As awful as COVID19 has been over the last year and a half one thing has continued to perplex myself and others. Why do babies whethe term or preterm so rarely acquire the virus? Numerous studies have been able to document placental changes and infection of these tissues. On rare occasions reports have come out with evidence of neonatal infection but fortunately most are mild.
These findings have in large part contributed to the Canadian Pediatric Society practice points on three topics.
In this post an argument was made that the reason these infants are resistant is due to low levels of ACE-2 receptors in the nasal mucosa of children. In this study children as young as 4 years of age were found to have very low levels of this receptor (portal of entry for SARS-CoV-2) into the host. I speculated at the time that if one carried forward the findings to younger children and infants you might find there were hardly any receptors at all.
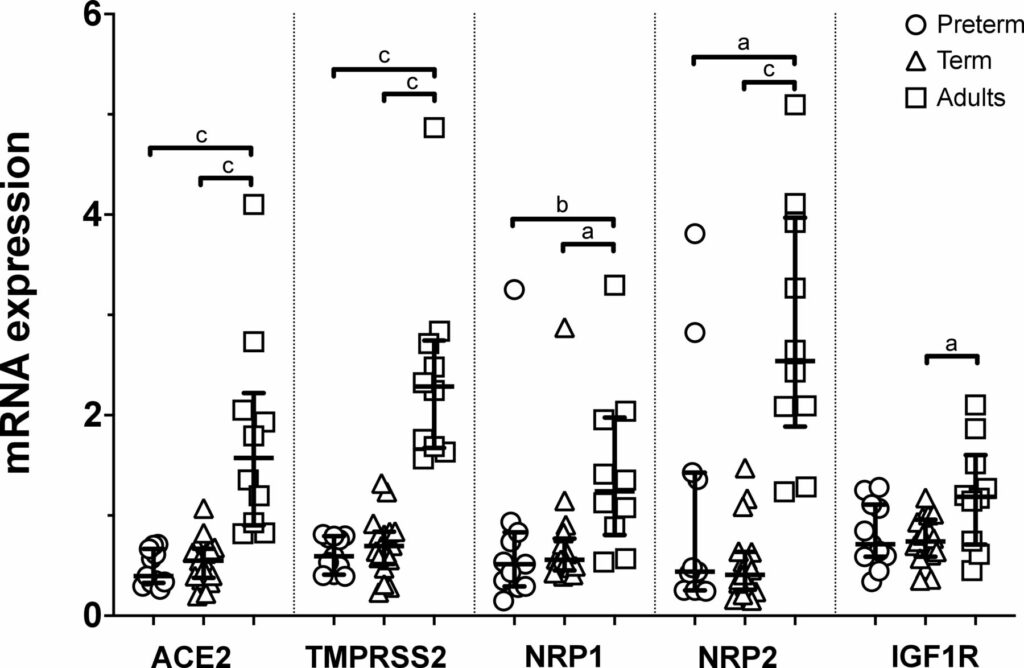
Well, someone finally did the study and confirmed what I suspected. The study report is entitled Nasal expression of SARS-CoV-2 entry receptors in newborns by Heinonen S et al. It’s not a big study but the results are consistent across 28 newborns (17 term and 11 preterm) and 10 adults. In each newborn whether term or preterm a nasal mucosal scraping was performed at 24 hours of age and used to measure by reverse-transcription quantitative PCR mRNA expression of ACE2, transmembrane serine protease 2 (TMPRSS2), neuropilin 1 (NRP1) and neuropilin 2 (NRP2) and insulin-like growth factor 1 receptor (IGF1R).
What the results show you is that babies are not just small adults. They are different yet preterm do not seem to be that different than term infants in terms of receptors. While ACE2 has garnered most of the attention when it comes to receptors for SARS-CoV-2 the others also play a role and are in general expressed to a lesser degree in neonates than adults.
