I am fortunate to work with a group of inter-professionals who strive for perfection. When you connect such people with those with skills in multimedia you create the opportunity for education. I can’t say enough about the power of education and moreover the ability to improve patient outcomes when it is done well.
With this post I am going to be starting to share a collection of videos that I will release from time to time. The hope with any release like this is that you the reader wherever you are may find some use from these short clips. My thanks to the team that put these together as the quality is beyond compare and the HD quality is great for viewing on any device.
Placing A Chest Tube Can Be A Difficult Thing
As I said to a colleague in training the other day, a chest tube may seem daunting but once you see how it is done it loses some of its intimidation. Having said that, once you see it placed it can be a long time between opportunities for you to view another. That is where having a repository of videos comes in that you can watch prior to the next opportunity. These very short clips are easy to access when needed and may calm the nerves the next time you are called to place a chest tube.
A Word About Chest Tubes
The videos in question demonstrate how to place a Thal quick chest tube. In case this looks foreign to you it may be because you are using the older generation style of chest tubes that come equipped with a trocar. Even without the use of the trocar, these rigid tubes carry a significant risk of lung laceration or other tissue injury. For a review of such complications related to chest tube insertion see Thoracostomy tubes: A comprehensive review of complications and related topics.
The jury as they say is still out with respect to the use of these softer chest tube sets. There is no question that they are easier to place than the traditional thoracostomy tube. Their pliability though does carry a significant risk of kinking or blockage as we have seen in some patients when the Thal chest tube set is used to drain fluid in particular. Less of an issue with air leaks.
Start of a series
This post I suppose marks a slightly new direction for the blog. While I thoroughly enjoy educating you with the posts about topics of interest I see an opportunity to help those who are more visual in their learning. The videos will be posted over the next while with accompanying written posts such as this. They can be accessed on my Youtube channel at
The giant leaps in Neonatology may for the most part be over. So many outstanding research trials have brought us to where we are today. The major innovations of surfactant replacement, the discovery of nitric oxide and its later use to treat pulmonary hypertension, caffeine for apnea have all changed our field for the better. Cooling for HIE has certainly changed my practice in that I now truly have no idea what to tell parents after even some of the worst cases of asphyxia as our team has witnessed “miracles”after cooling. What will come next? My bet is that we are about to enter the era of Quality Improvement more and more. Think about the last study you read that had a major change in your practice or better yet made a substantial change in survival or neurodevelopmental outcome.
Tweaking care is where its at.
I like to think of it as fine tuning. As the era of the major leaps in care seems to be passing us by what I see more and more are studies looking at how to make further improvements on what we already know. In some cases such as using higher doses of caffeine may reduce the incidence of apnea further compared to standard dosing while cooling for 96 hours instead of 72 and at lower temperatures after asphyxia may not be such a good idea after all. There will be some studies that suggest a modification of practice and then others that suggest we should look elsewhere for further improvements. With all of this evidence coming out in hundreds if not thousands of journals every week it is difficult to keep up and it may be that our focus is in need of a change in direction or at least devoting members of the team to look at something different.
That Focus Is On Quality Improvement (QI)
Before I go on I don’t want to insinuate that I am something that I am not. I do not have any formal training in QI and consider myself an amateur but I do understand enough to undertake a PDSA cycle and see where it takes me. To me QI is about finding ways to actually make your best practices the best they can be. Take for example our units goal to minimize needle pokes by carefully examining the usefulness of common tests that we perform. Add to this the recent implementation of non invasive technology such as transcutaneous bilirubin metres which our evidence suggests can reliably replace a serum sample to screen for those in need of phototherapy. While I commonly like to praise our team for its ability to critically think about needed bloodwork it was only through the collection of data using audit tools that we discovered we had a problem. The problem was that the rate of CBC samples that were clotting were unacceptably high at over 30%. This was compared to another NICU in the same city that had a rate of less than 1/3 that. The initial reaction since it was trained lab personnel collecting at the low clotting site vs nursing at the high rate site was that the solution was simple. Just change back to lab personnel (as it used to be) at the high rate site! Ah but that would create another problem. Other evidence used to build a care plan for our preterm infants suggested that clustering of care was better for them than poking them at the usual run time of the lab techs so we had a conflict. How did we solve it? We resisted our urge for the quick fix and entered into a formal QI project.
