I often catch myself saying that Neonatology being a relatively young speciality has so much more to discover. Any Pediatric resident can attest to this when they scan their journals and see so many articles exploring uncharted territory. As we continue to march forward it gave me pause to realize that we had lost someone in August who quite literally put the intensive in Neonatal Intensive Care.
Dr. Forrest Bird was an inventor and a pilot who was inspired to create a device to deliver oxygen to pilots flying at high altitude. This was needed due to the inability of the allied airforce to fly as high as the German planes. He was able to reverse engineer of sorts a solution to the lack of oxygen the airforce experienced and thereby level the playing field. This technology became the backbone behind the Bird Respirator first produced in 1950. This device is considered to be the dawn of the ventilator and was soon to put the iron lung out of business.
In 1963, following the death of John F. Kennedy’s son Patrick at 34 weeks from RDS research in the field of Neonatology blossomed bringing something positive out of tragedy. Funding for research in the area uncovered the cause of RDS as surfactant deficiency by Dr. Avery and a great number of papers followed exploring the concepts of surface tension, atelectasis and the effects of pressure on expansion of the newborn lung. While I clearly was not working in the field back then I have no doubt the clear need for a device to help these newborns with collapsable lungs inspired Dr. Bird to search for a solution. In 1970 he produced the Baby Bird Ventilator which was essentially a smaller version of the original. Up until this point, there was little that could be done for such preemies and other children in respiratory failure. By some accounts the ability to ventilate a newborn with positive pressure led to a reduction in mortality from 70% to 10% due to respiratory distress.
How Big An Impact Did It Have?
According to the World Health Organization approximately 15 Million babies are born before 37 weeks each year in the world. In the US alone about 1 in 9 babies are born at these gestational ages which translates to about 450000 babies per year. If we take a conservative estimate that 50% will have some degree of respiratory distress and need ventilation or CPAP that translates into 7.5 million babies every year helped by technology that Dr. Bird brought into this world. While true that the Baby Bird would be replaced by more advanced technology as years passed and ventilators of today bear little resemblance to the original design, every device owes a nod to the its ancestor the Baby Bird.
It has been 45 years since the Baby Bird came to market and there are few people working in the field today who would remember using this particular ventilator. Its inventor both directly and indirectly is responsible for saving the lives of millions of babies over a 45 year span. How many of us working in the field today can say that we know someone who has made such an impact in recent memory. Dr. Bird was a hero in Medicine and in particular Neonatology and for that reason in received the National Medal of Technology and Innovation from President Obama in 2009.
I hope that this piece helps to educate even a few people about this modern day hero. It also serves to remind me as we begin to lose the pioneers in our field that perhaps we aren’t such an young specialty anymore after all.
There is no question that adequate weight gain is a necessity in the NICU. We commonly strive for 15-20 g/kg/d in our centre but sadly our smallest infants often struggle to achieve such increases in mass. If you have worked with me you will often hear me state that after the acute issues are dealt with in a ELBW infant the most important thing we need to focus on is nutrition if we want to help these infants come off respiratory support. They simply need stronger bones, more muscle mass and adequate well balanced nutrition to heal some of the damage that unfortunately occurs while they are receiving positive pressure ventilation.
Does weight gain right after birth matter?
In the past few years however several papers have challenged this belief of mine in suggesting that the time shortly after birth is equally important in particular with reference to retinopathy of prematurity. Associations between poor weight gain in the first 2-6 weeks of age and worse ROP have been noted. The challenge as always with such retrospective or even prospective studies is the presence of confounders. Does the finding of worse ROP indicate that the lack of weight gain is in fact causative or is it reflective of other factors at work? When we are looking at retrospective studies the authors typically will try and control for such known factors but there may be other factors that have been unaccounted for. In particular, is the lack of weight gain attributable to a unit that pays poor attention to nutrition or a result of inflammatory states such as sepsis causing a catabolic rather than anabolic state in the child? Add to this that lipoprotein lipase tends to become less active in the presence of such inflammation and a rising triglyceride level will often dictate that lipids be reduced or stopped altogether further compromising nutrition.
