A debate broke out recently at one of our rounds when someone asked whether a recent case of NEC was possibly related to a transfusion that a baby received. Much has been written about Transfusion Associated Necrotizing Enterocolitis (TANEC) with the pendulum swinging back and forth between it existing as a real entity or simply being an association that is not causative in the least. Using one of my favourite sources, a retrospective analysis of the Canadian Neonatal Network database found no difference in mortality or morbidities for those who had a transfusion and NEC vs those without. Despite this we continue to see those who “hold feeds” for a few hours prior to transfusion and then resume them a few hours later. Why does this happen?
Risk vs Benefit
Those who hold feeds argue that in Neonatology we hold feeds for far less. Furthermore, what is the harm? If a baby develops NEC within 24 hours of a transfusion and we held the feeds we feel we have done all we could. If a baby is fed and develops NEC we are left asking “what if?”. The purists out there would argue the contrary though, that the evidence is not strong enough to support the practice and may require the insertion of an IV which is a painful procedure and places the infant at risk of infection from one or more skin breaks. Additionally, does the interruption of feeds potentially alter the microbiome of the patient and with it risk potential downstream consequences. In case you are wondering, I have tended to sit on the side of holding a feed although more often when I am asked about it than ordering it upfront. The fact is I just don’t know. The evidence has never been solid in this regard but it is hard to ignore the possibility when you have been bitten once or twice before (whether it was causative or not!). I doubt it really exists but then again what if there is something there?
It May Not Be The Transfusion But Anemia Itself
A recent paper Association of Red Blood Cell Transfusion, Anemia, and Necrotizing Enterocolitis in Very Low-Birth-Weight Infants may have found a possible explanation to the ongoing debate. Research papers associating transfusions with NEC may all have one thing in common in that they have not been able to prove causation. When you have many papers finding the same thing it leads medical teams to begin to believe there is causation. Something else may be at play at this paper suggests another association which again may not be causative but at least in my mind is perhaps biologically plausible. It may be that those patients who are transfused when their hemoglobin is below a threshold of 80 g/L are at increased risk of developing NEC rather than all patients transfused.
This study was a secondary analysis of a prospective study on transfusion transmission of cytomegalovirus in preterm infants < 1500g. The authors chose 80 g/L as a cutoff based on previous studies suggesting this threshold as an important one for transfusion practices. Forty eight out of 60 eligible infants developed NEC and it is from this 48 that multivariable analysis sought to identify factors predisposing to the outcome in question of NEC. The factor with the greatest hazard risk for NEC was severe anemia in a given week with an approximate 6 fold risk (range 2 – 18) while receiving an RBC transfusion in a given week of life did not meet statistical significance.
What does this mean?
Before embracing the result and concluding we have the answer we have to acknowledge the authors have gone on a fishing expedition of sorts. Any secondary analysis of a study that is done carries with it some words of warning. There may be variables that were not controlled for that are affecting the results. As well when looking at many many variables it could be by chance that something or several things come up by chance. Lastly it may be that again there is nothing more than an association here at play. Having said that, there is some biologic plausibility at least here.
Delivery of oxygen to the tissues is dependent on HgB level. The oxygen content of blood is described by: O2 content = (gm Hbg)(1.34 ml O2/gm Hbg)(% sat) + 0.003(pO2) = ml O2/dL.
Oxygen delivery = cardiac output X O2 concentration (or content)
Could RBCs become less deformable and increase viscosity in low O2 environments? This could be the case when the HgB declines below 80 g/L. Such changes to deformability have been demonstrated at mild levels of hypoxia as might exist in low pO2 conditions at the tissue level with anemia.
So imagine we have fewer RBCs carrying as much oxygen as they can but eventually you cross a threshold where there is not enough O2 being delivered at the tissue level and the RBCs become lodged or perhaps sluggish as they move through capillaries of the intestines. Add to this that NEC occurs in watershed areas most commonly and you have the potential setup for NEC.
Can we use the results of this study?
I suppose statistical purists out there will argue that it is merely an association. The fact remains that there are many people who are holding feeds for varying amounts of time despite the lack of conclusive evidence that TANEC exists. I wonder if a middle ground might be to be more cautious and restrict such practice to those with low HgB values below 80 g/L as the authors here have found. To me at least there is biologic plausibility as outlined above. It would seem to me that to hold feeds for all babies is excessive and likely without evidence but could the threshold actually matter which it comes to oxygen content. Given that NEC is a condition related to ischemia, the authors here have provided another association that makes me at the very least scratch my head.