How did we do it and what were the results?
It took us four rounds of PDSA cycles but in the end we found a solution that has lasted. As I write this I learned that one of our two units that had the high rates set a record low this past month of a 4.9% clotting rate even lower than the comparative site that began with a low clotting rate. It took work and was by no means easy but the dedication of our nurse educator to the task made all the difference. Fortunately, for those who don’t know where to begin an incredible resource is available from BMJ Quality Improvement who provide a step by step process to carry out your project. Moreover after using their template for publishing such work, we were able to publish our work which we hope may be of help for other centres that find themselves in a similar situation. Perhaps the solution might be the same or at least similar enough to try one of our interventions? The full paper can be found at the end of the post but the trend over time is so impressive that I felt obliged to show you the results.
Why should you care?
Teams spend so much time rolling out new evidence based initiatives. All the evidence in world won’t help if the intervention isn’t achieving the results you expect. How will you know unless you audit your results? You may be surprised to find that what you expected in terms of benefit you aren’t seeing. By applying the principals of QI you may find you don’t need to look for another treatment or device but rather you simply need to change your current practice. A little education and direction may be all that is needed. You may also find to your surprise that what you thought everyone was doing is not what they are doing at all.
Resist the quick solution and put in the time to find the right solution. As Carl Honore suggests slowing things down may be the best thing for all of us and more importantly the patients we care for.
Mohammed S et al. High versus low-dose caffeine for apnea of prematurity: a randomized controlled trial. Eur J Pediatr 2015 Jul;174(7):949-56.
Shankaran S et al. Effect of depth and duration of cooling on deaths in the NICU among neonates with hypoxic ischemic encephalopathy: a randomized clinical trial.JAMA 2014 Dec 24-31;312(24):2629-39
Anyone who attends the delivery of high risk newborns will eventually encounter a baby who is born “flat”. Most of these babies will respond to stimulation and for those that don’t, the vast majority of the remaining group will come around with the use of positive pressure ventilation. The remaining infants thankfully are the rare group but these are the ones that have the highest likelihood of dying or being severely impaired and therefore leave little room for error in their resuscitation if we hope to achieve a good outcome.
In 1816 Rene Theophile Hyacinthe Laennec invented the stethoscope to listen to the sounds of the heart and lungs. It is hard to believe that this coming year marks 200 years since that discovery and even harder to believe that when it counts most, this device still remains the best tool at your fingertips. When resuscitation has moved past the initial steps there is really nothing that can replace it’s accuracy when the going gets tough.
The most recent NRP guidelines recommend that all neonates who are receiving PPV have a preductal O2 pulse oximeter placed and oxygen titrated to the amount required to keep saturations within a range based on the age of the patient. Heart rate will be displayed when such monitoring is applied as well as when chest leads are placed giving you two readings of heart rate to compare. Such comparisons often prove useful when trying to determine if the displayed saturation is an adequate result. When looking at the recommendations from the NRP there is the clear statement that the best way of determining the heart rate is through auscultating the precordial pulse but does this always happen?
The answer as you might expect is no. Quite often during resuscitation I am told what the heart rate is based on the monitor. There is a danger in relying on such technology as you will see below. Recently I was called to the resuscitation area after the delivery of a non-vigorous infant. The patient was not responding to positive pressure ventilation as determined by the colour of the patient , which was dark purple despite confirmation of tube placement by end tidal capnography. The team was guiding their continued PPV without compressions based on the monitor which was showing a heart rate of 120-130 beats per minute and the belief that they had palpated a pulse. After hearing this and recognizing that the patient before me did not fit the reading on the monitor I reached for the stethoscope. The finding of no audible heart rate prompted us to start chest compressions.