The Evidence
A Swedish paper by Stoltz Sjöström et al published in 2015 examined 498 infants born between 22 0/7 – 26 6/7 weeks of age and sought to determine if poor weight gain and energy intake were responsible for increased rates of ROP in NICUs in Sweden. This retrospective study included infants with an overall rate of Grade III-V ROP of 34.5%. When looking at the differences in a number of variables including weight gain and energy intake in the first four weeks of life there appears to be a cutoff of 100 Kcal/kg/d as an average intake that predicts the risk of ROP. That is if the caloric intake on average over four weeks is less than 100 Kcal/kg/d then the risk of severe ROP increases. When controlling for all variables none of the constituents of nutrition appeared to be significant (protein, fat, carbohydrate) but rather the energy intake. Importantly two additional factors that bore out significance were prolonged ventilation and number of blood transfusions.
While this was a fairly good sized study there are a number of confounders here that again raise the question of what truly is causing the higher rate of ROP. ROP is known to be affected by oxygen use. The current state of thinking is that higher oxygen saturations (Support trial) as well as wide swings in oxygenation may predispose to worse ROP. Given that two important factors increasing the risk of severe ROP in this cohort were prolonged ventilation and need for blood increased numbers of blood transfusions these may well be a proxy for labile oxygenation. I can’t resist the speculation additionally that the lower energy intake may have delayed the building of adequate muscle and bony framework to assist these infants in coming off the ventilator. Sicker infants need more transfusions as well as the bone marrow takes on a quiescent state. It may well be that lower energy intakes are associated with worse ROP but as with other papers looking at this factor it may not be causative (at least directly).
The other thing to bear in mind is that this study is a retrospective analysis of a study originally published in 2009 called the Express Study. Much has changed in the realm of Neonatal Nutrition. When maternal breast milk is unavailable many units have access to donor milk. Early and more aggressive TPN has become the norm since that time with many infants receiving a starter solution on day 1 and TPN late on day 1 or certainly on day 2. Lastly, many centres are now changing from what had been the standard soy based lipid emulsion to one such as SMOF that contains omega-3 fatty acids with inherent anti-inflammatory effects. Given all these changes it would be interesting to see if many infants these days are receiving such low caloric delivery and even if so if their rates of severe ROP are indeed higher.
Conclusion
My take on this therefore is that while we should all strive for better nutrition in our infants I do not believe that the evidence is there yet that an average caloric delivery in the first 4 weeks of age of less than 100 Kcal/kg/d is causing worse ROP in our infants. We will never have a randomized controlled trial to determine such a causative relationship so these sorts of studies are the best we can do. Fortunately, even if there were a cause and effect relationship we are already striving to keep our goal calories above the threshold which seems to be associated with worse outcome.
In essence let’s all keep our eye on the energy being provided and with time all should be well provided we continue to be extremely vigilant with minimizing oxygen exposure in these vulnerable infants.
* I would like to thank Jennifer Degl for providing permission to use her photo for this post. She is the author of From Hope to Joy and does great work which can be found at: www.micropreemie.net
A publication this past week has been featured in multiple news stories across North America due to it’s impact on mortality and morbidity in the NICU. Shielding Parenteral Nutrition From Light Improves Survival Rate in Premature Infants: A Meta Analysis made the splash that it did because it’s premise is so simple yet has such an impact. In essence, protect TPN from light (including phototherapy) and you can cut mortality in the NICU in half!
A Canadian Research Story
The CBC has covered this as well with the following piece that also indicates that a survey of NICUs from 4 years ago indicated about half of hospitals did not employ such shielding. In fairness the meta-analysis has just been published which combined 4 studies and about 800 patients to yield these findings but the understanding that such practice could benefit newborns in NICU has been known for many years. What makes this story even more interesting to me is it’s Canadian origin in that Dr. Chessex performed much of the work in this field and his dedication to the area of oxidative stress in large part led to this finding.