The importance of collaborating in a respectful manner cannot be overemphasized, as a calm and well prepared team can handle just about anything thrown their way. This past week I finally had the opportunity to take the 7th ed NRP instructor course. What struck me most about the new version of the course was not the approach to the actual resuscitation but the preparation that was emphasized before you even start! It only takes 30 seconds to establish who is doing what in a resuscitation and while it would seem logical to divide up the roles each will take on it is something that has not been consistently done (at least in our institution). When a baby is born and responds to PPV quickly, this may not seem that important but in a situation where a team is performing chest compressions, placing an emergency UVC and moving on to epinephrine administration it certainly is nice to know in advance who is doing what.
The Golden Hour
We and many other centres have adopted this approach to resuscitation and at least here developed a checklist to ensure that everyone is prepared for a high risk delivery. While teams may think they have all the bases covered, when heart rates are racing it may surprise you to see how many times crucial bits of information or planning is missed. As I told you in another post I will be releasing a series of videos that I hope others will find useful. The video in this case is of a team readying itself for the delivery of a preterm infant that they anticipate will have respiratory distress. Ask yourself as you watch the film whether your team is preparing to this degree or not. Preparing in such a fashion certainly reduces the risk of errors caused by assumptions about who is doing what or what risk factors are present.
As you can tell I am a big fan of simulation in helping to create high functioning teams! More of these videos can be accessed on my Youtube channel at
The rise of donor milk banks and depots in recent years has been a welcome addition to the care of preterm infants. We have known for many years that “breast is best” and advocate for mother’s own milk whenever possible. When this is not possible we previously turned to formula but with the availability of pooled pasteurized donor milk many hospitals have focused on expanding the indications for use. Through personal communications in Canada we are a bit all over the map in terms of indications with some centres restricting use based on birth weight while others taking into account, gestational age as the main criteria. With respect to duration some centres use 2 weeks, others 4 and then others until a gestational age is reached which may mean up to 10 weeks of use for a baby born in that centre at 24 weeks. While variation exists it is hard to find anyone who would suggest this is a bad thing to provide.
The main reason for pushing expansion of programs is the strong evidence that avoidance of bovine milk is associated with a reduction in the risk of NEC. Many studies have been done in this regard and the Cochrane systematic review concluded that formula increased the risk of necrotising enterocolitis: typical risk ratio 2.77 (95% CI 1.40 to 5.46); risk difference 0.04 (95% CI 0.02 to 0.07).
While donor milk is a wonderful nutritional product for sure it does have one issue which is a lower protein content than mother’s own milk and as such dieticians will commonly increase the protein content from 0.9 g/dL to 1.2 g/dL by adding powder or more recently liquid protein supplements. One might expect then that doing so would provide a reduction is NEC, and an optimal source of nutrition for the growing preterm brain. Avoidance of NEC should reduce the risk of adverse neurodevelopmental outcome as the two have been linked before.
Enter the DOMINO Study
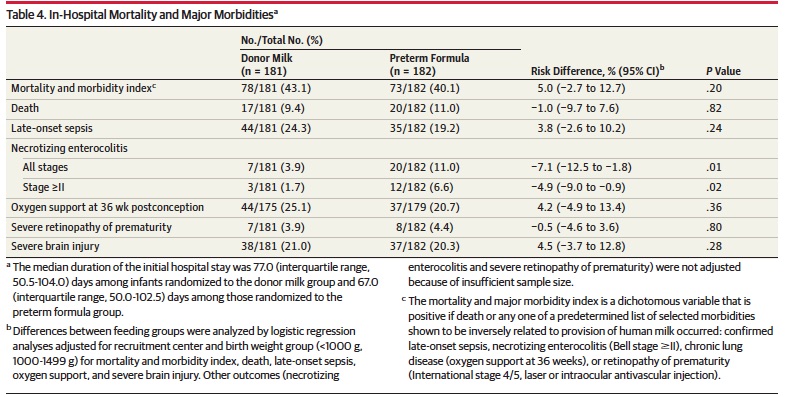
This Ontario, Canada based study utilized four NICUs to provide in a randomized fashion either donor human milk or formula with matching protein and caloric densities to 363 infants (181 donor milk, 182 formula). All infants were preferentially fed mother’s own milk but supplemented with donor or formula if unavailable and planned to use one or the other for up to 90 days or discharge whichever came first. The exposure to donor milk was quite long in comparison to our own units practice (1 month duration if born at < 1500g) . The median number of days for donor milk was 65 (IQR, 41-90). A significant risk to the results would be if there was a difference in amounts of mother’s own milk provided between the two groups but there was none. Exclusive feeding of mother’s own milk occurred in the Donor milk group (28.2%) and formula group (26.9%) respectively. Among infants requiring a supplement, there was no statistically significant difference between the donor milk and formula groups in the proportion of total enteral feeds for each infant consumed as mother’s milk (58.4% [IQR, 13.6%-96.0%] vs 63.3% [IQR, 9.6%-97.2%], respectively, P = .96).