What concerned me about this case was that the presence of technology actually hindered the institution of advanced resuscitation techniques. In the last few years much of the attention in the NRP program has shifted to monitoring during resuscitation. There have been many investigating the role of O2 saturation targeting, comparisons of chest leads versus pulse oximeters for acquisition of heart rates and stressing of the importance of attaching the probe to the patient and then to the monitor to improve signal acquisition times. This patient was in Pulseless Electrical Activity (PEA) which went unrecognized due to an adequate heart rate being visualized on a monitor in the context of a non-congruent clinical exam. PEA is a state in which the heart is still experiencing electrical conduction but there is not enough contractility to eject blood.
Another interesting aspect to this case was the claim that the infant had an adequate pulse. When I say claim I don’t mean that I believe the person in this case was lying but rather they believed they felt a pulse. As with many other posts I felt obliged to ask the question “How accurate is assessment of a pulse in a resuscitation?” As much as we would like to think we all stay calm under pressure there is no doubt that when it counts most and our heart is racing from our sympathetic nervous system on overdrive, we may experience the opposite state. A nicely done study addressed such accuracy in 2009 using patients who were on heart lung bypass. 209 doctors and nurses were asked to blindly assess presence or absence of pulse with the manipulation of pulsatility by using the presence of a left ventricular assist device or not. The findings of this study are somewhat disturbing in that 22% of the time they were wrong about the presence of a pulse. In this study they were given as long as they wanted and in no way were under stress to perform. They simply had to say after taking as much time as they needed whether the pulse was present or not. How accurate do you think they would be with a newborn, covered in amniotic fluid and blood with people giving resuscitation orders? Not very accurate I would say.
The NRP program recommends that a rising heart rate is the best indicator of a successful resuscitation. Two hundred years ago a physician brought the stethoscope into our repertoire of tools at our disposal in medicine. Despite all of our focus on non-invasive monitoring during resuscitation, confirmation of a heart rate should only be done by auscultation. Technology serves a useful purpose by providing confirmation of rhythm after hearing the heart beat but should never be used as a substitute for one of the oldest technologies there is.
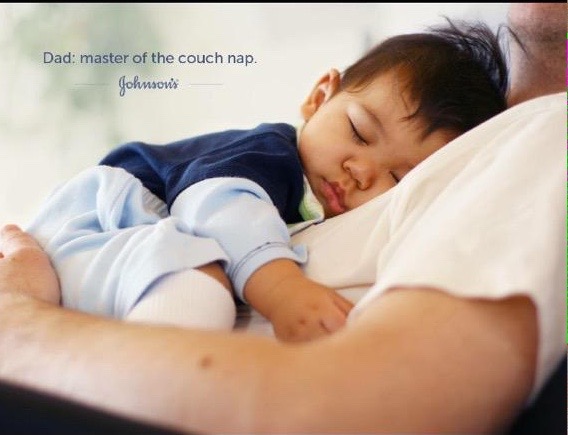
This post is a re-release due to a furor on twitter over the last month of the release of a Johnson’s Baby (July 17) showing the infant sleeping with dad on a couch. Johnson and Johnson has since spoken out about the ad and clearly stated it was not their intention to show unsafe sleeping practices but as a company working in the field of newborn care I do believe there is a responsibility to demonstrate safe sleeping practices and as you will see when you read on the couch is not one of them…
One of the greatest achievements of the 1990s in infant health has to be the “Back to Sleep Campaign” which has undergone a name change to the Safe to Sleep Campaign.
The back to sleep campaign achieved incredible results in reducing the risk of SIDS. Since its inception the program reduced the rate of SIDS by approximately 50% although annually in the US there remain approximately 4000 deaths per year. SIDS is clearly a parent’s worst nightmare and it is important to disseminate any information that we can to try and further reduce SIDS in addition to the Safe to Sleep campaigns achievements.
Much of what I am writing, I would really encourage readers to incorporate into discharge planning whether you are working in an NICU or postpartum ward. The advice is based on well done research and although not part of a randomized trial which is our gold standard, it has been found across many studies. These risks are now accepted as modifiable factors and as part of our responsibility to advocate for our patients this is one thing we can and should talk about.