Conclusions
In the previous post I argued what was in your nose makes a difference to your risk of contracting SARS-CoV-2. Really the point is what is not in your nose. Thankfully neonates do not have good expression of these receptors and that may be the biggest reason for the general protection they have from this pandemic. It has certainly a good time to be in the “have not” group!
A couple years back at the Canadian Pediatric Society annual meeting a discussion broke out about extubating infants to higher levels of CPAP. Conventional thinking had been to use levels between 5 – 8 cm H2O typically. I shared with the group the experience we had in Winnipeg (unpublished) of using higher levels from 9 -12 cm H2O with some degree of success in allowing earlier extubation. The group thought it was interesting but pointed out the lack of robust research in the area so were not so keen to “try it out”. Non-invasive positive pressure ventilation (NIPPV) has been used for some time in the neonatal world and has been compared to CPAP for extubation success and found to be superior as in this review Comparison of Complications and Efficacy of NIPPV and Nasal CPAP in Preterm Infants With RDS. In this review though as in others more typical CPAP levels are used so the question is whether the same efficacy would be seen with high level CPAP vs NIPPV.
Canadian Study to the Rescue
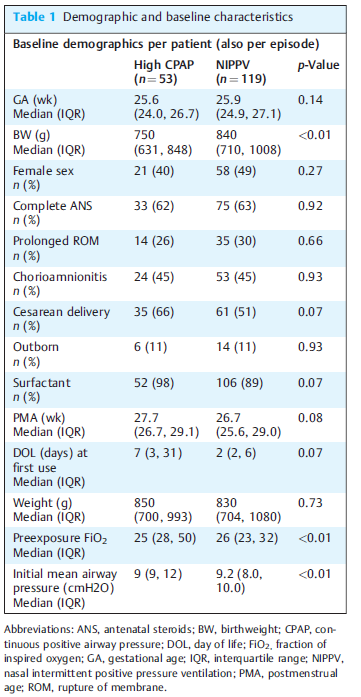
The study here is by Ahmad HA et al Comparison of High CPAP versus NIPPV in Preterm Neonates: A Retrospective Cohort Study and seeks to answer this question albeit in a retrospective fashion. The study is not well controlled since it is retrospective but it may be the best we have for now. Over a 3 year period the authors examined the outcomes for babies trialed on high CPAP (hCPAP of at least 9 cm H20) vs NIPPV. In each case they looked at the first episode of use. The modalities could have been used for extubation or as a primary means of support. The primary outcome was failure of the modality as defined by either intubation or change to the other strategy within 7 days. A total of 53 infants received hCPAP vs 119 NIPPV. Why the big difference? Since this was retrospective and not randomized it was up to the individual practioner which modality they wanted to try. If the majority of the unit favoured NIPPV this is why there would be such a difference. Herein lies the benefit of the primary outcome as if “conventional wisdom” was wrong and the other modality would be better then we should see a greater movement to the other strategy or more intubations in one group suggesting superiority of one vs the other.
The groups however aren’t entirely equivalent at baseline. The babies in the hCPAP group are quite a bit smaller on the one hand which would favour the NIPPV group. On the other hand there is almost a significant difference in surfactant provision for the hCPAP arm which might favour the hCPAP group. The other thing also nearing statistical significance is when the intervention was trialed. The median time is 2 days for teh NIPPV group and 7 for hCPAP suggesting one may have been used more prophylactically and the other post extubation. Different strategies might make a difference to outcome? Also no infants received MIST or INSURE and all were started on traditional lower levels of CPAP prior to surfactant.
