For almost a decade now confirmation of intubation is to be done using detection of exhaled CO2. The 7th Edition of NRP has the following to say about confirmation of ETT placement “The primary methods of confirming endotracheal tube placement within the trachea are detecting exhaled CO2 and a rapidly rising heart rate.” They further acknowledge that there are two options for determining the presence of CO2 “There are 2 types of CO2 detectors available. Colorimetric devices change color in the presence of CO2. These are the most commonly used devices in the delivery room. Capnographs are electronic monitors that display the CO2 concentration with each breath.” The NRP program stops short of recommending one versus the other. I don’t have access to the costs of the colorimetric detectors but I would imagine they are MUCH cheaper than the equipment and sensors required to perform capnography using the NM3 monitor as an example. The real question though is if capnography is truly better and might change practice and create a safer resuscitation, is it the way to go?
Fast but not fast enough?
So we have a direct comparison to look at. Hunt KA st al published Detection of exhaled carbon dioxide following intubation during resuscitation at delivery this month. They started from the standpoint of knowing from the manufacturer of the Pedicap that it takes a partial pressure of CO2 of 4 mm Hg to begin seeing a colour change from purple to yellow but only when the CO2 reaches 15 mm Hg do you see a consistent colour change with that device. The capnograph from the NM3 monitor on the other hand is quantitative so is able to accurately display when those two thresholds are reached. This allowed the group to compare how long it took to see the first colour change compared to any detection of CO2 and then at the 4 and 15 mm Hg levels to see which is the quicker method of detection. It is an interesting question as what would happen if you were in a resuscitation and the person intubates and swears that they are in but there is no colour change for 5, 10 or 15 seconds or longer? At what point do you pull the ETT? Compare that with a quantitative method in which there is CO2 present but it is lower than 4. Would you leave the tube in and use more pressure (either PIP/PEEP or both?)? Before looking at the results, it will not shock you that ANY CO2 should be detected faster than two thresholds but does it make a difference to your resuscitation?
The Head to Head Comparison
The study was done retrospectively for 64 infants with a confirmed intubation using the NM3 monitor and capnography. Notably the centre did not use a colorimetric detector as a comparison group but rather relied on the manufacturers data indicating the 4 and 15 mm Hg thresholds for colour changes. The mean age of patients intubated was 27 weeks with a range of 23 – 34 weeks. The results I believe show something quite interesting and informative.
Median time secs (range)
Earliest CO2 detection
3.7 (0 – 44s)
4 mm Hg
5.3 (0 – 727)
15 mm Hg
8.1 (0 – 727)
I wouldn’t worry too much about a difference of 1.6 seconds to start getting a colour change but it is the range that has me a little worried. The vast majority of the patients demonstrated a level of 4 or 15 mm Hg within 50 seconds although many were found to take 25-50 seconds. When compared to a highest level of 44 seconds in the first detection of CO2 group it leads one to scratch their head. How many times have you been in a resuscitation and with no CO2 change you keep the ETT in past 25 seconds? Looking closer at the patients, there were 12 patients that took more than 30 seconds to reach a threshold of 4 mm Hg. All but one of the patients had a heart rate in between 60-85. Additionally there was an inverse relationship found between gestational age and time to detection. In other words, the smallest of the babies in the study took the longest to establish the threshold of 4 and 15 mm Hg.
Putting it into context?
What this study tells me is that the most fragile of infants may take the longest time to register a colour change using the colorimetric devices. It may well be that these infants take longer to open up their pulmonary vasculature and deliver CO2 to the alveoli. As well these same infants may take longer to open the lung and exhale the CO2. I suppose I worry that when a resuscitation is not going well and an infant at 25 weeks is bradycardic and being given PPV through an ETT without colour change, are they really not intubated? In our own centre we use capnometry in these infants (looks for a wave form of CO2) which may be the best option if you are looking to avoid purchasing equipment for quantitative CO2 measurements. I do worry though that in places where the colorimetric devices are used for all there will be patients who are extubated due to the thought that they in fact have an esophageal intubation when the truth is they just need time to get the CO2 high enough to register a change in colour.