Smoking, Alcohol, Illicit Drug Use and Partner Violence
These have been identified as risk factor for SIDS both prenatally and in the homes of newly born infants. As it has been associated, it is not always clear whether smoking and drug use in and of themselves cause biochemical or developmental changes in the developing fetus that predisposes them to SIDS or if it a marker for something else such as socioeconomic status. That being said there are many reasons to deter people from these factors so I would see this as a strong area for advocacy.
Co-sleeping
This has been appreciated as a risk factor for SIDS for many years although I suspect many parents are unaware of its risk. I can understand how it can happen and why some mother’s who are wanting to encourage breastfeeding favour it. Having your infant with you such that the moment they wake you can turn to them and feed them is simple and avoids having to go back and forth from rooms particularly when you have a “snacker” on your hands and you are exhausted from the endless night time feeding. This has and will likely continue to be cited as a risk though for SIDS and should be discouraged. What remains a little unclear is whether co-sleeping by itself is actually a risk in the absence of other factors as outlined in the above paragraph. A meta-analysis of multiple studies by Carpenter indicated that co-sleeping with or without the above factors placed infants at risk of SIDS although the risk was increased further when such factors were present.
Curiously Blair PS et al found exactly the opposite result that in the absence of risk factors of smoking, alcohol or drug use the practice of co-sleeping appeared to add no additional risk for SIDS.
So the jury is perhaps out as to whether co-sleeping in the absence of other risk factors increases the risk of SIDS given the conflicting studies but in the presence of uncertainty I would at least caution that the practice should be avoided if there is the potential for actual risk.
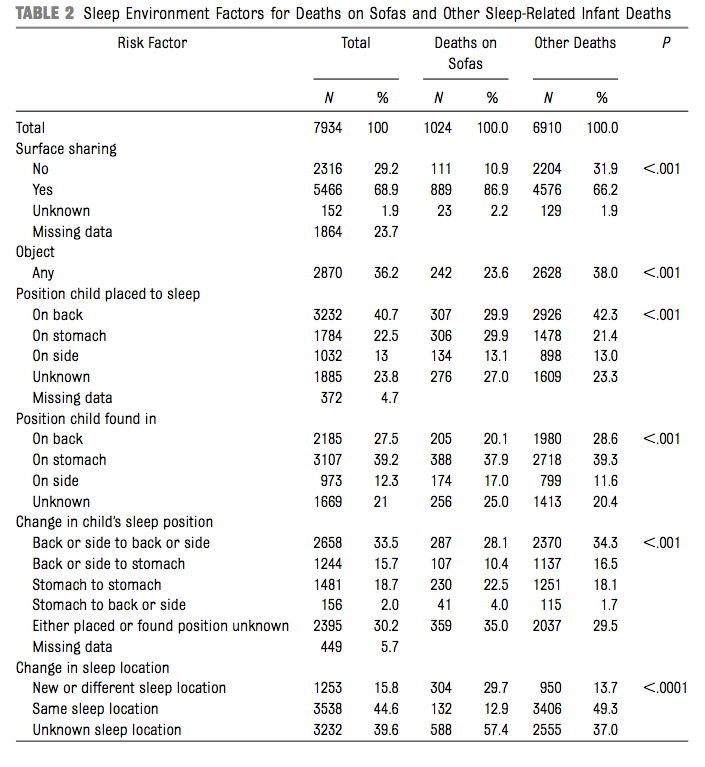
What has been consistent however is that the use of the sofa as a sleeping surface is one that should be avoided. Avoidance should include even naps with your infant as it doesn’t take very long for an adverse outcome to be realized. In previous studies in fact the risk has been estimated to be 67 times that of sleeping in a bed. A recent well done study of 9073 sleep related deaths found that 1024 occurred while co-sleeping on sofas. This study documented all deaths from 2004-2012 and demonstrated a 12.1% incidence of death in this environment. As a probable explanation for the increased risk found with this position, more infants were likely to have been placed prone or side lying while sleeping on the sofa with a parent. Suffocation in this position particularly if wedged in between the parent and the cushion would be far more likely. The complete study can be found here. For risks while sleeping on sofas see the accompanying table.
