If you work in NICU you will have seen many babies who have passed through the stages of apnea, weaned off respiratory support and have reached a sufficient weight for discharge but alas will just not feed. Different strategies have been employed to get these infants feeding that rely in many cases on a cue based approach but in the end there are some that just won’t or can’t do it. Many of these babies will be sent home either with NG feedings or if it appears to be a more long term situation a gastrostomy tube. For this blog post I am going to present to you some novel research that suggests there may be another way to approach this and would like to thank one of the followers of my social media for alerting me to this work. You know who you are as the saying goes!
This was an open label Phase 0 trial (few patients as a pilot) using taVNS to help improve feeding in ex-preterm or 3 recovering from HIE infants who were now past term and all headed towards a gastrostomy tube. The hospital carrying out the study entitled Transcutaneous Auricular Vagus Nerve Stimulation-Paired Rehabilitation for Oromotor Feeding Problems in Newborns: An Open-Label Pilot Study by Badran BW et al did not come out of thin air. Prior research in adult patients recovering from stroke found in multiple studies (all referenced in the paper) that motor stimulation accompanied by VNS improves motor function recovery. The objective here then was to see if stimulation of the auricular nerve along with assessment and motor treatments from an occupational therapist once a day could help improve feeding and avoid GT placement. The trial overview is as shown below.
The centre in which the study was done had a historical rate in this population of <10% of such patients avoiding a GT (all reaching term equivalent age and not showing an improvement in feeds). This was demonstrated in previous work by at the Medical University of South Carolina (MUSC). “Preterm infants who have not reached full PO feeds by 40-week gestational age (GA) and/or after 40 days of attempting PO feeds have a >90% chance of eventually needing G-tube implantation to achieve full enteral feeds (Ryan and Gehle, 2019).”
The Intervention
taVNS was done once a day during a bottle feed and timed with observed suckling and swallowing by an OT. The stimulation was stopped during a pause in feeding.
As you read this you may be concerned about side effects (as I was) of passing an electrical current to the ear and stimulating the auricular branch of the vagus nerve. This has been shown in other work to activate both afferent and efferent pathways of the vagus nerve and enhance plasticity and functional motor recovery. Could you then apply the same to improving development of the motor pathways of the preterm newborn or patient recovering from HIE? The authors examined skin irritation, pain scores and incidence of bradycardia before and during feeding while stimulation was occurring and found no difference in any of the measures. In order to minimize pain the authors increased the current by 0.1 mA until they perceived stimulation by change in facial expression, shrugging or fidgety movements. In the event of an increase in pain scoring by 3 the dose was decreased by the same amount. in the end the intervention was deemed safe without any adverse effects.
The primary outcome was ability to increase and maintain full daily PO intake for 4 days (>120 mL/kg/d and maintain a weight gain of >20 g/day until discharge.
Why you should care about the results
If you work in a hospital like mine you would probably find that once the discussion about a GT placement begins, few miraculously avoid it. In this study they found that 8 of the 14 patients or 57% avoided the GT. Their historical achievement in this regard was <10%. This could be by chance of course since the study is a small one but when looking at the PO intake between non-responders and responders they demonstrate the following.
The authors found no statistically significant increase in the non-responders after the taVNS in PO feeds but also note there were three infants born to mothers with diabetes in this group. I have commented before on the effect of diabetes on successful feeding so this certainly could have affected the success of this group. If you look at the change over time in the responder group they look graphically like there was an upwards trend in the feeding ability prior to the intervention although the increase or slope of the improvement due to small numbers was not significant. The takeoff in feeding afterwards was.
The findings in this study are extremely exciting to me. As units across the globe struggle with patient flow, one of the most common reasons for these patients to stay in hospital is no longer BPD or apnea but inability to feed. The idea that such a simple intervention that is done once daily for 30 minutes might influence the development of feeding coordination in these at risk infants is phenomenal in terms of its impact on patient flow.
If you wonder about whether this is a one off study, there is a lot of active research in this area. A quick search of clinicaltrials.gov uncovers 61 studies on taVNS recruiting at the moment for a variety of ailments. In fact the next study is a Phase 1 trial aiming to recruit 40 patients and is underway. If interested the link to the study is here.
