized using the citrate form at 20 mg/kg as a load and with 10 mg/kg maintenance dosing (divide by 2 for base equivalents).
The primary outcome was total duration of oxygen support and a sample size was chosen based on a previous pilot RCT and the expectation that they could show a reduction in O2 requirement of 7 days in the prophylactic group. Looking at the baseline characteristics of the groups the only difference was the median day of starting caffeine which for the prophylactic group was day 1 and for therapeutic day 3.
Results
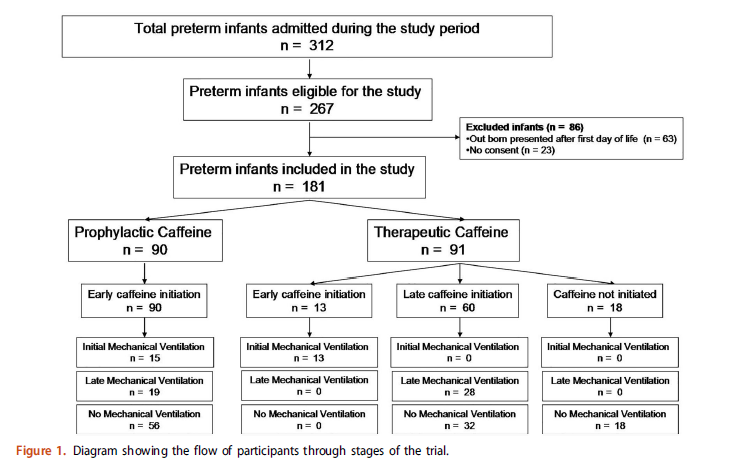
What happened in both groups and the reasons for starting caffeine are shown in teh following diagram.
As you can see, 13 patients were started due to need for initial mechanical ventilation, 28 for late mechanical ventilation with the rest being apnea as a reason except for 18 patients who never needed caffeine. When looking at the whole patient population the primary outcome was no different between the groups using an intention to treat analysis.
What the authors did next is where the controversy comes from but has some interesting data nonetheless. They did a “per-protocol analysis” on the whole group and found the following:
Per protocol analysis showed that prophylactic caffeine therapy was associated with a significant reduction in the duration of oxygen therapy compared to therapeutic initiation among included preterm infants [median and IQR of 28 (18–36) days versus 34 (23–51) days, p¼.005 respectively].
Essentially what this means is they said let’s exclude those babies who never needed caffeine and just compare babies that all received caffeine in either arm. Now they see a difference of 6 days which is pretty close to the 7 days expected . Purests will note though that by doing so you can’t claim that the groups were balanced in terms of risk factors since the presented baseline characteristics are not necessarily still the same.
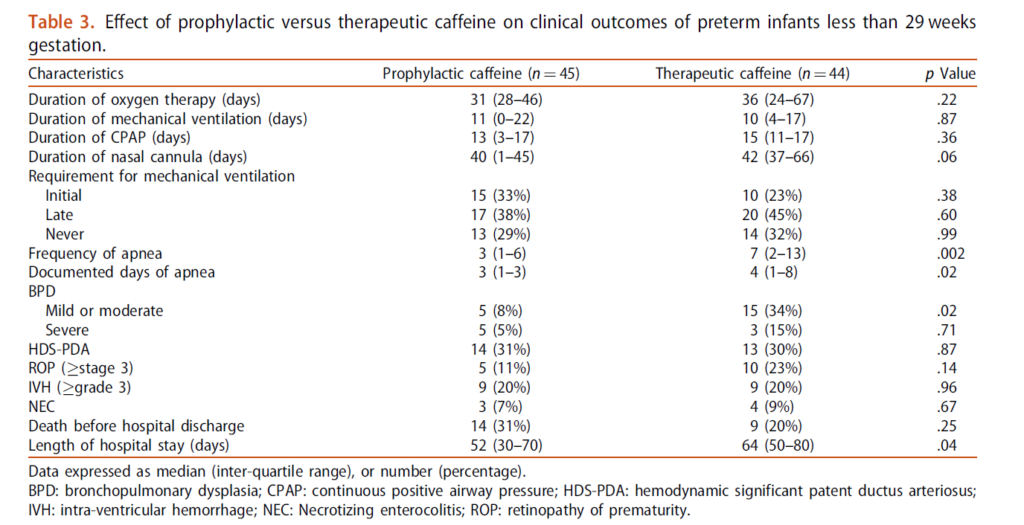
They went further though and asked the question. “What about a subgroup of <29 weeks?”. These babies are undoubedly higher risk for AOP and ventilation. Is the problem that the inclusion of babies 30-31 weeks diluted a potential benefit? Here is what they found.