Results
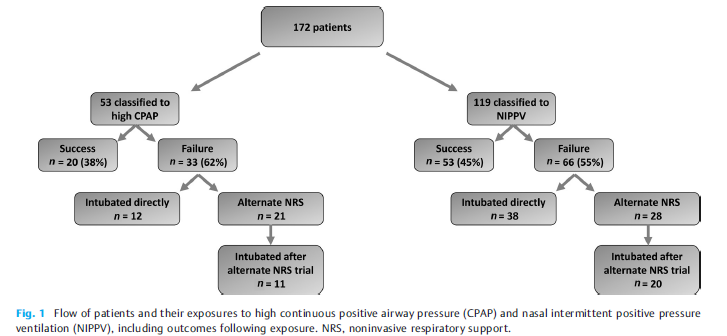
The results tell an interesting story (I think) with the primary outcome being no different 62% in the hCPAP vs 55% with NIPPV. Looking at the patient outcomes in the figure from the paper one gets a little more detail and can surmise how people viewed the two modalities as a strategy and can see they were a bit different.
There seems to have more confidence in the unit with NIPPV as a way to prevent intubation. For those that failed hCPAP 12/33 were intubated as the next step (about a third) while the other 2/3 were trialed on NIPPV. Looking at those started out on NIPPV, 38/66 were intubated directly 58% or almost 2/3 while 28/66 were trialed on hCPAP. Of the ones trialed on hCPAP 20/28 or 71% were still intubated. Comparatively of those who were changed from nCPAP to NIPPV 11/21 were intubated or about 50%.
The authors find no difference in the primary outcome which is true. The problem of course with this analysis though is that there was no standardization with determining when one would choose to intubate. This issue can really play with the results. Let’s say for example that one Neonatologist really believes for the most part that NIPPV is the mode that can really prevent intubation more than hCPAP. It is conceivable that the reason in crossover intubations are less with NIPPV is that people were willing to tolerate a slightly higher pCO2 or a couple more apneas since they believe the modality is best and the infant will “get better soon”. On the other hand, infants already on NIPPV who are deteriorating might be intubated more readily as the attending might think “this hCPAP is a bunch of malarky”
It is worth mentioning that the incidence of air leak was no different between the two, nor was NEC or feeding intolerance from exposing the babies to such high pressures.
Conclusions
The study doesn’t “prove” anything. I don’t see it as a complete waste though as it does a number of things. It does show that small infants can be managed with hCPAP in NICU without any significant increase in complications. It also sets the stage for a couple future prospective trials I can see. Firstly, a trial of traditional CPAP vs hCPAP is needed as some units don’t have access to NIPPV or simply don’t use. The second is a prospective trial with clear parameters for failure between hCPAP and NIPPV. Lastly, the authors ran the NIPPV and CPAP off ventilators in the units. The work of breathing would be potentially different with the use of devices solely designed for CPAP with fluidic flips. It would be important to use optimal devices for both modalities in such a trial and I for one can’t wait to see them.
What can I say? I have had a love affair with research on hypoglycemia. I suppose ever since my colleague and I began the quest of rewriting the Canadian Pediatric Society statement The screening and management of newborns at risk for low blood glucose it has become an interest. Embedded in the statement is commentary on the use of glucose gels for management of neonatal hypoglycemia and based on the sugar babies trial that found treatment of hypoglycemia with dextrose gel reduced admission for hypoglycemia and improved rates of breastfeeding after discharge I have been a proponent. A new approach has arisen in a large study in neonates that warrants some discussion. It tackles hypoglycemia from a preventative approach rather than as a treatment per se and is presented below.