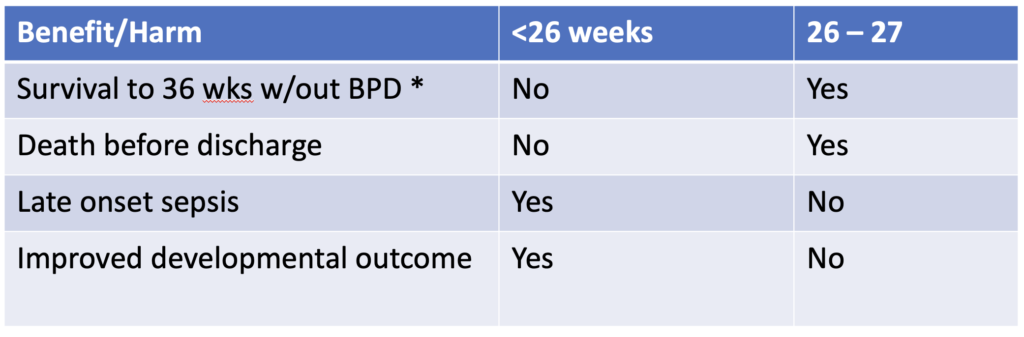
Precision medicine is a growing field in which genetic factors, environment, metabolism and even lifestyle are taken into account when deciding who should receive a treatment or not. When it comes to bronchopulmonary dysplasia I believe anyone who works in Neonatal care can attest it is a mystery why some infants go on to develop BPD while others don’t. We do know that certain treatment strategies may increase risk such as using excessive volumes or pressure to ventilate and in the last 25 years the notion that your level of cortisol in the blood may make a difference as well. I have written about prophylactic hydrocortisone use before in Hydrocortisone after birth may benefit the smallest preemies the most! When looking at the literature thus far and taking into account the results of the individual patient meta-analysis the following table can be generated highlighting a summary of benefits.
The question thus becomes if there is benefit for some infants under 26 weeks and then for some that are 26 and 27 weeks but there is also risk of harm, is there a way to select out those who are most likely to benefit with the least risk of harm.
A baby’s initial cortisol level may be the answer
The PREMILOC study was a double-blond multicentred trial of 523 infants randomly assigned to either prophylactic hydrocortisone in the first 24 hours of life or placebo. All infants were under 28 weeks at birth and received 1 mg/kg/d of hydrocortisone 1 mg/kg/d for 7 days followed by 3 days of 0.5 mg/kg/d for three days. In a pre-planned study coming out of the PREMILOC study, researchers looked at the role of baseline cortisol in predicting response to treatment or risk of adverse outcomes.
What they found in examining baseline levels for both treatment and placebo groups was that a relationship exists between the baseline level and such outcomes.
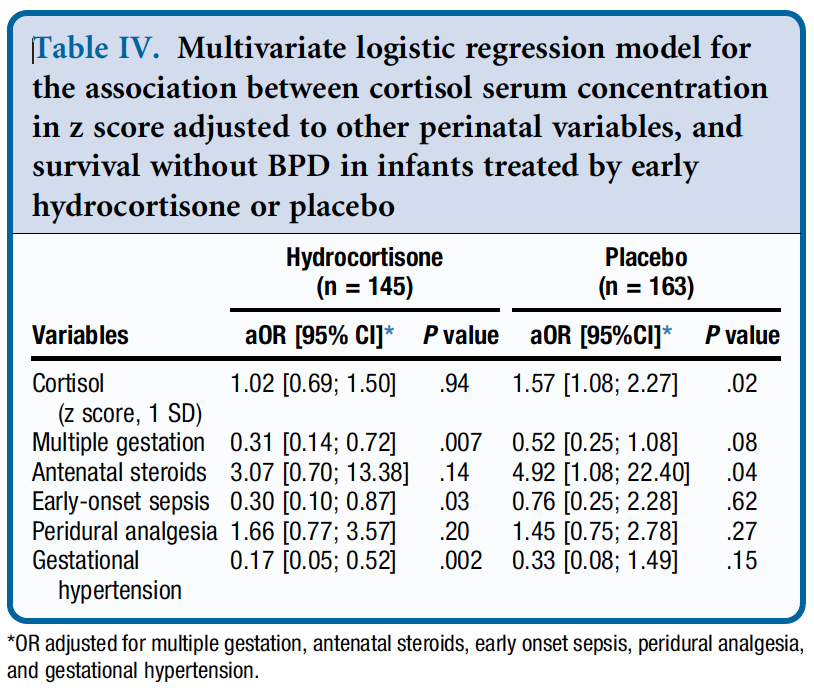
From Table 4 they found a relationship between survival without BPD and a higher initial level of cortisol but found no such relationship in the treatment arm. The threshold of what was considered high was 880 nmol/L although the mean cortisol was in the 400-500 nmol/L range. in other words, if having adequate physiologic levels of cortisol is the goal and a baby already has that, giving more non-antiinflammatory dosing of hydrocortisone doesn’t yield benefit.
