

I have been mulling over this piece for some time. In my own practice I have long questioned the role for standard phototherapy (the equivalent of a single light source) vs intensive phototherapy (delivering >30 microwatts/cm2/nm and usually two light sources) when treating jaundice for all patients. I have bolded that last part to emphasize that I am not just talking about newborns with severe hyperbilirubinemia but rather all infants with treatable jaundice based on local treatment curves such as shown in the CPS and AAP statements. 
When newborns are only 30 – 50 micromol/L above the treatment threshold as an example, I will see standard phototherapy ordered or after initiating treatment with intensive phototherapy as the level approaches no treatment required you will see people switch to standard phototherapy again. Why is that and does it make sense?
The rationale for using less intensive phototherapy has been to minimize side effects. Historically, these were retinal damage (hence the eye covers), electrolyte disturbances, increased insensible water loss and occasionally rashes. I use the word historically as they for the most part are no longer relevant today provided a narrow spectrum LED light source is utilized which is the technology used in most modern phototherapy light sources now. Backing up this claim, in 2008 Dr. Maisels, showed that in preterm infants receiving LED based light there were no increases in transepidermal water loss. By limiting the wavelength of light emitted to 430 – 490 nm and avoiding the infrared wavelengths. Whether the concern exists with respect to retinal effects is tough to say for sure so continued precautions with eye covers are recommended.
Go Big or Go Home
If there is little harm to phototherapy then is there a reason to use more? The effectiveness of phototherapy is generally based on three things. The first is the proximity of the light source to the patient (< 15 cm is ideal), the second is the intensity of the lamp and the third is the surface area covered. If you are using a single focused spot and covering only 15- 20% of the body you are missing out on a lot of skin that could be helping to lower an infants bilirubin more rapidly. As I see it, if there is little harm in giving phototherapy and the rate of bilirubin decline is faster with better phototherapy, why would you use anything less than intensive using two light sources? Also from a developmental care point of view, less time under the lights means more time for skin to skin and that is always a good thing.
Phototherapy and DNA damage
What prompted me to write this piece actually was the following paper Jaundice, phototherapy and DNA damage in full-term neonates by Ramy N et al from November of 2015. In this paper the authors used a validated measure of DNA damage and assessed infants both before and after phototherapy. Thirty six newborns with jaundice were compared to 30 controls. The results are shown in the following figure.
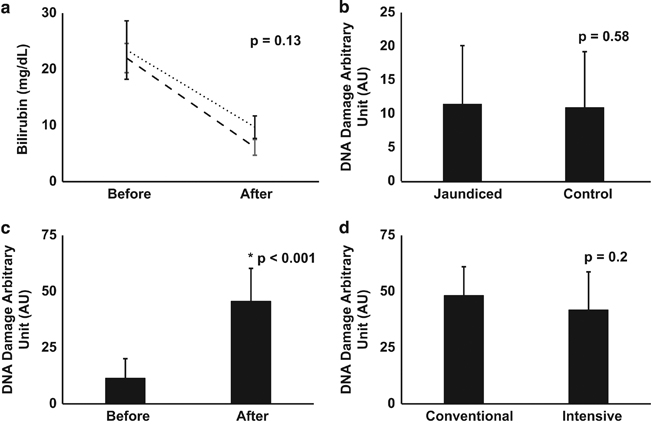
Figure B demonstrates that prior to initiation of phototherapy the extent of DNA damage in tested cells is no different whether you are jaundiced or not. In essence bilirubin is not toxic to cells which also makes sense knowing that bilirubin has antioxidant properties and hence one would think it might be protective against DNA damage. It is figure C and D that provide the most interesting information. Figure C demonstrates that phototherapy (conventional and intensive groups combined) leads to an increase in DNA damage. Figure D is important in that it illustrates that comparing conventional and intensive phototherapy groups there is no difference in rates of DNA damage. This would indicate that more intensive phototherapy is not hazardous to cells.