In fact in 1999 he published the following paper Protecting solutions of parenteral nutrition from peroxidation which demonstrated that simply covering the bag of TPN was not enough to prevent oxidation from occurring. The whole set up including the bag, lines and during the preparation of TPN needed to be shielded or peroxide concentrations increased by 1.5 -2 times compared to when a clear set up was used. Furthermore phototherapy led to a further rise in the concentration of these oxidative harmful molecules. Ironically it is the necessary components of TPN including riboflavin and lipid that create the environment for light to create these oxidative products that can damage tissue.
You may ask yourself at this point why something that was known nearly 17 years ago did not lead to widespread adoption by NICUs across Canada and perhaps North America. For one, medicine is notoriously slow to change practice especially when there is an effort and cost that will need to be considered. Sourcing such materials is actually more difficult than it may seem as we learned locally two years ago when one of our hospitals began this change. Secondly, Neonatology is littered with bench research that while striking in its findings simply did not translate into a clinically relevant outcome. For example we know that phenobarbital increases the conjugation of bilirubin in the liver and therefore in theory should be a great adjunctive treatment to phototherapy for the usual newborn jaundice but that didn’t pan out in human trials. What is the story here though?
The Landmark Study Results That Made Headlines
The meta-analysis mentioned in the start of this piece and causing all this attention included four studies that examined possible reductions in mortality. In 2007 Chessex studied the effect of light protection (LP) on the incidence of BPD finding a 30% reduction in those infants in a randomized study of LP vs none. This finding alone should be enough to raise some eyebrows and it did as many centres were adopting LP around this time. The second study done in Egypt in 2009 demonstrated a similar finding in reduced BPD rates. The third study was by Chessex again in 2009 and once more demonstrated reductions in oxidant stress and BPD. Curiously the largest of the studies based out of France with 587 patients in 2014 randomized to LP or none found no difference in BPD or death but the latter was very close to meeting statistical significance. In all of these studies no difference in mortality was noted however when they were combined and examined as a group the following was identified. Herein lies the power so to speak of the meta-analysis. Small studies may not demonstrate a difference that reaches significance in the desired outcome of interest but if several studies that have very similar measurements are pooled together the power to find a difference may emerge. That would seem to be the case here in that not only is there a halving of mortality that reaches statistical significance but a specific disadvantage for males was uncovered in that they had a two fold risk compared to females of dying if their TPN was uncovered.
Are These Results Relevant to Modern Practice
The results of this study are profound in terms of the impact that they could have on both BPD and mortality in our NICUs. One caveat needs to be mentioned however and that is the utlilization of oxygen in the NICU now and during the time of these studies. Since the time periods that these studies were undertaken, the use of oxygen for many units including our own has become more tightly regulated. As per NRP guidelines we resuscitate our newborns with room air and use every effort at the bedside to avoid wide swings of FiO2 when addressing an episode of desaturation. Furthermore, antenatal steroids, surfactant, liberal use of CPAP have all led to marked reductions in need for FiO2 such that the days of infants being on 30% FiO2 by nasal prongs have been replaced by room air on CPAP for the most part (at least in our units). What would these results be now if these studies were repeated? My suspicion is not as dramatic but there is no question that for at least 17 years we have known about the risk of such oxidative stress.
Is there any logic behind waiting for more evidence in a modern cohort before implementing a strategy of protecting these solutions from light? I don’t think so and hope that the rest of our community agrees and does not wait many more years to implement such precautions. How many other conditions such as ROP could be affected by simply protecting these solutions from light? Quite frankly I don’t need to know. The time has come for change.
Thank you Dr. Chessex for your dedication in bringing this translational research from the bench to the bedside.