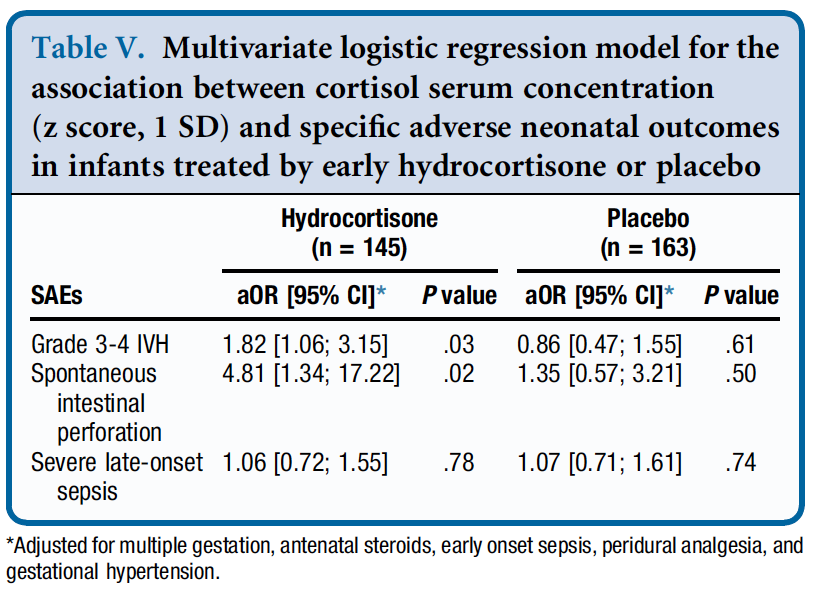
Similarly, when looking at side effects a positive correlation was found between higher baseline levels of cortisol and risk of grade III/IV IVH and spontaneous intestinal perforation. It would seem therefore that if a baby has the level of cortisol that they would normally have from a physiologic perspective they are no different than a placebo arm patient when given hydrocortisone as you bring them to where they need to be. When you double the dose however that they should have, side effects begin to rear their ugly head.
How can you use this information?
From personal conversations I know that many centres are struggling with what to do about giving hydrocortisone. On the one hand there isn’t much benefit (if at all) for BPD in the 24 and 25 week infants but they do better from a neurodevelopmental standpoint. On the other hand there is a benefit in the 26 and 27 week infants but you may predispose them to side effects as well.
This is where precision medicine comes in. One option for centers unsure of who to provide this to (if at all) could be to use a threshold of 880 nmol/L and if the initial level is above this you would not treat but if below offer treatment. This level while found in the study to be predictive of side effects in particular if high does seem very high to me. I would think most babies would qualify which is not necessarily a bad thing but in our center we have typically used levels above 400 or 500 as an adequate stress response. Regardless of the level picked one would be using physiologic data to determine who to give hydrocortisone to as a way to try and maximize benefit and minimize harm for the individual patient.
Make no mistake. Regardless of whether you decide to try this for your patients I don’t believe this is a magic bullet. The best chances for our patients come from having bundles of evidence based based practices and applying them to the patient population if we hope to reduce BPD and minimize risk from any side effects of our treatments. The question is whether prophylactic hydrocortisone should be part of this bundle.
This could turn into a book one day I suppose but I have become interested in chalenging some of my long held beliefs these days. Recently I had the honour of presenting a webinar on “Dogmas of Neonatology” for the Indian Academy of Pediatrics which examined a few practices that I have called into question (which you can watch in link). Today I turn my attention to a practice that I have been following for at least twenty years. I have to also admit it is something I have never really questioned until now! In our institution and I suspect many others, infants born under 1250g have been fed every two hours while those above every three. The rationale for this has been that a two hour volume is smaller and causes less gastric distention. This in theory would benefit these small infants by helping to not compromise ventilation or lead to reflux. Overwhelming the intestine with large distending boluses would also in theory lead to less necrotizing enterocolitis. All of this of course has been theoretical and I can thank those who preceded me in Neonatology for coming up with these rules!