Anyways, this is food for thought and a chance to look at your own practice and see if it is in need of a tweak…
Skin to skin care or kangaroo care is all the rage and I am the first one to offer my support for it. Questions persist though as to whether from a physiological standpoint, babies are more stable in an isolette in a quiet environment or out in the open on their mother or father’s chests. Bornhorst et al expressed caution in their study Skin-to-skin (kangaroo) care, respiratory control, and thermoregulation. In a surprising finding, babies with an average gestational age of 29 weeks were monitored for a number of physiological parameters and found to have more frequent apnea and higher heart rates than when in an isolette. The study was small though and while there were statistical differences in these parameters they may not have had much clinical significance (1.5 to 2.8 per hour for apnea, bradycardia or desaturation events). Furthermore, does an increase in such events translate into any changes in cerebral oxygenation that might in turn have implications for later development? Tough to say based on a study of this magnitude but it certainly does raise some eyebrows.
What if we could look at cerebral oxygenation?
As you might have guessed, that is exactly what has been done by Lorenz L et al in their recent paper Cerebral oxygenation during skin-to-skin care in preterm infants not receiving respiratory support.The goal of this study was to look at 40 preterm infants without any respiratory distress and determine whether cerebral oxygenation (rStO2)was better in their isolette or in skin to skin care (SSC). They allowed each infant to serve as their own control by have three 90 minute periods each including the first thirty minutes as a washout period. Each infant started their monitoring in the isolette then went to SSC then back to the isolette. The primary outcome the power calculation was based on was the difference in rStO2 between SSC and in the isolette. Secondary measures looked at such outcomes as HR, O2 sat, active and quiet sleep percentages, bradycardic events as lastly periods of cerebral hypoxia or hyperoxia. Normal cerebral oxygenation was defined as being between 55 to 85%.
Surprising results?
Perhaps its the start of a trend but again the results were a bit surprising showing a better rStO2 when in the isolette (−1.3 (−2.2 to −0.4)%, p<0.01). Other results are summarized in the table below:
Mean difference in outcomes
Variable
SSC
Isolette
Difference in mean
p
rStO2
73.6
74.8
-1.3
<0.01
SpO2 (median)
97
97
-1.1
0.02
HR
161
156
5
<0.01
% time in quiet sleep
58.6
34.6
24
<0.01
No differences were seen in bradycardic events, apnea, cerebral hypoexmia or hyperoxemia. The authors found that SSC periods in fact failed the “non-inferiority” testing indicating that from a rStO2 standpoint, babies were more stable when not doing SSC! Taking a closer look though one could argue that even if this is true does it really matter? What is the impact on a growing preterm infant if their cerebral oxygenation is 1.3 percentage points on average lower during SSC or if their HR is 5 beats per minute faster? I can’t help but think that this is an example of statistical significance without clinical significance. Nonetheless, if there isn’t a superiority of these parameters it does leave one asking “should we keep at it?”
Benefits of skin to skin care
Important outcomes such as reductions in mortality and improved breastfeeding rates cannot be ignored or the positive effects on family bonding that ensue. Some will argue though that the impacts on mortality certainly may be relevant in developing countries where resources are scarce but would we see the same benefits in developed nations. The authors did find a difference though in this study that I think benefits developing preterm infants across the board no matter which country you are in. That benefit is that of Quiet Sleep (QS). As preterm infants develop they tend to spend more time in QS compared to active sleep (AS). From Doussard- Roossevelt J, “Quiet sleep consists of periods of quiescence with regular respiration and heart rate, and synchronous EEG patterns. Active sleep consists of periods of movement with irregular respiration and heart rate, and desynchronous EEG patterns.” In the above table one sees that the percentage of time in QS was significantly increased compared to AS when in SSC. This is important as neurodevelopment is thought to advance during periods of QS as preterm infants age.