In the end as health care providers anticipatory guidance needs to be part of all of our practices. We all talk about “Back to Sleep” but do all programs caution about the risks of napping or sleeping with your infants on a sofa? We have a chance to make a real difference and eliminate over a 1000 deaths a year that are attributable to this position. I know it is easy to take a quick nap with a child on the sofa but is the risk worth it? That is something every parent needs to decide for themselves but the first thing is getting the information into their hands so they can make an informed decision!
I know, this sounds like a ridiculous title to a post but it actually happened in Detroit recently. Krista and Jamie Contreras loving parents of 6 day old Bay were denied care by a Pediatrician solely due to the parents being Lesbians. Please watch this short video before reading on.
I can’t help but think that the recent laws that have been passed in Indiana and Arkansas open the door for similar situations in those states. Moreover, imagine the impact if the laws spread to other conservative states in the US. If you look at some history though, the Religious Freedom Restoration Act (RFRA) was first passed in 1993. The act was brought into being after an American Indian man was fired from his job for failing a company drug test. The drug in this case was peyote which culturally was acceptable for him to use but not in keeping with company policy. The law that was brought into existence was therefore designed to protect people from the Government and industry interfering with religious practices which in this case they were as peyote was used as part of his religious practice.
That sounds like a very positive step in the right direction so why have Indiana and Arkansas come under so much heat over this current legislation? The reason is that the law makes it possible for not only the individual but a company or business to sidestep the law if their religious beliefs are found to be in conflict with a person or request. Don’t believe this could happen? It already did. The US Supreme Court recently ruled that the HobbyLobbycompanycouldrefuse to providebirthcontrol to employees as a healthbenefit. Usingbirthcontrol violates the company’s Christianreligiousbeliefs.
The physician in this case lacked a solid RFRA in Michigan so she could do nothing more than apologize for her stance. What concerns me greatly though is the hypothetical situation in which a member of the Lesbian Gay Bisexual Transgender (LGBT) community decides to have a child with a member of the same sex in a state with an RFRA. What if for instance Michigan had such a law? Would this Pediatrician have apologized or simply stood behind the government? I am not sure what would have happened and in a state like Michigan which in my view is a little more progressive than some of the states in the “Bible Belt” I suspect this family would have found another Pediatrician to take care of them. If this story had taken place in Arkansas, how difficult would it have been to find another Pediatrician on short notice while the infant was still hospitalized? Might be a little harder.
On the first day of Medical School all students are asked to take the Hippocratic Oath. The Oath is not the same as was first spoken by Hippocrates but rather in one form or another is based on the version that came from the Declaration of Geneva and reads as follows:
At the time of being admitted as a member of the medical profession:
I solemnly pledge to consecrate my life to the service of humanity;
I will give to my teachers the respect and gratitude that is their due;
I will practice my profession with conscience and dignity;
The health of my patient will be my first consideration;
I will respect the secrets that are confided in me, even after the patient has died;
I will maintain by all the means in my power, the honour and the noble traditions of the medical profession;
My colleagues will be my sisters and brothers;
I will not permit considerations of age, disease or disability, creed, ethnic origin, gender, nationality, political affiliation, race, sexual orientation, social standing or any other factor to intervene between my duty and my patient;
I will maintain the utmost respect for human life;
I will not use my medical knowledge to violate human rights and civil liberties, even under threat;
I make these promises solemnly, freely and upon my honour.
Point number 4 states “The health of my patient will be my first consideration”. Furthermore point #8 specifically spells out that sexual orientation should not matter.
In essence the newborn baby is in need of treatment and you are obligated to provide such treatment without consideration of whether the parents are members of the LGBT community.