Study Challenges This Old Belief
Yadav A et al published Two-hourly versus Three-hourly Feeding in Very Low Birthweight Neonates: A Randomized Controlled Trial out of India (well timed given my recent talk!). The authors randomized 175 babies born between 1000-1500g to either be fed q2h vs q3h once they began protocol feeding. The primary outcome was time to full feedings. Curiously, the paper indicates they decided to do a preplanned subgroup analysis of the 1000-1250 and 1251 -1500g groups but in the discussion it sounds like this is going to be done as a separate paper so we don’t have that data here.
The study controlled conditions for determining feeding intolerance fairly well. As per the authors:
“Full enteral feed was defined as 150 mL/Kg/day of enteral feeds, hypoglycaemia was defined as blood glucose concentration <45mg/dL [15]. Feed intolerance was defined as abdominal distension (abdominal girth ≥2 cm), with blood or bile stained aspirates or vomiting or pre-feed gastric residual volume more than 50% of feed volume; the latter checked only once feeds reached 5 mL/kg volume [16]. NEC was defined as per the modified Bells staging.”
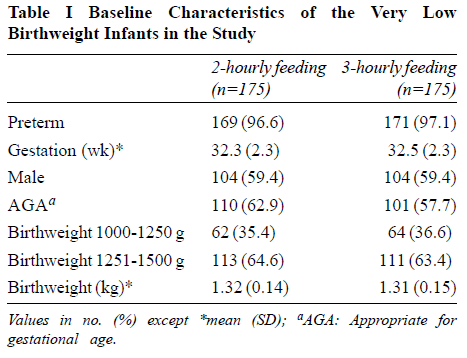
We don’t use gastric residuals in our unit to guide cessation of feedings anymore but the groups both had residuals treated the same way so that is different but not somethign that I think would invalidate the study. The patients in the study had the baseline characteristics shown below and were comparable.
Results
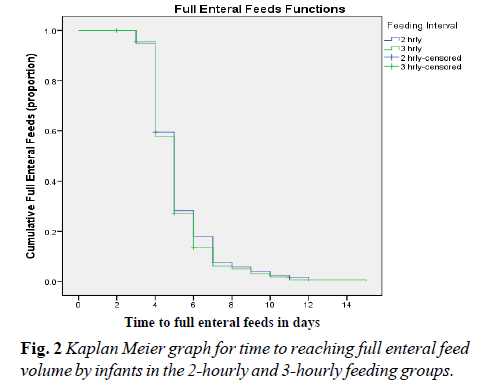
It will be little surprise to you that the results indicate no difference in time to full feedings as shown in Figure 2 from the paper.
The curves for feeding advancement are essentially superimposed. Feeding every two vs three hours made no difference whatsoever. Looking at secondary outcomes there were no differences as well in rates of NEC or hypoglycemia. Importantly when examining rates of feeding intolerance 7.4% of babies in the 2 hour and 6.9% in the 3 hour groups had this issue with no difference in risk observed.
Taking the results as they are from this study there doens’t seem to be much basis for drawing the line at 1250g although it would still be nice to see the preplanned subgroup analysis to see if there were any concerns in the 1000-1250 group.
Supporting this study though is a large systematic review by Dr. A. Razak (whom I have collaborated with before). In his systematic review Two-hourly versus three-hourly feeding in very low-birth-weight infants: A systematic review and metaanalysis. he concluded there was no difference in time to full feeds but did note a positive benefit of q3h feeding in the 962 pooled infants with infants fed 3-hourly regainin birth weight earlier than infants fed 2-hourly (3 RCTs; 350 participants; mean difference [95% confidence interval] -1.12 [-2.16 to -0.08]; I2 = 0%; p = 0.04). This new study is a large one and will certainly strengthen the evidence from these smaller pooled studies.
Final Thoughts
The practice of switching to q2h feedings under 1250g is certainly being challenged. The question will be whether the mental barriers to changing this practice can be broken. There are many people that will read this and think “if it’s not broken don’t fix it” or resist change due to change itself. The evidence that is out there though I would submit should cause us all to think about this aspect of our practice. I will!