The hPOD Study
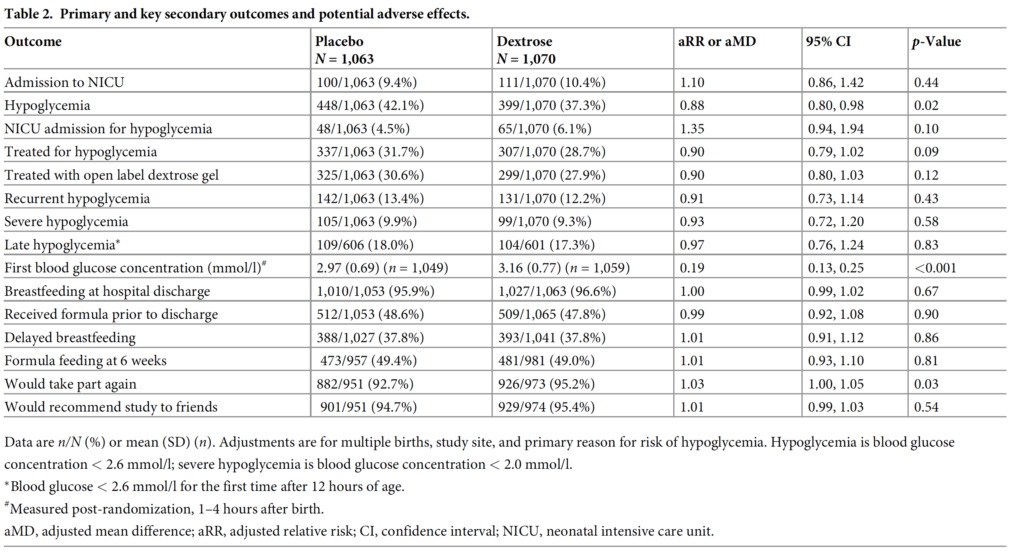
The same group from Auckland led by Jane Harding published a preventative trial in January entitled Evaluation of oral dextrose gel for prevention of neonatal hypoglycemia (hPOD): Amulticenter, double-blind randomized controlled trial. The study approached the problem of hypoglycemia by looking at whether provision of dextrose gel at 1 hour of age along with a breastfeed could reduce admission to NICU. The targeted population were babies with risk factors for hypoglcyemia such as maternal diabetes, late preterms and SGA or LGA infants. Remarkably this multicentre study managed to randomize 2149 infants into dextrose (1078) and placebo 1071) arms which for a neonatal study is pretty big! Blood glucose levels were analyzed on all at risk infants at 2 hours of age and were then followed up every 2-4 hours for the first 12 hours of age and until there were 3 consecutive measurements greater than or equal to 2.6 mmol/L. Given the size of the study it should come as no surprise that the two groups were similar in terms of baseline characteristics. The most common risk factor for hypoglycemia in each group was maternal diabetes at 81% in each group.
In the end the only thing that was different between the two groups was a diagnosis of hypoglycemia with about a 5% reduction in the outcome. Admission to NICU was no different whether it was for any reason or hypoglycemia alone. Treatment with IV therapy was also no different between groups and in addition breastfeeding rates were exceptionally high at discharge at about 96% for both groups. So the conclusion here is that prophylactic glucose gel doesn’t matter much but I have a few thoughts despite this being a VERY large trial and the authors really doing a good job of answering an important question.
My Thoughts on the Outcomes
The study demonstrates that one dose of glucose gel does not affect admission for any reason or for hypoglycemia. I can’t help but wonder if allowing the dextrose gel group to receive one or two more doses could have changed that outcome.
No difference in admission is not surprising since there are many reasons that a baby could be admitted with those underlying risk factors. Low birth weight, TTN, RDS etc would be some reasons and I wouldn’t think would be any different. It might have been better to power the study for admission for hypoglycemia as that to me is the only reason for admission that could be impacted by such prophylaxis.
When your breastfeeding rate in the placebo arm is at 95.9% there really isn’t much room for improvement so not sure a lack of improvement with dextrose gels can really be called here. There really wasn’t anywhere to go but down and previous work suggested that rates can go up. As the saying goes, can you apply the results of the study to my population. I can only wonder what would have happened if the authors were to replicate this study in a population with breastfeeding rates of 80%.
Is the outcome of reduced hypoglycemia a good enough outcome alone to adopt prophylactic dextrose gel? I don’t think so as there was no difference in groups between recurrent or severe hypoglycemia which is what likely matters most to neurodevelopmental outcome. Curiously the mean initial blood glucose was 2.97 and 3.16 in the placebo and glucose gel arms respectively so I am not sure how hypoglycemic this population really was. Yes there were about 40% in each arm that were hypoglycemic but only 10% were severe and almost 90% never had another episode. It’s possible that just by chance these children were on a very mild spectrum and therefore prophylaxis had little effect since they really were only going to have transient hypoglycemia.