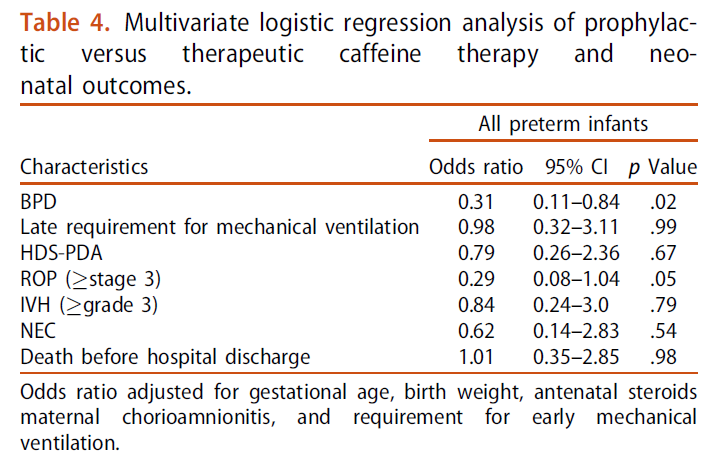
The main two things to draw your attention to are the marked reduction in mild to moderate BPD and shorter length of stay in hospital. Moreover when they looked at risk of BPD for the whole group they found a reduction in risk. Importantly there was no difference in adverse effects from caffeine use in either arm of concern.
What Can We Take From This?
Any discussion about adverse effects needs to acknowledge that these are short term outcomes we are looking at. Do babies who have never received caffeine do better in the long run? The CAP study did not suggest that was the case but it was a different time with different babies. Do I think caffeine is harmful? No I don’t, especially in the babies who would otherwise experience multiple apneic events or prolonged ventilation.
What this study does raise in my mind though is whether a change in approach to prophylactic caffeine is warranted. The authors don’t specify (I don’t think) but I suspect the bulk of the babies who did not need caffeine were in the 30-31 week group. We know that positive pressure ventilation is harmful to the developing preterm lung. Providing caffeine in the first few hours of life in the hopes of avoiding invasive ventilation or shortening the course of ventilation is the main reason that we likely see consistent reductions in BPD with its use. Under 29 weeks I would certainly favour giving caffeine early but above that as the risk of BPD drops considerably is a watch a wait approach a reasonable one to take? As this study was unblinded it is possible the babies were treated differently with respect to ventilation and apnea managment but I do think the risk is low. If the attendings caring for the babies were not part of the study and knew they were free to give caffeine if needed there may be less risk of bias.
In the end the results of this study in essence are supportive of my practice. I suspect they support many others as well. To answer the question really about side effects I suspect we would need much larger sample sizes than this with adequate power to detect differences but for now I will continue to say “give it and give it early!”
As awful as COVID19 has been over the last year and a half one thing has continued to perplex myself and others. Why do babies whethe term or preterm so rarely acquire the virus? Numerous studies have been able to document placental changes and infection of these tissues. On rare occasions reports have come out with evidence of neonatal infection but fortunately most are mild.
These findings have in large part contributed to the Canadian Pediatric Society practice points on three topics.
In this post an argument was made that the reason these infants are resistant is due to low levels of ACE-2 receptors in the nasal mucosa of children. In this study children as young as 4 years of age were found to have very low levels of this receptor (portal of entry for SARS-CoV-2) into the host. I speculated at the time that if one carried forward the findings to younger children and infants you might find there were hardly any receptors at all.