Quite frankly I am embarrassed for this physician. Do not misunderstand my intention here though. Whether I support the LGBT community or not is irrelevant to this discussion. What is relevant is that a member of the medical community who swore an oath to put the patient first has violated that oath. It is my hope that these words will reach the eyes or ears of physicians who may have had similar thoughts and remind them of the oath that they once swore to uphold. The United States is at a tipping point (quoting Malcolm Gladwell again) where physicians or medical corporations may opt to refuse treatment for infants who happen to be born to LGBT parents. The infant was born into this world and needs someone to care for them from a medical standpoint. Whether their parents choose to be intimate with members of the same sex should never enter the equation and I hope that this is the last report I hear of this behaviour by a member of the medical community. Sadly as I often say hope is not a good plan and I fear that this indeed will not be the last instance we hear of.
The President of the United States no doubt wishes to leave a legacy as he prepares to leave office. Obamacare, a nuclear deal with Iran and a two state solution for Israel and the Palestinians will be great accomplishments if they last. Sadly if he doesn’t weigh in and do something soon the ability of companies, organizations and governments to discriminate against member of the LGBT community will leave a black mark on the Presidency that will be remembered long after the Republicans undo much of what he feels will be his “accomplishments”.


 The videos in question demonstrate how to place a Thal quick chest tube. In case this looks foreign to you it may be because you are using the older generation style of chest tubes that come equipped with a trocar. Even without the use of the trocar, these rigid tubes carry a significant risk of lung laceration or other tissue injury. For a review of such complications related to chest tube insertion see Thoracostomy tubes: A comprehensive review of complications and related topics.
The videos in question demonstrate how to place a Thal quick chest tube. In case this looks foreign to you it may be because you are using the older generation style of chest tubes that come equipped with a trocar. Even without the use of the trocar, these rigid tubes carry a significant risk of lung laceration or other tissue injury. For a review of such complications related to chest tube insertion see Thoracostomy tubes: A comprehensive review of complications and related topics.
 As the era of the major leaps in care seems to be passing us by what I see more and more are studies looking at how to make further improvements on what we already know. In some cases such as using
As the era of the major leaps in care seems to be passing us by what I see more and more are studies looking at how to make further improvements on what we already know. In some cases such as using 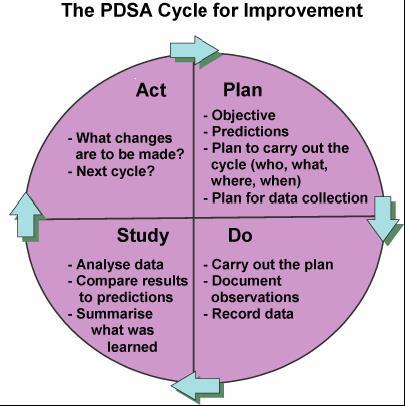 To me QI is about finding ways to actually make your best practices the best they can be. Take for example our units goal to minimize needle pokes by carefully examining the usefulness of common tests that we perform. Add to this the recent implementation of non invasive technology such as transcutaneous bilirubin metres which our evidence suggests can reliably replace a serum sample to screen for those in need of phototherapy. While I commonly like to praise our team for its ability to critically think about needed bloodwork it was only through the collection of data using audit tools that we discovered we had a problem. The problem was that the rate of CBC samples that were clotting were unacceptably high at over 30%. This was compared to another NICU in the same city that had a rate of less than 1/3 that. The initial reaction since it was trained lab personnel collecting at the low clotting site vs nursing at the high rate site was that the solution was simple. Just change back to lab personnel (as it used to be) at the high rate site! Ah but that would create another problem. Other evidence used to build a care plan for our preterm infants suggested that clustering of care was better for them than poking them at the usual run time of the lab techs so we had a conflict. How did we solve it? We resisted our urge for the quick fix and entered into a formal QI project.