In spite of my comments above I believe the authors did a fine job trying to answer an important question which to be honest others have wondered about before. For now I won’t be recommending this in my own institution but I do wonder what project will come next from this group that keeps on producing great work in the area of neonatal hypoglycemia.
This post is a written as a tribute to John Minski RRT who taught me much about ventilation over the years and has been a champion for innovation in our unit. As he prepares to move on to the next phase of his life I thought it would be a nice send off to talk about something that he has been passionate about for some time. That passion is inhaled nitric oxide for more than just pulmonary hypertension.
Prior Evidence
This is actually nothing really new. For a review on the background behind the theory you can read The potential of nitric oxide releasing therapies as antimicrobial agents. While we think of iNO as being a drug for pulmonary hypertension it has other capabilities. It can diffuse across cell membranes and damage pathogens by causing nitrosative and oxidative damage. The amount of iNO needed though to accomplish this bactericidal action is much higher than the typical levels of 20 – 40 ppm that we use. Last year in August Bogdanovski et al published Antibacterial activity of high-dose nitric oxide against pulmonary Mycobacterium abscessus disease. They describe a protocol of providing 30 minute doses of 160 ppm for 21 days in a 24 year old patient with cystic fibrosis who was infected with mycobacterium abscessus. While they were not able to eradicate the organism, they were able to demonstrate functional improvement in the patient. Also notable was the absence of adverse effects in terms of methemoglobin levels. Other prior research in-vitro has shown iNO at high levels to be truly bacteriocidal as per the review above.
In this paper they describe the use of iNO at 160 ppm in 5 spontaneously breathing patients with confirmed COVID19 infection. This was provided as a rescue therapy in the absence of any high quality therapies for this disease. The protocol was to give them the same dose of 160 ppm for 30 minutes at a time until resolution of their symptoms with those that received multiple treatments getting anywhere from 5-9 courses. In each case after each 30 minute period the treating physicians measured levels of methemoglobin and nitrogen dioxide and found in each patient acceptable levels after these brief exposures.
Results
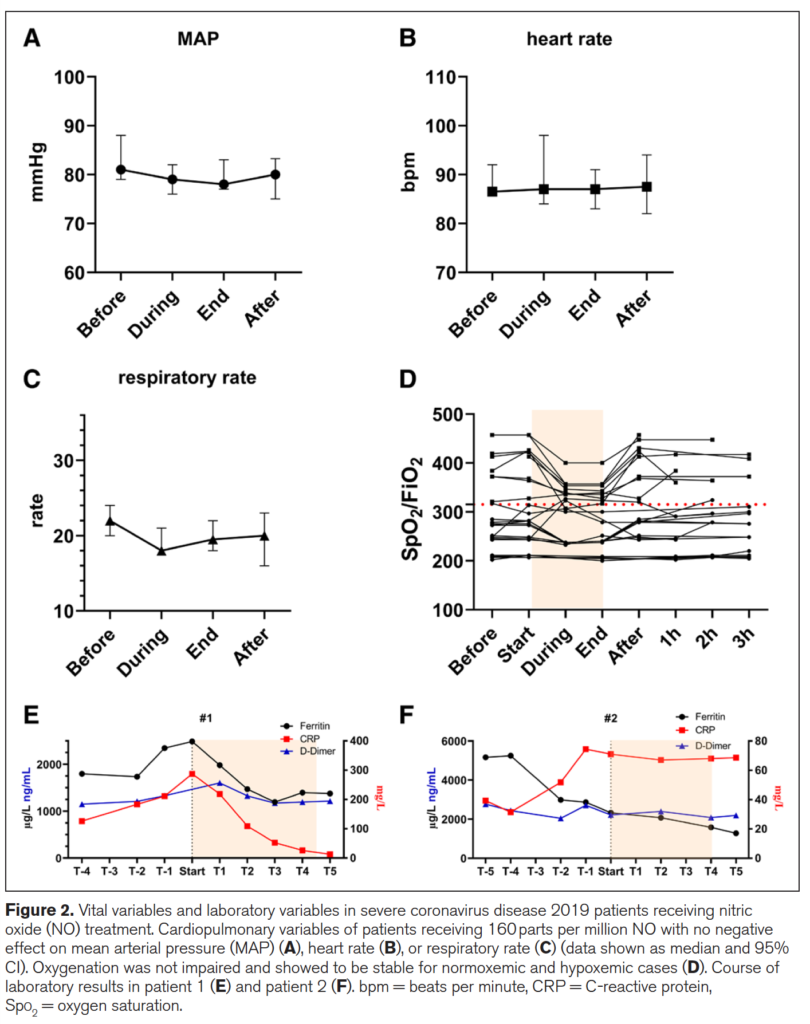
Of the 5 patients treated 2 died from COVID19 and three survived. The two patients who died interestingly were the ones who each only received one treatment each. The other three received 5, 8 and 9 treatments respectively. The authors recorded mean arterial pressure, heart rate, respiratory rate, SpO2/FiO2 and finally measurements of inflammatory markers in the two patients who died (E) and the 3 who survived in (F) in the figure below.