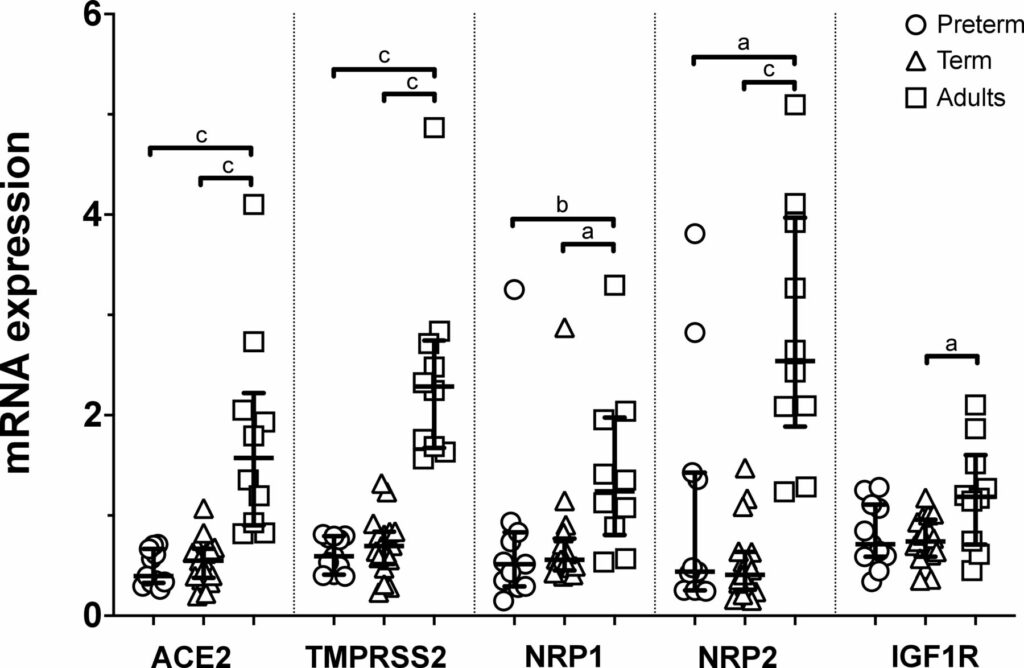
Well, someone finally did the study and confirmed what I suspected. The study report is entitled Nasal expression of SARS-CoV-2 entry receptors in newborns by Heinonen S et al. It’s not a big study but the results are consistent across 28 newborns (17 term and 11 preterm) and 10 adults. In each newborn whether term or preterm a nasal mucosal scraping was performed at 24 hours of age and used to measure by reverse-transcription quantitative PCR mRNA expression of ACE2, transmembrane serine protease 2 (TMPRSS2), neuropilin 1 (NRP1) and neuropilin 2 (NRP2) and insulin-like growth factor 1 receptor (IGF1R).
What the results show you is that babies are not just small adults. They are different yet preterm do not seem to be that different than term infants in terms of receptors. While ACE2 has garnered most of the attention when it comes to receptors for SARS-CoV-2 the others also play a role and are in general expressed to a lesser degree in neonates than adults.
Conclusions
In the previous post I argued what was in your nose makes a difference to your risk of contracting SARS-CoV-2. Really the point is what is not in your nose. Thankfully neonates do not have good expression of these receptors and that may be the biggest reason for the general protection they have from this pandemic. It has certainly a good time to be in the “have not” group!
A couple years back at the Canadian Pediatric Society annual meeting a discussion broke out about extubating infants to higher levels of CPAP. Conventional thinking had been to use levels between 5 – 8 cm H2O typically. I shared with the group the experience we had in Winnipeg (unpublished) of using higher levels from 9 -12 cm H2O with some degree of success in allowing earlier extubation. The group thought it was interesting but pointed out the lack of robust research in the area so were not so keen to “try it out”. Non-invasive positive pressure ventilation (NIPPV) has been used for some time in the neonatal world and has been compared to CPAP for extubation success and found to be superior as in this review Comparison of Complications and Efficacy of NIPPV and Nasal CPAP in Preterm Infants With RDS. In this review though as in others more typical CPAP levels are used so the question is whether the same efficacy would be seen with high level CPAP vs NIPPV.
Canadian Study to the Rescue
The study here is by Ahmad HA et al Comparison of High CPAP versus NIPPV in Preterm Neonates: A Retrospective Cohort Study and seeks to answer this question albeit in a retrospective fashion. The study is not well controlled since it is retrospective but it may be the best we have for now. Over a 3 year period the authors examined the outcomes for babies trialed on high CPAP (hCPAP of at least 9 cm H20) vs NIPPV. In each case they looked at the first episode of use. The modalities could have been used for extubation or as a primary means of support. The primary outcome was failure of the modality as defined by either intubation or change to the other strategy within 7 days. A total of 53 infants received hCPAP vs 119 NIPPV. Why the big difference? Since this was retrospective and not randomized it was up to the individual practioner which modality they wanted to try. If the majority of the unit favoured NIPPV this is why there would be such a difference. Herein lies the benefit of the primary outcome as if “conventional wisdom” was wrong and the other modality would be better then we should see a greater movement to the other strategy or more intubations in one group suggesting superiority of one vs the other.