Some time ago Nick Hall from Graham’s Foundation posted the following question on Linkedin:
Private room vs open bay for the NICU. Can always get a quote from a parent saying it is great but….? At what cost? Impact on staff? Is parent time in those NICUs greater now? Other alternatives?
Included in the post was an article discussing the benefits of such a design. Below I will look at the benefits and risks and conclude with an answer to his last question.
The NICUs of the 1970s through late 1990s have been described as “barn like” or “open concept” but in recent years the belief that single patient rooms (SPR) would offer greater benefit to infants led to the adoption of such a unit design across North America. The imagined benefits would be related to improved parent comfort, creating a desire for families to spend more time with their children. As we move to a “family centred” approach to care, a key goal of all units should be to make their families as comfortable and stress free as possible in order to have a positive experience.
Detractors meanwhile, speak of concern regarding isolation of such infants when families do not visit and moreover a risk that such infants deprived of sensory experience will have impaired development. Last year a paper was published that did not help quell such fears; Alterations in Brain Structure and Neurodevelopmental Outcome in Preterm Infants Hospitalized in Different Neonatal Intensive Care Unit Environments (full article in link). This study which compared infants cared for in SPR to an open unit (the hospital in this study had a mixture of both in their NICU) found a worrisome finding at 2 year follow-up in that the infants in SPR had lower scores on language and a trend towards lower motor scores as well. Additionally, partly explaining such findings may have been differences noted at term equivalent age in both the structure and activity of the children’s brains compared to those cared for in an open environment. We were starting construction on a new NICU at the time this paper was published and I can tell you the findings sent shockwaves through our hospital as many wondered whether this was the right decision.
Devil Is in The Details
Looking further into this study, the urban population bore little resemblance to our own. In our hospital all women are taught how to perform skin to skin care and the majority of our mothers spend a great deal of time with their infants. To see how successful have a look at our recent Kangaroo Care drive results! The families in this study however the average hours per week of parent visitation over the length of stay ranged from 1.8-104 hours with a mean of 19+/- 19 hours. The average number of days held per week over the length of stay was 0-6 days with a mean of 2.4 +/-1.5 days. The average number of days held skin-to-skin over the length of stay ranged from 0-4 days, with a mean of 0.7 +/- 0.9 days. In short they were hardly there.
Second Study Finds The Opposite
Later on in 2014 a second study on this subject was published; Single-family room care and neurobehavioral and medical outcomes in preterm infants. Infants < 1500g who were admitted to an NICU between 2008 and 2012 were compared with respect to medical and neurobehavioral outcomes at discharge. Participants included 151 infants in an open-bay NICU and 252 infants after transition to a SPR NICU.
Statistically significant results (all Ps ≤.05) showed that infants in the SPR NICU weighed more at discharge, had a greater rate of weight gain, required fewer medical procedures, had a lower gestational age at full enteral feed and less sepsis, showed better attention, less physiologic stress, less hypertonicity, less lethargy, and less pain.Nurses reported a more positive work environment and attitudes in the SPR NICU.
This study in fact demonstrated greater maternal involvement in a SPR with improvement in outcomes across the board. It would seem then that in a SPR environment, provided there is enough family visitation and involvement this model truly is superior to the open concept. Furthermore despite concerns by some nurses that the loss of line of sight to their patients will make for a more stressful working environment this does not seem to be the case.
What About Families Who Cannot or Simply Aren’t Visiting Frequently?
The reality is that there are many reasons for parents to be absent for long periods during their newborns stay. Having a home outside of the city with other children to care for, work obligations, or loss of custody and abandonment due to apprehension are just some of these reasons. In our hospital, at least 15-20% of all patients admitted are from outside Winnipeg. The evidence as I see it supports the move to a SPR but what do we do for those children who need more visitation? The solution is a cuddler program. In our new hospital we are grateful for the generosity of our Children’s Hospital Foundation who secured a donor to pay for a coordinator of such a program. The veteran parent who is leading this program ensures that no infant goes beyond a set period of time without feeling the touch or hearing the sound of a voice. Such a program is in fact already in place at our other tertiary hospital and was featured in a lovely article attached here. Taking all the information together that is out there I think that if we can provide the necessary stimulation from both touch and auditory stimuli as well we can provide these infants with the developmental needs that each of them requires.