Short term but not long term gains
Curiously (at least to me) I would have expected differences in some of the morbidities other than NEC but such was not the case.
The strength of using human milk though can not be understated as any reduction in NEC is an extremely important outcome regardless of whether long term neurodevelopment is affected positively or not.
in terms of the latter outcome no difference was observed between the two groups. The Bayley III findings were quite similar at 18 months which on the surface may cause everyone’s shoulders to sag as the benefit everyone hoped for did not transpire. Additionally, linear growth, head circumference and weight gain were not different between groups. This may simply reflect that protein and caloric intakes were indeed matched between groups whereas in the past, the lack of protein fortification led to delays in growth in the donor milk groups.
At the risk of sounding like the end of a Cochrane review I am not sure this is the final word on donor milk and outcome. Larger studies may be needed to get at the real truth. This was not a pure sample of donor milk vs formula as a significant percentage (over 20% in both groups) received purely mother’s own milk. Furthermore, in those that received supplements there was still a significant percentage that received some of mother’s own milk. The authors suggest that a larger sample size would unlikely have detected a difference and that may be the case but is it so due to where the study was done. What if the study were done in a centre with a very low rate of breastfeeding? I am concerned that the lack of response in outcome may reflect a dilution of the impact of the strategy by having such a successful rate of providing mother’s own milk.
All Is Not Lost
Using a glass is half full view, I think it is worth pointing out that this study should also provide some comfort for those centres that use formula as a supplement. Clearly the higher rate of NEC is not comforting to anyone but for those who survive to discharge the neurodevelopmental outcome is promising. Formula in some circles has taken on a view as almost a toxic substance but I often remind residents and fellows that while we prefer breast milk, formula has been used in NICUs for decades and not every patient who receives it will develop NEC. Yes it is a risk factor for NEC and when you don’t have an alternative it is an acceptable form of nutrition to use. What I think may be lost in the DOMINO study is that if you are a centre that uses formula as there is no access to DBM this should help provide reassurance to the families you care for. All is not lost after the DOMINO study. Every cloud has a silver lining and fear not this will not be the last study to test this hypothesis. At the moment it is just the best we have and this is not the last we will hear on this topic.
Rather excited this week as Biomed Central picked up a blog post that I wrote on social media. The post is found here. It is based though on a larger version that I have included below and really delves into the impact of social media and how one uses it. A big thank you to Kristy Wittmeier for all of her help in writing the post.
Original Piece
I read with great interest the article by Campbell et al entitled Social media use by physicians: a qualitative study of the new frontier of medicine. The study interviewed 17 physician users of social media of which only one writer of a blog responded, but then declined to participate. The four themes that emerged of Rugged Individualism, Uncertainty, Social Media as Media and Time Constraints certainly resonate with me as a blogger who also happens to be a Pediatrician but more specifically a Neonatologist. The first theme truly resonates with me as I think back over the journey that has taken me to where I am now. We in the medical social media world are certainly learning as we go. Without clear paths drawn for us we explore and contemplate how we will make a positive difference far beyond the reach of the typical physician in a clinic, hospital or local community. The commentary that follows explores the journey that I have taken with social media; engaging in largely unpaid work to bring information to others using these forums.
My own story as a Neonatal Blogger began in 2015 when my Minecraft-obsessed son asked me to help him start a blog about Minecraft. Two very poorly read posts started my foray into blogging using WordPress as my blogging forum. Around the same time, our family acquired a puppy and despite our best efforts over the next 18 months this new addition woke me between 4 – 5 AM daily. After being awoken one morning at 4 AM I read an article on NICU size as it relates to outcomes and had a marked reaction to the conclusions of the paper. On a whim on this early February morning, I chose to set up my own blog site, and All Things Neonatal was born. I would like to say that there was a master plan at the inception but it was due to a visceral reaction to a paper perhaps enhanced by irritability and fatigue that led to me choosing to put my thoughts out there. And I was hooked. A year and a half later, I have produced a total of 139 publications on the site.