The groups however aren’t entirely equivalent at baseline. The babies in the hCPAP group are quite a bit smaller on the one hand which would favour the NIPPV group. On the other hand there is almost a significant difference in surfactant provision for the hCPAP arm which might favour the hCPAP group. The other thing also nearing statistical significance is when the intervention was trialed. The median time is 2 days for teh NIPPV group and 7 for hCPAP suggesting one may have been used more prophylactically and the other post extubation. Different strategies might make a difference to outcome? Also no infants received MIST or INSURE and all were started on traditional lower levels of CPAP prior to surfactant.
Results
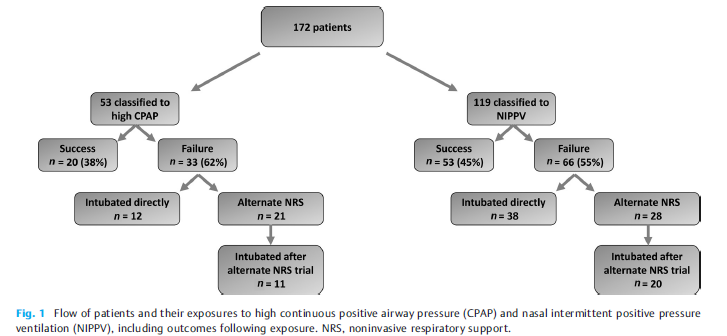
The results tell an interesting story (I think) with the primary outcome being no different 62% in the hCPAP vs 55% with NIPPV. Looking at the patient outcomes in the figure from the paper one gets a little more detail and can surmise how people viewed the two modalities as a strategy and can see they were a bit different.
There seems to have more confidence in the unit with NIPPV as a way to prevent intubation. For those that failed hCPAP 12/33 were intubated as the next step (about a third) while the other 2/3 were trialed on NIPPV. Looking at those started out on NIPPV, 38/66 were intubated directly 58% or almost 2/3 while 28/66 were trialed on hCPAP. Of the ones trialed on hCPAP 20/28 or 71% were still intubated. Comparatively of those who were changed from nCPAP to NIPPV 11/21 were intubated or about 50%.
The authors find no difference in the primary outcome which is true. The problem of course with this analysis though is that there was no standardization with determining when one would choose to intubate. This issue can really play with the results. Let’s say for example that one Neonatologist really believes for the most part that NIPPV is the mode that can really prevent intubation more than hCPAP. It is conceivable that the reason in crossover intubations are less with NIPPV is that people were willing to tolerate a slightly higher pCO2 or a couple more apneas since they believe the modality is best and the infant will “get better soon”. On the other hand, infants already on NIPPV who are deteriorating might be intubated more readily as the attending might think “this hCPAP is a bunch of malarky”
It is worth mentioning that the incidence of air leak was no different between the two, nor was NEC or feeding intolerance from exposing the babies to such high pressures.
Conclusions
The study doesn’t “prove” anything. I don’t see it as a complete waste though as it does a number of things. It does show that small infants can be managed with hCPAP in NICU without any significant increase in complications. It also sets the stage for a couple future prospective trials I can see. Firstly, a trial of traditional CPAP vs hCPAP is needed as some units don’t have access to NIPPV or simply don’t use. The second is a prospective trial with clear parameters for failure between hCPAP and NIPPV. Lastly, the authors ran the NIPPV and CPAP off ventilators in the units. The work of breathing would be potentially different with the use of devices solely designed for CPAP with fluidic flips. It would be important to use optimal devices for both modalities in such a trial and I for one can’t wait to see them.
What can I say? I have had a love affair with research on hypoglycemia. I suppose ever since my colleague and I began the quest of rewriting the Canadian Pediatric Society statement The screening and management of newborns at risk for low blood glucose it has become an interest. Embedded in the statement is commentary on the use of glucose gels for management of neonatal hypoglycemia and based on the sugar babies trial that found treatment of hypoglycemia with dextrose gel reduced admission for hypoglycemia and improved rates of breastfeeding after discharge I have been a proponent. A new approach has arisen in a large study in neonates that warrants some discussion. It tackles hypoglycemia from a preventative approach rather than as a treatment per se and is presented below.