There may be little difference favouring less oxygen extraction during isolette times but maybe that isn’t such a good thing? Could it be that the small statistical difference in oxygen extraction is because the brain is more active in laying down tracks and making connections? Totally speculative on my part but all that extra quiet sleep has got to be good for something.
To answer the question of this post in the title I think the answer is a resounding yes for the more stable infant. What we don’t know at the moment except from anecdotal reports of babies doing better in SSC when really sick is whether on average critically ill babies will be better off in SSC. I suspect the answer is that some will and some won’t. While we like to keep things simple and have a one size fits all answer for most of our questions in the NICU, this one may not be so simple. For now I think we keep promoting SSC for even our sick patients but need to be honest with ourselves and when a patient just isn’t ready for the handling admit it and try again when more stable. For the more stable patient though I think giving more time for neurons to find other neurons and make new connections is a good thing to pursue!
I don’t envy our nurses who care for babies withdrawing from various opiates and other substances. These assignments are definitely a challenge and require a great deal of patience and depending on the shrillness of an infant’s cry a good set of earplugs. Nonetheless we do our best with these infants to keep them calm and avoid as much stimulation as we can as we attempt to minimize the excitability of their nervous system.
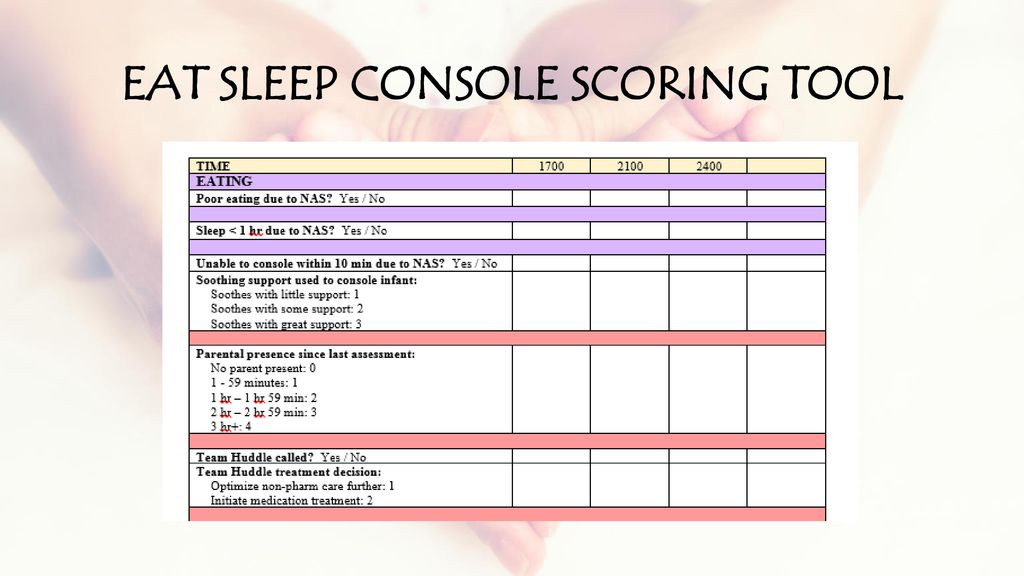
Over 40 years ago the Finnegan Neonatal Abstinence scoring system was developed to assist medical teams by providing as objective a system as possible to compare one infant to another and determine when and if a patient should be treated pharmacologically. Unfortunately there is a problem inherent with this scoring system. It is the same problem that exists when you don’t have a blinded research trial. Imagine you are caring for an infant and you were given no history about drug exposure. How might you score a patient like that compared to one in which you are told has been exposed to illicit substances? Your senses are heightened and moreover if you were told this baby is “withdrawing terribly” or “is awful at night” you are biased. How are you likely to score such a patient when they are “on the edge” of being counted as a 1 or a 0 in a category? I bet in many cases, especially if you haven’t taken care of many such patients you err on the side of caution and score them on the high side. It is human nature. When the possible outcome of failing to recognize a withdrawing patient is a seizure, no one wants to be on when it happens having their scoring questioned. Have a look at the scoring tool though.