Since that post, an incredible shift has occurred in the way that we as a team view attempts at resuscitation at 23 weeks. It took a great deal of dialogue among all health care providers and a deeper understanding of concerns of both Obstetrical and Neonatal colleagues to come to a mutual understanding that could yield a path to move forward. Through dialogue, the damage that had been done by the development of a “broken telephone” was repaired and trust emerged across disciplines which was the only way forward from the beginning.
Why not 22 weeks?
Yes, gestational age is so much more than just a number and must include estimates of fetal size, certainty of dates, parental wishes and several other factors to arrive at a decision that incorporates the wishes of the family. There are certainly significant challenges to informing families during a time of incredible stress as to the options that lay before them but we have to do our best in the time that we have.
When you are crossing that barrier of 24 weeks gestation, despite the caution above about the uncertainty surrounding gestational age dating there is a significant mental leap to move to 23 weeks. The leap to consider 22 weeks is even larger and I would suggest several fold. Is it possible that we would resuscitate such an infant? Absolutely if the dating was uncertain, the family had strong wishes and the team was on board with such a decision but for now this will not be advocated for at all in our city. I suspect similar discussions are happening all over North America and it will be fascinating to see where we land in 5, 10 and more years into the future.
What was the most important change to practice to enable progress?
Prior to 2015 we had one survivor at 23 weeks in a five year period. This year out of five actively resuscitated 3 have survived and at early assessments seem to be doing well. The overwhelming consensus was that skin care needed to be of paramount importance in this process. To that end we began a new process for cleaning the umbilical cord for line insertion with the goal to minimize skin burns on the abdomen. I am proud to report that since we change our technique there have been no skin burns found where once this was commonplace.
The process can be found in this short video here.
For now though, we are about to embark on a new journey in our city and I look forward to the continued collaboration with Obstetricians, Ethicists and all members of the Neonatal team as we explore this new frontier together.
I thought you may find it useful to see how this journey began and where we think it may go by watching this video of myself, Dr. Craig Burym (Obstetrics) and Dr. Aviva Goldberg (Ethics) presenting the approach to resuscitation at 23 weeks from the Neonatal, Obstetrical and Ethical standpoints. The video is about 50 minutes in length but truly addresses issues from multiple vantage points so if you missed it or are interested in how these issues were dealt with please have a look.
(If you are watching this on an Apple computer please use Safari to view)
Living in Canada we are privileged to have a universal health care system. Privileged in the sense that all citizens are entitled to the same level of care regardless of economic circumstance although the monetary costs to the tax payer is another story and forms the basis of most arguments in the US against adopting such a system down south. My goal of this post though is not to enter into a debate about which system is superior but rather speak of the dollars and cents attributable to being born too early or too small.
In the US such measurements are simpler as costs are more easily measured in a private health care system but each health care region in Canada can measure to a certain degree the costs associated with a hospital stay. Certainly the story of Raquena Thomas made this clear to me. In 2007 she was born in Edmonton after her mother left Jamaica for a visit with family in Edmonton. After delivering she was found to have hypoplastic left heart syndrome (HLHS) and went on to have the first stage of the Norwood procedure. What followed was a bill to the mother for $162576 and for commentary on the discussion that ensued about who should pay the bill see the article here. As I was working at the Stollery Children’s Hospital at the time and cared for this infant it was clear to me after this experience that the hospital indeed has a clear method to calculate costs even if we the taxpayer are blind to such calculations.