The SPR is the right design in my mind for families with many benefits that spring forth in such an environment. This need not be a win-lose scenario for your hospital. Do not underestimate the power of a cuddler and don’t hesitate to seek support to initiate such a program. It could mean the difference from going from good to great!
In recent years we have moved away from measuring and reporting gastric residuals. Checking volumes and making decisions about whether to continue feeding or not just hasn’t been shown to make any difference to care. If anything it prolongs time to full feeds without any demonstrable benefits in reduction of NEC. This was shown in the last few years by Riskin et al in their paper The Impact of Routine Evaluation of Gastric Residual Volumes on the Time to Achieve Full Enteral Feeding in Preterm Infants. Nonetheless, I doubt there is a unit in the world that has not had the following situation happen. It is 2 AM and the fellow on call is notified that they need to come and see a patient. On arrival the bedside nurse shows them a syringe that contains dark green murky fluid. The fellow is told that NG tube placement was just being checked and this is what was aspirated. The infant is fine in terms of exam but the question is asked “What should I do with this fluid”. The decision is made that the fluid looks “gross” and they discard it and then decide to resume feedings with a fresh batch of milk. Both parties feel good about discarding what looked totally unappealing for anyone to ingest and the night goes on. If this sounds familiar it should as I suspect this happens frequently.
Logical Fallacy
A colleague of mine introduced me to this concept and I think it may apply here. Purdue University’s writing lab defines a Logical Fallacy in this way “Fallacies are common errors in reasoning that will undermine the logic of your argument. Fallacies can be either illegitimate arguments or irrelevant points, and are often identified because they lack evidence that supports their claim.”
I think we may have one here that has pervaded Neonatology across the globe. Imbedded in the fallacy is the notion that because the dark green aspirates look gross and we often see such coloured aspirates in patients with necrotizing enterocolitis or other bowel disease, all green aspirates must be bad for you. The second fallacy is that the darker the aspirate the more seriously you should consider discarding it. This may surprise you but on their own there isn’t much of anything that has been shown to be wrong with them. Looking for evidence to demonstrate increased rates of NEC or other abdominal issues in an otherwise well patient finds pretty much nothing to support discarding.
The main reason for the share of this paper is what is in Table 3.
Although not significantly different the mean estimates for concentration of bile acids in the pale and dark green aspirates came close to being different. Other nutritional content such as fat, protein and carbohydrate were no different. As the bile became darker though the bile acids tended to increase. It is this point that is worthy of discussion.
A Breakdown of the Aspirate
I’m with you. When you look at that murky dark green fluid in the syringe it just seems wrong to put that back into a belly. Would you want to eat that? Absolutely not but when you break it down into what is in there, suddenly it doesn’t seem so bad. We assume that we would not want to refeed such putrid looking material and that is where the logical fallacy exists. What evidence do we have that refeeding that fluid is bad? As I said above not much at all. Looking at the fact that there is actual nutritional calories in that fluid and bile acids as well you come to realize that throwing it away may truly not be in the best interest of the baby. Calories may wind up in the garbage and along with them, bile acids.
Bile acids are quite important in digestion as they help us digest fat and moreover as they enter the ileum they are reabsorbed in large quantities which go to further help digestion. In addition bile acid concentrations are what helps draw fluid into bile and promotes bile flow. By throwing these bile acids out we could see lower bile volumes and possible malabsorption from insufficient emulsification of fat.
The other unmeasured factors in this fluid are the local hormones produced in the bowel such as motilin which helps with small bowel contractility. Loss of this hormone might lead to impairment of peristalsis which can lead to other problems such as bacterial overgrowth and malabsorption.
Now all of this is speculative I will admit and to throw out one dark green aspirate is not going to lead to much harm I would think. What if this was systematic though over 24 or 48 hours that such aspirates were being found and discarded. Might be something there, What I do think the finding of such aspirates should trigger however is a thorough examination of the patient as dark green aspirates can be found in serious conditions such as NEC or bowel perforation. In the presence of a normal examination with or without laboratory investigations what I take from this study is that we should question are tendency to find and discard. Maybe the time has come to replace such fear with a practice of closing our eyes and putting that dark green aspirate right back where it came from.