Knowing the benefit that I have received, and hopefully also imparted by engaging in social media as a healthcare professional has sparked my interest in encouraging others to consider doing the same. And for those interested in going beyond considering to doing, I would like to share some key learnings from my journey to inform yours. To establish yourself in the realm of social media you need to utilize more than one platform, obtain your content in a time efficient manner and do not let your voice stay silent for too long.
Harnessing the combined power of multiple social media sites
When you begin blogging you come to realize that the method has its limitations in terms of reach. As the paper suggests, the polling of social media users identifies multiple potential websites for both collecting and disseminating information (Facebook, Twitter, Tumblr, Linkedin, Google+ as examples). Using them in combination can far enhance your reach. At the time of this writing the number of people who “follow” me on each site is quite disparate with Facebook by far leading the way in distribution power.
Table 1 – Variance in impact of commonly used social media websites
Site
Number of Followers
Facebook
11859
Twitter
921
WordPress (my primary blogging platform)
393
Also in the article, concern is raised over the lack of feedback for social media users as it pertains to to data on interaction with their postings. With Facebook one cannot determine what was done with your post but on twitter there is some further delineation as one receives a tally of impressions, engagements and link clicks. When it comes to real metrics though, this is where the actual blogging site provides more useful data. I recommend embracing metrics, not only to understand your reach but perhaps just as importantly to give you the drive to continue your writings. My most popular post, has received 5117 reads, meaning that this many took the time to open my blog post to hear what I had to say on the subject. If you were to share your thoughts on an article with colleagues via email, post a new guideline in an office or clinic or publish an article in a journal, how many people would actually see it? The same information, if cited in a blog post and shared through Facebook can see a dramatic rise in exposure, along with your interpretation of the work. The aforementioned post for example has had a reach on Facebook of 50934 people to date and was shared 58 times multiplying the distribution many fold. If you published a journal article and were notified of such circulation I suspect you would be jubilant.
How to obtain content?
One of the greatest benefits to my own practice has been the necessity of using a wide net to capture potentially interesting content for my readers. This habit facilitates the necessary practice of continuous learning through collecting articles from such sources as weekly automated pubmed searches, and various Child Health news websites. With time as your audience builds, postings on your own sites, tags on Facebook or mentions on Twitter draw your attention to content which your followers believe may be of interest to you. Remember in most circumstances you are not being paid for these efforts and in between managing the rest of your workday and balancing the demands of a personal life this aspect of your life needs to be done in a very time efficient manner.
Do Not Let Your Voice Stay Silent For Too Long
If you want people to pay attention to what you are adding to the pool of knowledge, deposits must occur frequently. Your followers are far more likely to mention you on various social media sites if they know you are likely to see and occasionally respond to their posts. Without such a presence, the mentions, likes and shares slow, as will your growth and relevance in the social media world. Future research should determine what the optimal frequency of posts to maximize reach would be. I have long suspected that excessive posting may have the effect of diluting the important messages while posting too infrequently means you may be quickly forgotten. Individuals must find the balance that works for them to keep their audience engaged while maintaining their motivation to continue the practice.
What Really Motivates Those Who Participate in Social Media?
I believe the motivation lies in the three qualities described by Malcolm Gladwell in his book The Tipping Point. He described three types of people that are needed for something to go from an idea to widespread adoption; connectors, mavens and salesmen. The doctors out there on social media likely have a little bit of all these characteristics. Gladwell said this about connectors; “They are people who “link us up with the world…people with a special gift for bringing the world together”. With respect to mavens he characterized them as having the ability to “start “word-of-mouth epidemics” due to their knowledge, social skills, and ability to communicate”. Lastly, salesmen in his view are “persuaders”. These three traits aptly describe those that have waded into this field. They must have the confidence to put their message out there with content that captures people’s attention and certainly have the goal of persuading people that it is worth considering what they have to say. The fundamental drive though comes from a place of harnessing these traits to help people. Whether writing original content or sharing what others have produced, the social media physician’s goal is generally pure and that is to share knowledge and generate discussion. For example, if you have a new strategy for reducing infection, the active social media physician would ask “why not share this with the world” rather than limit it to your institution or city.