There is a lot of stuff in there to check off! What if it could be simpler?
The ESC Tool
In early May, news began to break of an abstract being presented at the Pediatric Academic Society meeting. The news story from the AAP can be found here. The ESC tool is a three question tool used to assess whether an infant requires treatment for withdrawal.
E – Eat (is an infant is able to eat 1 or more ounce per feeding)
S – Sleeping (sleep for an hour or longer undisturbed)
C – Console (Be consoled in 10 minutes or less.)
If all three criteria are met, the patient does not need treatment. If one or more criteria are not met the housestaff are notified and first non-pharmacologic and then pharmacologic means are employed if necessary to control symptoms.
The authors did something quite interesting. They looked at 50 patients with 201 hospital days with prenatal exposures to opiates and applied the ESC criteria to guide treatment. Concurrently they captured the Finnegan scores but did not use them to guide treatment.
The findings I hope you will agree are quite interesting!
“FNASS scores indicated starting morphine in 30 infants (60%). Morphine was actually started on only 6 patients (12%) (p< 0.0001) based on the ESC approach. The FNASS led protocol directed initiating or increasing meds on 24.6% of days compared to 2.7% of days using the ESC approach (p< 0.0001). The FNASS approach directed that morphine was either not started or decreased on 65.8% of days compared with 94.4% of days using the ESC approach (p< 0.0001). There were no readmissions or reported adverse events.
Pretty amazing but…
The ESC approach greatly reduced the need for treatment and as the authors state there were no readmissions or reported adverse events. What we don’t know and will be needed I suspect before anyone will adopt this strategy (which I have to say again is so much simpler that current approaches) is how these children do in the long run. If the system is undertreating withdrawal, could we see downstream impacts of a “kinder and gentler” approach? One outcome that will be reported soon in the next month is length of stay. I am eagerly awaiting further results as I for one think that a simpler approach to these patients may be just what the doctor ordered. I think the nurses might thank us as well but we will see just how appropriate it is!
The Abstract reporting these findings can be found below
If there is one thing that keeps coming back as a lesson again and again in life it is the importance of communication. Whether it be in the home or at work, too many of our “problems” in the workplace come down to whether or not our teams talk to one another effectively.
A tremendous source of stress of course is the unknown. When a baby is born in the field we can only rely on the information being presented to us via telephone contact. In the melee that occurs on arrival of a potentially sick patient, details can be missed.
The following video illustrates such a situation and I believe aptly provides a good example of how to communicate in such a way that the stress of the situation is relieved. If we can all strive to slow things down just a little we may find that communication eliminates much of the tension in such a situation.
If you are looking to “slow” down your life and improve things such as communication style you may want to have a look at the book “In Praise of Slow” as we head into the weekend. It’s all about slowing things down to actually improve efficiency. The world is moving pretty quickly these days and couldn’t we all do with a little more efficiency and less wasted time? In Neonatology we are confronted with surprises every day, often with little notice. If we can slow things down and pass on the needed information to the right people at the right time we will help to reduce errors if we can just get it right the first time!
As you can tell I am a big fan of simulation in helping to create high functioning teams! More of these videos can be accessed on my Youtube channel at
I have often said that if this came to pass as a mandatory requirement that I would make an announcement shortly thereafter that I was moving on to another career. I think people thought I was kidding but I can put in writing for all to see that I am serious! The subject has been discussed for some time as I can recall such talks with colleagues both in my current position and in other centres. The gist of the argument for staying in-house is that continuity is improved over that period and efficiency gained by avoiding handovers twice a day . How many times have you heard at signover that extubation will be considered for the following morning or to keep the status quo for another issue such as feeding until the next day. No doubt this is influenced by a new set of eyes being in the unit and a change in approach to being one of “putting out fires” overnight. The question then is whether having one Neonatologist there for 24 hours leads to better consistency and with it better outcomes. With respect to PICUs the AAP has previously recommended that 24 hour in-house coverage by an intensivist be the standard so should Neonatology follow suit?