To me QI is about finding ways to actually make your best practices the best they can be. Take for example our units goal to minimize needle pokes by carefully examining the usefulness of common tests that we perform. Add to this the recent implementation of non invasive technology such as transcutaneous bilirubin metres which our evidence suggests can reliably replace a serum sample to screen for those in need of phototherapy. While I commonly like to praise our team for its ability to critically think about needed bloodwork it was only through the collection of data using audit tools that we discovered we had a problem. The problem was that the rate of CBC samples that were clotting were unacceptably high at over 30%. This was compared to another NICU in the same city that had a rate of less than 1/3 that. The initial reaction since it was trained lab personnel collecting at the low clotting site vs nursing at the high rate site was that the solution was simple. Just change back to lab personnel (as it used to be) at the high rate site! Ah but that would create another problem. Other evidence used to build a care plan for our preterm infants suggested that clustering of care was better for them than poking them at the usual run time of the lab techs so we had a conflict. How did we solve it? We resisted our urge for the quick fix and entered into a formal QI project.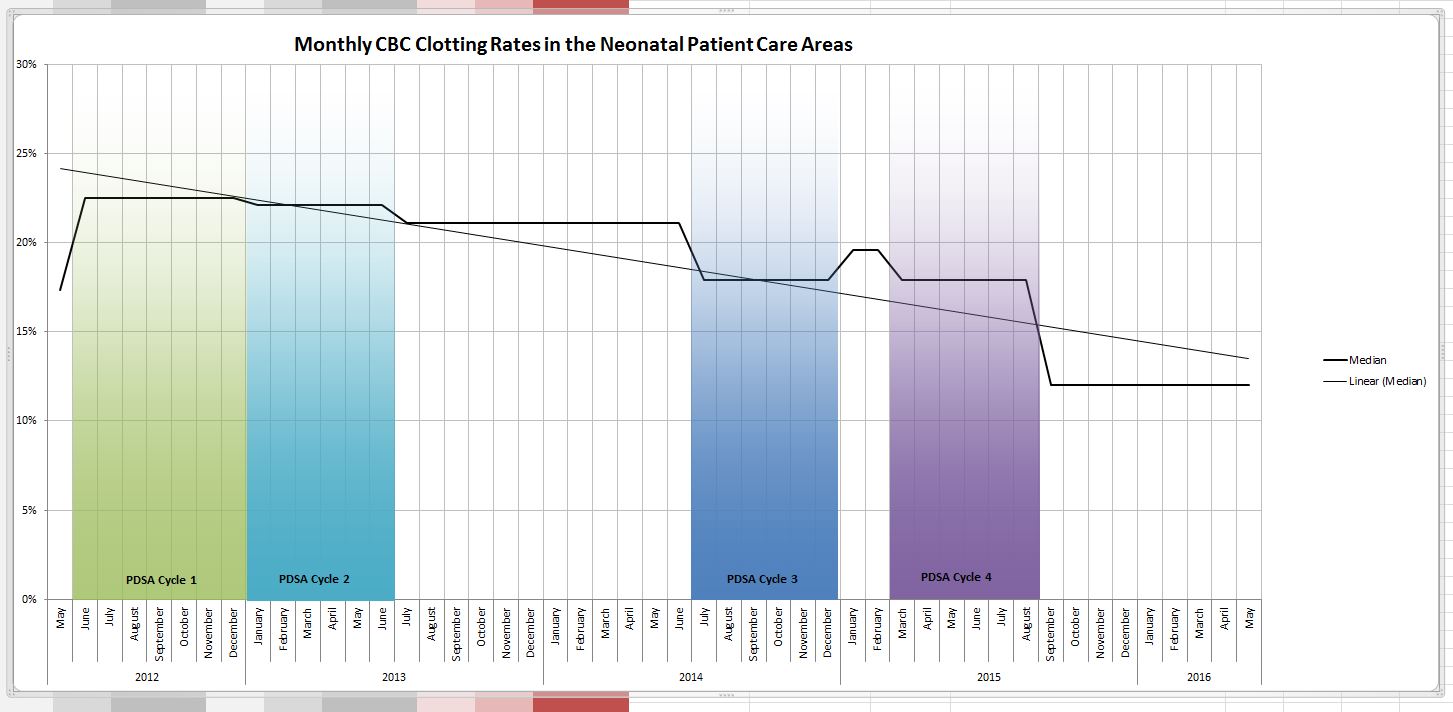
 A little education and direction may be all that is needed. You may also find to your surprise that what you thought everyone was doing is not what they are doing at all.
A little education and direction may be all that is needed. You may also find to your surprise that what you thought everyone was doing is not what they are doing at all.


{kind=link}