This frontier like field though does come with some caveats before you dip your feet into the collective pool of the various media sites. As opposed to the more traditional medium of peer reviewed publications there is no one to assess your content prior to its release. You are your own editor and therefore may miss the mark from time to time by missing a relevant publication that might influence your conclusions. You must be prepared for the good and the bad. One can easily appreciate the positive comments that often come but not all posts will be “home runs” and on some occasions the feedback (which will be public) may not be what you had hoped for. You must constantly reflect on your own potential biases yet strive to improve base of knowledge; adding more ‘signal’ than ‘noise’. Respect for patient confidentiality is paramount and within Canada and elsewhere. Organizations such as the Canadian Medical Association have set guidelines for conduct in this space that should be adhered to. [Ref 3] This new frontier for the Rugged Individualist is therefore not for the faint of heart. It does however bring the world closer together and provide one with a post-publication form of peer review. Once you enter into the fray it may surprise you how much information is in fact out there, that now flows to you through global connections. It is an evolving form of communication and one that I am happy to part of. In fact, I am a better neonatologist for it. Is it right for you?


 The importance of collaborating in a respectful manner cannot be overemphasized, as a calm and well prepared team can handle just about anything thrown their way. This past week I finally had the opportunity to take the 7th ed NRP instructor course. What struck me most about the new version of the course was not the approach to the actual resuscitation but the preparation that was emphasized before you even start! It only takes 30 seconds to establish who is doing what in a resuscitation and while it would seem logical to divide up the roles each will take on it is something that has not been consistently done (at least in our institution). When a baby is born and responds to PPV quickly, this may not seem that important but in a situation where a team is performing chest compressions, placing an emergency UVC and moving on to epinephrine administration it certainly is nice to know in advance who is doing what.
The importance of collaborating in a respectful manner cannot be overemphasized, as a calm and well prepared team can handle just about anything thrown their way. This past week I finally had the opportunity to take the 7th ed NRP instructor course. What struck me most about the new version of the course was not the approach to the actual resuscitation but the preparation that was emphasized before you even start! It only takes 30 seconds to establish who is doing what in a resuscitation and while it would seem logical to divide up the roles each will take on it is something that has not been consistently done (at least in our institution). When a baby is born and responds to PPV quickly, this may not seem that important but in a situation where a team is performing chest compressions, placing an emergency UVC and moving on to epinephrine administration it certainly is nice to know in advance who is doing what.
 Two very poorly read posts started my foray into blogging using WordPress as my blogging forum. Around the same time, our family acquired a puppy and despite our best efforts over the next 18 months this new addition woke me between 4 – 5 AM daily. After being awoken one morning at 4 AM I read an article on NICU size as it relates to outcomes and had a marked reaction to the conclusions of the paper. On a whim on this early February morning, I chose to set up my own blog site, and All Things Neonatal was born. I would like to say that there was a master plan at the inception but it was due to a visceral reaction to a paper perhaps enhanced by irritability and fatigue that led to me choosing to put my thoughts out there. And I was hooked. A year and a half later, I have produced a total of 139 publications on the site.
Two very poorly read posts started my foray into blogging using WordPress as my blogging forum. Around the same time, our family acquired a puppy and despite our best efforts over the next 18 months this new addition woke me between 4 – 5 AM daily. After being awoken one morning at 4 AM I read an article on NICU size as it relates to outcomes and had a marked reaction to the conclusions of the paper. On a whim on this early February morning, I chose to set up my own blog site, and All Things Neonatal was born. I would like to say that there was a master plan at the inception but it was due to a visceral reaction to a paper perhaps enhanced by irritability and fatigue that led to me choosing to put my thoughts out there. And I was hooked. A year and a half later, I have produced a total of 139 publications on the site. He described three types of people that are needed for something to go from an idea to widespread adoption; connectors, mavens and salesmen. The doctors out there on social media likely have a little bit of all these characteristics. Gladwell said this about connectors; “They are people who “link us up with the world…people with a special gift for bringing the world together”. With respect to mavens he characterized them as having the ability to “start “
He described three types of people that are needed for something to go from an idea to widespread adoption; connectors, mavens and salesmen. The doctors out there on social media likely have a little bit of all these characteristics. Gladwell said this about connectors; “They are people who “link us up with the world…people with a special gift for bringing the world together”. With respect to mavens he characterized them as having the ability to “start “