What is interesting from the figure above is the reduction in respiratory rate during treatment (certainly could be placebo from believing they will get better) but the oxygenation during the treatment improved as well. Could this be from a reduction in associated pulmonary hypertension? Certainly could be. Looking at the patients who died in (E) vs the ones in (F) who survived (patient 3 not shown) demonstrate that use of iNO stopped the rise in CRP and in the case of those who died reduced it significantly. There could be an argument made then that the changes in respiratory pattern observed during treatment are associated with a concomitant attenuation of inflammation. This treatment just might work but of course needs far more studies to be certain of that. On that note a review of iNO for this type of indication reveals there are currently 16 studies enrolling in this area of research so I imagine there will be more info to come with this story.
What about the neonate with pneumonia?
I sent this paper around to my colleagues and it generated some great discussion. I am no Ethicist but the question raised was could this be considered a “last ditch” treatment for the neonate succumbing to a pneumonia? I have no doubt if you are reading this that you will have seen in neonatal units around the world that there are infants who develop pneumonia unresponsive to traditional treatments such as iNO at regular doses, antibiotics, higher PEEP, surfactant etc. If we have this knowledge with respect to the potential use of iNO at high dose and a positive impact on pulmonary infective disease is this something that should be offered to parents?
We have no date to my knowledge in babies on the use of this type of dosing but it comes down to a question of what is the alternative? If a patient is dying on the ventilator are we at the point of knowledge here that it is worth offering the family this treatment? One could do so with full disclosure about the lack of neonatal data both for effectiveness and safety. Or do you fall on the side of it could be harmful and expedite death so should not be used. If you use it though and wait till the patient is in extremus on 100% oxygen might it be too late? Do parents have the right to know when they ask the question “is there anything else you can do?” For me I think the answer is that there should be a discussion with this evolving research out there. I am comfortable with it as long as the parents understand the potential for it to make things worse and shorten their time with their child. Alternatively if they choose not to that is their prerogative but should they have the choice when the competing outcome is death?
I can’t tell you whether you should or shouldn’t offer this in your institution but my suspicion is that you will be discussing this among colleagues before long. Who knows you might just one day say you saw it here first!
Thanks John M for the inspiration and keep sending those articles!
If you work in NICU you will have seen many babies who have passed through the stages of apnea, weaned off respiratory support and have reached a sufficient weight for discharge but alas will just not feed. Different strategies have been employed to get these infants feeding that rely in many cases on a cue based approach but in the end there are some that just won’t or can’t do it. Many of these babies will be sent home either with NG feedings or if it appears to be a more long term situation a gastrostomy tube. For this blog post I am going to present to you some novel research that suggests there may be another way to approach this and would like to thank one of the followers of my social media for alerting me to this work. You know who you are as the saying goes!