Now HLHS is a condition that affects very few infants a year in any given province but what about low birth weight and preterm birth? This as we say in Neonatology is our bread and butter. In 2009 Lim et al published data on the Canadian population in attempt to ascertain the health care costs for these groups of patients (CIHI survey: Hospital costs for preterm and small-for-gestational age babies in Canada)
In this period 1 in 7 babies was born either preterm or small for gestational age. If specifically looking at infants < 2500g defined as low birth weight this represented 6% of all babies born. When you factor in that there were 350000 babies born in that year in Canada we are looking at about 21000 babies nationally. Looking at the costs for these infants one sees a direct relationship between decreasing birth weight and increasing costs in the hospital. This should not be surprising to anyone. It should be noted though that the paper provides average costs only without standard deviation or ranges. As you would expect, the costs for a patient with severe HIE or NEC would be higher than the 26 week infant who has a very smooth course and does not have a symptomatic PDA, severe IVH or any other significant disability during their course.
The data looking at such costs is scare with respect to the Canadian landscape and even more difficult to determine has been lifetime costs or at least incremental costs after leaving the hospital environment. I was delighted to see that former colleagues of mine in Edmonton have published a new paper examining both the extent of health service utilization (HSU) attributable costs in the year following discharge of both LBW and normal birth weight peers in Alberta (abstract here). Not surprisingly, smaller babies have more medical needs. In this study LBW patients had an average of 5.9 outpatient services and 1.1 visits to the ER in the first year of life compared to 2 and 0.9 in the normal birth weight peers. Physician services were double with 22.7 office visits compared to 11.9 in the NBW group. The costs to the Health Care system overall are represented in the table below which demonstrates that the LBW infants make up 37% of the total health care costs of newborns yet represent only 6% of the population. In terms of risk factors for LBW they were high prepregnancy weight, aboriginal women and low socioeconomic status. Efforts to lessen the incidence of the first and third factor in our pregnant population would be a good target for public health efforts. Bear in mind that the costs outlined below are in addition to the costs in the hospital.
BW Category
Cost per patient
Patients
Cost to System (millions)
NBW
$3,942
43207
182
LBW <2500
$33,096
3123
108
1500 – 2499g (MLBW)
$20,467
2571
53
1000 – 1499g (VLBW)
$83,895
278
23
< 1000g (ELBW)
$117,546
274
32
The analysis provided in this paper does not specify out the costs by certain conditions such as NEC or BPD so all we have to go on are averages for HSU and cost. It does however raise a point which I believe is crucial to any discussions with respect to expanding programs within the hospital. We need to refocus administration at both the hospital level and at the funding source (our provincial governments) as to the true costs of the conditions that we are trying to prevent. It is only through looking at the costs of both the hospitalization and after discharge that we can truly come to understand the cost effectiveness of expanded programs or new treatment modalities.
Donor breast milk is one that I believe serves as a good example of a program that is in need of expansion in many places in the country but is hampered by the perception of high up front costs. The average cost of this milk is about $4 per ounce. I will simplify the math a little as there would be a phase of escalating the volume per day and a wean at the end but let’s say we have a 1.5 kg infant that we want to treat with DBM for a period of 4 weeks. The cost to do this assuming a TFI of 150 mL/kg/d would be a little over $800 per patient so with the increasing phase, wean and adjusting for some weight gain let’s say $1000 per patient. If there were 200 such patients in your hospital each year the annual cost would be $200000 which on the surface seems like a lot of money. From the most recent cochrane review though comparing formula to donor milk the risk ratio to develop NEC is 2.77 meaning that a preterm baby who receives formula is nearly three times as likely to develop NEC. Ignoring differing rates of NEC by hospital let’s just use the concept that we could prevent one case of NEC a year with such a strategy. The cost of medical NEC is somewhere between 100-140K while surgical is 200 – 240K. The in-hospital costs of preventing just one case nearly pay for or exceed the cost of the entire years supply of DBM. If you add to this the cost of the following years of physician visits, consultants, testing, special diets and investigations and procedures these patients receive the costs are more than covered from just one patient.
Health care budgets are no doubt a difficult thing to balance but the point of all of this is that when determining whether to spend our precious health care dollars we must look at not only the impact during the hospitalization but for years after if we truly modify future risks as well.


