

A couple years back at the Canadian Pediatric Society annual meeting a discussion broke out about extubating infants to higher levels of CPAP. Conventional thinking had been to use levels between 5 – 8 cm H2O typically. I shared with the group the experience we had in Winnipeg (unpublished) of using higher levels from 9 -12 cm H2O with some degree of success in allowing earlier extubation. The group thought it was interesting but pointed out the lack of robust research in the area so were not so keen to “try it out”. Non-invasive positive pressure ventilation (NIPPV) has been used for some time in the neonatal world and has been compared to CPAP for extubation success and found to be superior as in this review Comparison of Complications and Efficacy of NIPPV and Nasal CPAP in Preterm Infants With RDS. In this review though as in others more typical CPAP levels are used so the question is whether the same efficacy would be seen with high level CPAP vs NIPPV.
Canadian Study to the Rescue
The study here is by Ahmad HA et al Comparison of High CPAP versus NIPPV in Preterm
Neonates: A Retrospective Cohort Study and seeks to answer this question albeit in a retrospective fashion. The study is not well controlled since it is retrospective but it may be the best we have for now. Over a 3 year period the authors examined the outcomes for babies trialed on high CPAP (hCPAP of at least 9 cm H20) vs NIPPV. In each case they looked at the first episode of use. The modalities could have been used for extubation or as a primary means of support. The primary outcome was failure of the modality as defined by either intubation or change to the other strategy within 7 days. A total of 53 infants received hCPAP vs 119 NIPPV. Why the big difference? Since this was retrospective and not randomized it was up to the individual practioner which modality they wanted to try. If the majority of the unit favoured NIPPV this is why there would be such a difference. Herein lies the benefit of the primary outcome as if “conventional wisdom” was wrong and the other modality would be better then we should see a greater movement to the other strategy or more intubations in one group suggesting superiority of one vs the other.
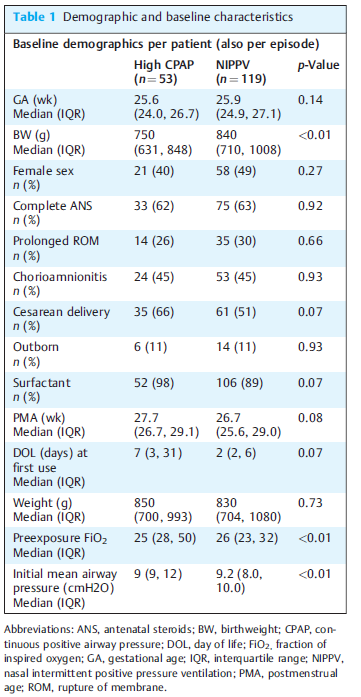
The groups however aren’t entirely equivalent at baseline. The babies in the hCPAP group are quite a bit smaller on the one hand which would favour the NIPPV group. On the other hand there is almost a significant difference in surfactant provision for the hCPAP arm which might favour the hCPAP group. The other thing also nearing statistical significance is when the intervention was trialed. The median time is 2 days for teh NIPPV group and 7 for hCPAP suggesting one may have been used more prophylactically and the other post extubation. Different strategies might make a difference to outcome? Also no infants received MIST or INSURE and all were started on traditional lower levels of CPAP prior to surfactant.
Results
The results tell an interesting story (I think) with the primary outcome being no different 62% in the hCPAP vs 55% with NIPPV. Looking at the patient outcomes in the figure from the paper one gets a little more detail and can surmise how people viewed the two modalities as a strategy and can see they were a bit different.
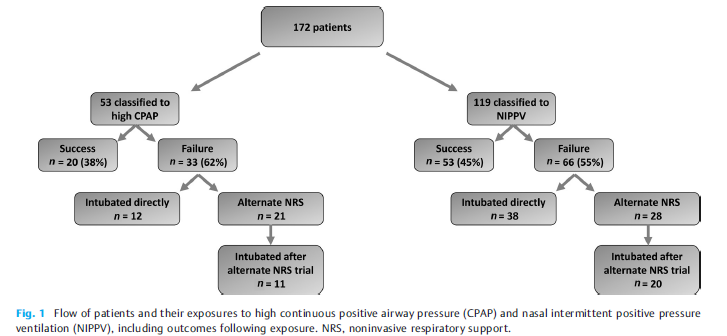
There seems to have more confidence in the unit with NIPPV as a way to prevent intubation. For those that failed hCPAP 12/33 were intubated as the next step (about a third) while the other 2/3 were trialed on NIPPV. Looking at those started out on NIPPV, 38/66 were intubated directly 58% or almost 2/3 while 28/66 were trialed on hCPAP. Of the ones trialed on hCPAP 20/28 or 71% were still intubated. Comparatively of those who were changed from nCPAP to NIPPV 11/21 were intubated or about 50%.
The authors find no difference in the primary outcome which is true. The problem of course with this analysis though is that there was no standardization with determining when one would choose to intubate. This issue can really play with the results. Let’s say for example that one Neonatologist really believes for the most part that NIPPV is the mode that can really prevent intubation more than hCPAP. It is conceivable that the reason in crossover intubations are less with NIPPV is that people were willing to tolerate a slightly higher pCO2 or a couple more apneas since they believe the modality is best and the infant will “get better soon”. On the other hand, infants already on NIPPV who are deteriorating might be intubated more readily as the attending might think “this hCPAP is a bunch of malarky”
It is worth mentioning that the incidence of air leak was no different between the two, nor was NEC or feeding intolerance from exposing the babies to such high pressures.
Conclusions
The study doesn’t “prove” anything. I don’t see it as a complete waste though as it does a number of things. It does show that small infants can be managed with hCPAP in NICU without any significant increase in complications. It also sets the stage for a couple future prospective trials I can see. Firstly, a trial of traditional CPAP vs hCPAP is needed as some units don’t have access to NIPPV or simply don’t use. The second is a prospective trial with clear parameters for failure between hCPAP and NIPPV.
Lastly, the authors ran the NIPPV and CPAP off ventilators in the units. The work of breathing would be potentially different with the use of devices solely designed for CPAP with fluidic flips. It would be important to use optimal devices for both modalities in such a trial and I for one can’t wait to see them.