What was noted in the end though is what is most important here. As expected the duration of phototherapy differed between the two strategies. Infants in the conventional group were under lights for 62.2 ± 23.02 hrs vs 41.3 ± 22.9 hrs, P = 0.005 in the intensive group. When the authors analyzed the relationship between DNA damage and length of phototherapy there was a statistically significant relationship between the two.
In summary then
- Intensive phototherapy is more effective than conventional at reducing levels of jaundice
- Phototherapy is associated with minimal clinical side effects whether intensive or conventional.
- Infants receiving conventional phototherapy require longer courses of treatment.
- Longer courses are associated with greater levels of DNA damage.
- The significance of this DNA damage is unknown based on this study but in principal avoiding such injury may be a wise thing to do.
One last benefit – less needle pokes and shorter lengths of stay!
If an infant spends an average of one less day under phototherapy lights do not underestimate the added benefit with respect to avoiding needle pokes. Typically such infants receive one poke a day to “check how the decline is going”. Shortening the course of phototherapy may translate into one or two less pokes or more and that is definitely a good thing!
Lastly I will leave you with a tip from my own practice which I have found very useful to eliminate at least one poke. When phototherapy is effective and the bilirubin is coming down (and is close to the threshold for stopping but not quite there yet) it is common for people on rounds to order another bilirubin for the morning and continue phototherapy until that result. The result comes back the following morning and the practitioner orders a follow-up bilirubin for the following day to check for the “rebound”.
An alternative strategy is to keep the infant on phototherapy overnight and rather than checking on the bilirubin in the morning just stop the phototherapy on rounds. Eight hours later check the bilirubin and if it is below the threshold for treatment send the infant home. You avoid an overnight stay and instead of poking twice in two days do it all in one.
Whether you take this advice or not is up to you but if all that comes from this post is a decrease in the general fear of intensive phototherapy I may have gotten somewhere and the DNA of many babies out there will thank you!
Thanks for posting this. Having recently completed my training insensible water loss and electrolytes were never a big issue so I always wondered why nurses asked me whether I wanted standard or intensive phototherapy. I was always of the opinion that if the baby needed phototherapy it would be best to get the values down quickly for the reasons you outlined. It is nice to have the historical background for their reasoning and an updated view on current evidence and reasoning.
Another added benefit (especially for full or late pre terms) is the reduced time away from positive breastfeeding behaviors which lead to higher and more successful breastfeeding duration rates. The quicker infants are off phototherapy and discharged home the better it is for establishing breastfeeding.
Besides anti-oxidant properties, bilirubin formation also has pulmonary vasodilatation properties as NO is formed in the process of the bilirubin breakdown. Nice overview!
You mention that increasing the surface area covered increases the effectiveness of phototherapy. I’ve heard that elsewhere, including in the AAP position paper, and it makes no sense. As far as I know, the photochemical reaction is not saturable, in practical terms. Therefore, the relevant variables for amount of bilirubin converted by phototherapy are number of light photons and concentration of the substrate, bilirubin. Giving twice as much phototherapy to a given surface area of skin has exactly the same effect as doubling the amount of skin exposed to the original intensity of phototherapy. Therefore, putting lights on other body parts, such as legs and arms, is far less effective that increasing the intensity to the largest relatively flat body surface available, the torso. It’s basic organic chemistry.
Greg as the bilirubin that is converted is in the tissue and not the blood (although is ultimately carried away through that means) exposing more tissue to the light should lead to more conversion to lumirubin as otherwise you are correct that it is not saturable. If the bilirubin was presented to the light source at a constant rate then surface area would have nothing to do with it. Covering more skin though increases the amount of substrate converted per second though as I see it. While I have a degree in Chemistry with my focus being Organic Chemistry I will have to confess I am not about to get into a debate about that aspect as it has been many years since I thought about such things ????
Cuanto me gustaría que éste material estuviera en español para poder leerlo. Me pueden decir si viene en Español.
Tal vez copiarlo en traductor Google