 In 1970 he produced the Baby Bird Ventilator which was essentially a smaller version of the original. Up until this point, there was little that could be done for such preemies and other children in respiratory failure. By some accounts the ability to ventilate a newborn with positive pressure led to a reduction in mortality from 70% to 10% due to respiratory distress.
In 1970 he produced the Baby Bird Ventilator which was essentially a smaller version of the original. Up until this point, there was little that could be done for such preemies and other children in respiratory failure. By some accounts the ability to ventilate a newborn with positive pressure led to a reduction in mortality from 70% to 10% due to respiratory distress.

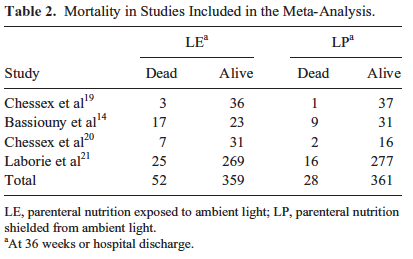 Herein lies the power so to speak of the meta-analysis. Small studies may not demonstrate a difference that reaches significance in the desired outcome of interest but if several studies that have very similar measurements are pooled together the power to find a difference may emerge. That would seem to be the case here in that not only is there a halving of mortality that reaches statistical significance but a specific disadvantage for males was uncovered in that they had a two fold risk compared to females of dying if their TPN was uncovered.
Herein lies the power so to speak of the meta-analysis. Small studies may not demonstrate a difference that reaches significance in the desired outcome of interest but if several studies that have very similar measurements are pooled together the power to find a difference may emerge. That would seem to be the case here in that not only is there a halving of mortality that reaches statistical significance but a specific disadvantage for males was uncovered in that they had a two fold risk compared to females of dying if their TPN was uncovered.


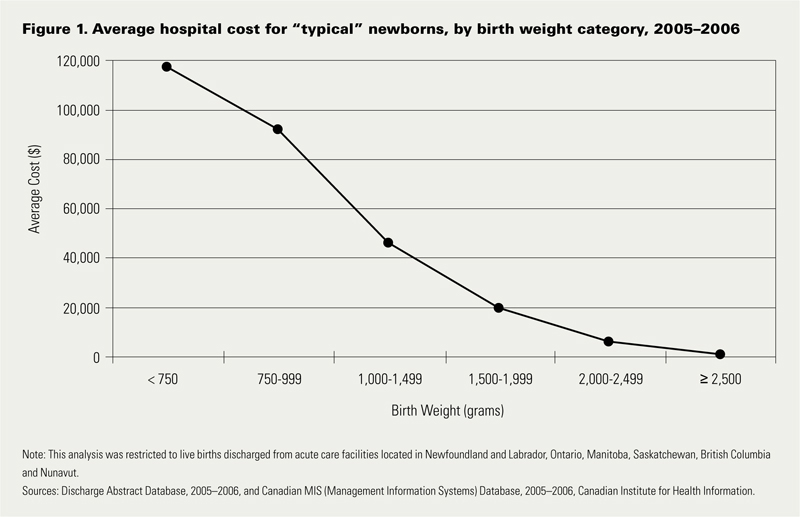 Looking at the costs for these infants one sees a direct relationship between decreasing birth weight and increasing costs in the hospital. This should not be surprising to anyone. It should be noted though that the paper provides average costs only without standard deviation or ranges. As you would expect, the costs for a patient with severe HIE or NEC would be higher than the 26 week infant who has a very smooth course and does not have a symptomatic PDA, severe IVH or any other significant disability during their course.
Looking at the costs for these infants one sees a direct relationship between decreasing birth weight and increasing costs in the hospital. This should not be surprising to anyone. It should be noted though that the paper provides average costs only without standard deviation or ranges. As you would expect, the costs for a patient with severe HIE or NEC would be higher than the 26 week infant who has a very smooth course and does not have a symptomatic PDA, severe IVH or any other significant disability during their course.