This was an open label Phase 0 trial (few patients as a pilot) using taVNS to help improve feeding in ex-preterm or 3 recovering from HIE infants who were now past term and all headed towards a gastrostomy tube. The hospital carrying out the study entitled Transcutaneous Auricular Vagus Nerve Stimulation-Paired Rehabilitation for Oromotor Feeding Problems in Newborns: An Open-Label Pilot Study by Badran BW et al did not come out of thin air. Prior research in adult patients recovering from stroke found in multiple studies (all referenced in the paper) that motor stimulation accompanied by VNS improves motor function recovery. The objective here then was to see if stimulation of the auricular nerve along with assessment and motor treatments from an occupational therapist once a day could help improve feeding and avoid GT placement. The trial overview is as shown below.
The centre in which the study was done had a historical rate in this population of <10% of such patients avoiding a GT (all reaching term equivalent age and not showing an improvement in feeds). This was demonstrated in previous work by at the Medical University of South Carolina (MUSC). “Preterm infants who have not reached full PO feeds by 40-week gestational age (GA) and/or after 40 days of attempting PO feeds have a >90% chance of eventually needing G-tube implantation to achieve full enteral feeds (Ryan and Gehle, 2019).”
The Intervention
taVNS was done once a day during a bottle feed and timed with observed suckling and swallowing by an OT. The stimulation was stopped during a pause in feeding.
As you read this you may be concerned about side effects (as I was) of passing an electrical current to the ear and stimulating the auricular branch of the vagus nerve. This has been shown in other work to activate both afferent and efferent pathways of the vagus nerve and enhance plasticity and functional motor recovery. Could you then apply the same to improving development of the motor pathways of the preterm newborn or patient recovering from HIE? The authors examined skin irritation, pain scores and incidence of bradycardia before and during feeding while stimulation was occurring and found no difference in any of the measures. In order to minimize pain the authors increased the current by 0.1 mA until they perceived stimulation by change in facial expression, shrugging or fidgety movements. In the event of an increase in pain scoring by 3 the dose was decreased by the same amount. in the end the intervention was deemed safe without any adverse effects.
The primary outcome was ability to increase and maintain full daily PO intake for 4 days (>120 mL/kg/d and maintain a weight gain of >20 g/day until discharge.
Why you should care about the results
If you work in a hospital like mine you would probably find that once the discussion about a GT placement begins, few miraculously avoid it. In this study they found that 8 of the 14 patients or 57% avoided the GT. Their historical achievement in this regard was <10%. This could be by chance of course since the study is a small one but when looking at the PO intake between non-responders and responders they demonstrate the following.
The authors found no statistically significant increase in the non-responders after the taVNS in PO feeds but also note there were three infants born to mothers with diabetes in this group. I have commented before on the effect of diabetes on successful feeding so this certainly could have affected the success of this group. If you look at the change over time in the responder group they look graphically like there was an upwards trend in the feeding ability prior to the intervention although the increase or slope of the improvement due to small numbers was not significant. The takeoff in feeding afterwards was.
The findings in this study are extremely exciting to me. As units across the globe struggle with patient flow, one of the most common reasons for these patients to stay in hospital is no longer BPD or apnea but inability to feed. The idea that such a simple intervention that is done once daily for 30 minutes might influence the development of feeding coordination in these at risk infants is phenomenal in terms of its impact on patient flow.
If you wonder about whether this is a one off study, there is a lot of active research in this area. A quick search of clinicaltrials.gov uncovers 61 studies on taVNS recruiting at the moment for a variety of ailments. In fact the next study is a Phase 1 trial aiming to recruit 40 patients and is underway. If interested the link to the study is here.