The hPOD Study
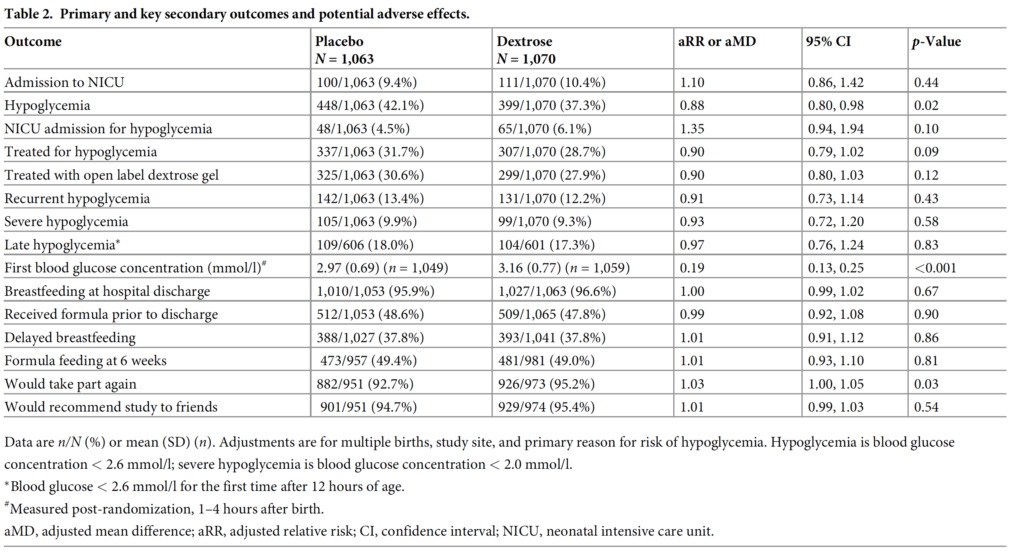
The same group from Auckland led by Jane Harding published a preventative trial in January entitled Evaluation of oral dextrose gel for prevention of neonatal hypoglycemia (hPOD): Amulticenter, double-blind randomized controlled trial. The study approached the problem of hypoglycemia by looking at whether provision of dextrose gel at 1 hour of age along with a breastfeed could reduce admission to NICU. The targeted population were babies with risk factors for hypoglcyemia such as maternal diabetes, late preterms and SGA or LGA infants. Remarkably this multicentre study managed to randomize 2149 infants into dextrose (1078) and placebo 1071) arms which for a neonatal study is pretty big! Blood glucose levels were analyzed on all at risk infants at 2 hours of age and were then followed up every 2-4 hours for the first 12 hours of age and until there were 3 consecutive measurements greater than or equal to 2.6 mmol/L. Given the size of the study it should come as no surprise that the two groups were similar in terms of baseline characteristics. The most common risk factor for hypoglycemia in each group was maternal diabetes at 81% in each group.
In the end the only thing that was different between the two groups was a diagnosis of hypoglycemia with about a 5% reduction in the outcome. Admission to NICU was no different whether it was for any reason or hypoglycemia alone. Treatment with IV therapy was also no different between groups and in addition breastfeeding rates were exceptionally high at discharge at about 96% for both groups. So the conclusion here is that prophylactic glucose gel doesn’t matter much but I have a few thoughts despite this being a VERY large trial and the authors really doing a good job of answering an important question.
My Thoughts on the Outcomes
The study demonstrates that one dose of glucose gel does not affect admission for any reason or for hypoglycemia. I can’t help but wonder if allowing the dextrose gel group to receive one or two more doses could have changed that outcome.
No difference in admission is not surprising since there are many reasons that a baby could be admitted with those underlying risk factors. Low birth weight, TTN, RDS etc would be some reasons and I wouldn’t think would be any different. It might have been better to power the study for admission for hypoglycemia as that to me is the only reason for admission that could be impacted by such prophylaxis.
When your breastfeeding rate in the placebo arm is at 95.9% there really isn’t much room for improvement so not sure a lack of improvement with dextrose gels can really be called here. There really wasn’t anywhere to go but down and previous work suggested that rates can go up. As the saying goes, can you apply the results of the study to my population. I can only wonder what would have happened if the authors were to replicate this study in a population with breastfeeding rates of 80%.
Is the outcome of reduced hypoglycemia a good enough outcome alone to adopt prophylactic dextrose gel? I don’t think so as there was no difference in groups between recurrent or severe hypoglycemia which is what likely matters most to neurodevelopmental outcome. Curiously the mean initial blood glucose was 2.97 and 3.16 in the placebo and glucose gel arms respectively so I am not sure how hypoglycemic this population really was. Yes there were about 40% in each arm that were hypoglycemic but only 10% were severe and almost 90% never had another episode. It’s possible that just by chance these children were on a very mild spectrum and therefore prophylaxis had little effect since they really were only going to have transient hypoglycemia.
In spite of my comments above I believe the authors did a fine job trying to answer an important question which to be honest others have wondered about before. For now I won’t be recommending this in my own institution but I do wonder what project will come next from this group that keeps on producing great work in the area of neonatal hypoglycemia.