A Tale of Two Periods
My friends in Calgary, Alberta underwent a change in practice in 2001 in which they transitioned from having an in-house model of Neonatologist coverage for 24 hours a day to one similar to our own centres where the Neonatologist after handover late afternoon could take call from home. An article hot off the presses entitled Twenty-Four hour in-house neonatologist coverage and long-term neurodevelopmental outcomes of preterm infants seeks to help answer this question. The team undertook a retrospective analysis of 387 infants born at < 28 weeks gestational age during the periods of 1998-2000 (24 hour period, N=179 infants) vs 2002 – 2004 (day coverage, N= 208 infants) with the goal of looking at the big picture being follow-up for developmental outcome at 3 years. This is an important outcome as one can look at lots of short term outcomes (which they also did) but in the end what matters most is whether the infants survive and if they do are they any different in the long term.
As with any such study it is important to look at whether the infants in the two periods are comparable in terms of risk factors for adverse outcome. Some differences do exist that are worth noting.
Increased risk factors in the 24 hour group
Chorioamnionitis
Maternal smoking
Smaller birthweight (875 vs 922 g)
Confirmed sepsis (23% vs 14%)
Postnatal steroids (45% vs 8%) – but duration of ventilation longer in the day coverage group likely due to less postnatal steroids ( 31 vs 21 days)
All of these factors would predict a worse outcome for these infants but in the end for the primary outcome of neurodevelopmental impairment there was no difference. Even after controlling for postnatal steroids, birth weight, sex and 5 minute apgar score there was still no difference.
What might this mean?
Looking at this with a glass is half full view one might say that with all of the factors above predicting worse outcome for infants, the fact that the groups are not different in outcome may mean that the 24 hour model does indeed confer a benefit. Maybe having a Neonatologist around the clock means that care is made that much better to offset the effect of these other risk factors? On the other hand another explanation could also be that the reason there is no difference is that the sample just isn’t big enough to show a difference. In other words the size of the study might be underpowered to find a difference in developmental outcome.
One of the conclusions in this study is that the presence of a Neonatologist around the clock may have led to earlier extubation and account for the nearly 10 day difference in duration of ventilation. While I would love to believe that for personal reasons I don’t think we can ignore the fact that in the earlier epoch almost 50% of the babies received postnatal steroids compared to 8% in the later period. Postnatal steroids work and they do so by helping us get babies off ventilators. It is hard to ignore that point although I woudl like to take credit for such an achievement.
For now it would appear that I don’t feel compelled to stay overnight in the hospital unless it is necessary due to patient condition necessitating me having my eye on the patient. I am not sure where our field will go in the future but for now I don’t see the evidence being there for a change in practice. With that I will retire to my bedroom while I am on call and get some rest (I hope).




 If you are looking to “slow” down your life and improve things such as communication style you may want to have a look at the book “In Praise of Slow” as we head into the weekend. It’s all about slowing things down to actually improve efficiency. The world is moving pretty quickly these days and couldn’t we all do with a little more efficiency and less wasted time? In Neonatology we are confronted with surprises every day, often with little notice. If we can slow things down and pass on the needed information to the right people at the right time we will help to reduce errors if we can just get it right the first time!
If you are looking to “slow” down your life and improve things such as communication style you may want to have a look at the book “In Praise of Slow” as we head into the weekend. It’s all about slowing things down to actually improve efficiency. The world is moving pretty quickly these days and couldn’t we all do with a little more efficiency and less wasted time? In Neonatology we are confronted with surprises every day, often with little notice. If we can slow things down and pass on the needed information to the right people at the right time we will help to reduce errors if we can just get it right the first time!