
by All Things Neonatal | Mar 5, 2016 | Breastfeeding, Breastmilk, Uncategorized
I woke up this morning and as I do everyday, scanned the media outlets for news that would be of interest to you the reader. One such article today was about how breast milk may give babies a metabolic boost due to micro RNA present in the milk. This got me thinking about how natural a thing this breast milk is and how substances within interact with the baby receiving it. After that point I recalled writing about a challenge to the statement that breast milk is natural and thought you might like to see what I considered to be an outrageous piece of journalism from last year.
The premise of the article is that by reinforcing that breastfeeding is natural we may hamper initiatives to increase vaccination in many parts of the world and in particular North America I would think. The idea here is that if we firmly entrench in women’s heads that natural is better then this will strengthen the conviction that we should not vaccinate with these “man made” unnatural vaccines. I am sorry to be dramatic about this but I think the argument is ridiculous and in fact dangerous.
The Definition of Natural
“existing in nature and not made or caused by people : coming from nature”
From the Mirriam Webster dictionary
Breastfeeding satisfies this definition pure and simple and there is nothing that anyone should say to suggest otherwise no matter what the motive is. The shift from formula to breastfeeding has been predicated on this notion and a plethora of literature on the subject demonstrating reductions in such things as infections of many kinds, diarrhoea, atopic disease in the first year of life as examples. In my world of premature infants additional reductions in NEC, bloody stools, have been seen and more recently in some cases improved neurodevelopmental outcomes.
In this case of irresponsible journalism a better approach if you were wanting to use the natural argument with respect to vaccines is to promote just that.
Vaccines are Natural
Someone will no doubt challenge me on this point as it would be a fair comment to say that there are artificial substances added to vaccines but there is no question the organisms that we vaccinate against are natural.
Think about this for a moment. All of the vaccines out there are meant to protect us against organisms that exists in NATURE. These are all bacteria or viruses that have likely existed on this planet of ours for millions of years. They are found everywhere and in many cases what we are doing when we give such vaccines are providing parts of or weakened versions of these natural organisms in order for us the human to mount a protective response.
This protective response is NATURAL. If we didn’t vaccinate and came across the fully virulent pathogen in NATURE our bodies would do exactly what they do when a vaccine is given to us. Our immune system would mount a response to the organism and start producing protective antibodies. Unfortunately in many cases this will be too little too late as the bacteria or virus will cause it’s damage before we have a chance to rid ourselves of this natural organism.
This is the basis of vaccination. Allow our bodies a chance to have protection against an organism that we haven’t been exposed to yet so that when it comes we have a legion of antibodies just waiting to attach this natural organism.
CNN Didn’t Get It Right

In the article which is based on a paper entitled the Unintended Consequences of Invoking the “Natural” in Breastfeeding Promotion by Jessica Martucci & Anne Barnhill the authors admit that the number of families that this actually would impact is small. the question then is why publish this at all. Steering families away from thinking that breastfeeding is natural is wrong. Plain and simple.
If the goal is to improve vaccination rates, focus on informing the public about how NATURAL vaccinations actually are and don’t drag breastfeeding down in order to achieve such goals. As a someone who writes themselves I am well aware of how personal biases creep into everything we write. I am aware of the irony of that statement since it is clear what side of the argument I sit on. While I peruse CNN myself almost daily I think the editors either missed the larger message in this piece or perhaps felt the same way. A disclosure that “the opinions of the author do not necessarily represent those of the network” does not cut it for what I would consider responsible journalism in this case.

by All Things Neonatal | Mar 3, 2016 | antenatal steroids, Neonatal, Neonatology, Uncategorized
What a hard topic to resist commenting on. This was all over twitter and the general media this week after the New England Journal published the following paper; Antenatal Betamethasone for Women at Risk for Late Preterm Delivery. The fact that it is the NEJM publishing such a paper in and of itself suggests this is a top notch study…or does it?
In case the idea of giving antenatal steroids after 34 weeks sounds familiar it may be so as I wrote about the use of such an approach prior to elective c-section in a previous post; Not just for preemies anymore? Antenatal steroids for elective c-sections at term.
Is there a benefit to giving antenatal steroids from 34 0/7 – 36 5/7 weeks?
That is the central question the authors here sought to answer. Would women who had a high risk of delivering during this time period have less risk of a composite primary outcome of treatment in the first 72 hours (the use of continuous positive airway pressure or high-flow nasal cannula for at least 2 hours, supplemental oxygen with a fraction of inspired oxygen of at least 0.30 for at least 4 hours, extracorporeal membrane oxygenation, or mechanical ventilation) or stillbirth or neonatal death within 72 hours after delivery.
On the surface this seems like a very worthwhile set of outcomes to look at and the authors found in the end some pretty remarkable findings in a total of 2827 women randomized to placebo or betamethasone.
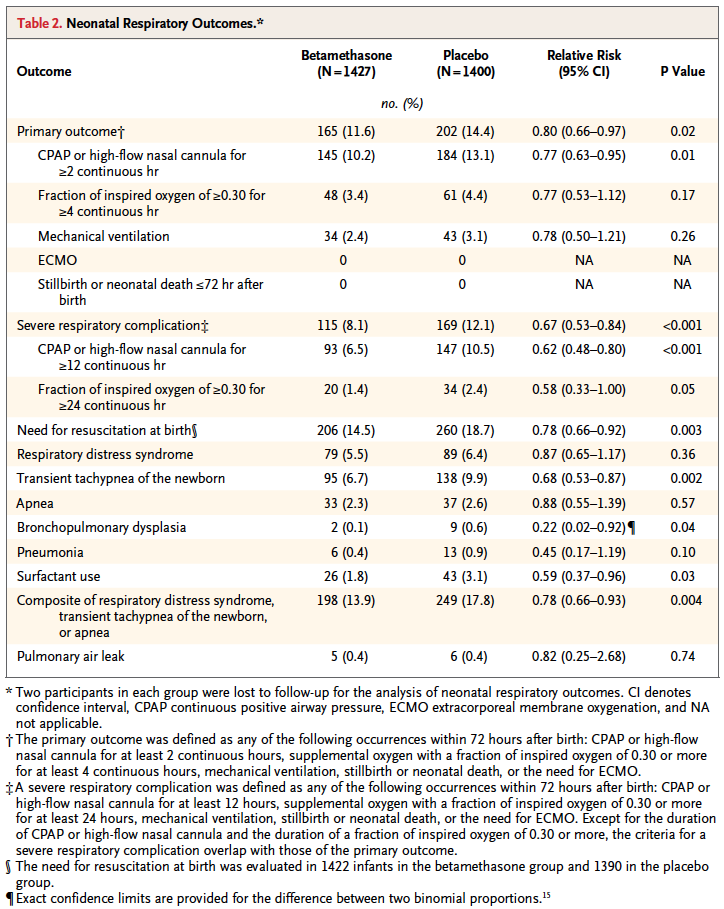
Looking at the results one sees that the primary outcome showed a significant difference with 2.8% less infants experiencing these conditions. However, when one looks at the details the only contributor to this difference was the need for CPAP or HFNC for >= 2 hours. A need for over 30% FiO2 for > 4 hours was also not different. No differences were noted in mechanical ventilation, ECMO, deaths whether stillbirths or neonatal deaths. Curiously, significant differences for secondary outcomes were seen with incidence of severe respiratory distress, and need for CPAP for over 12 hours.
These results are not truly that surprising at least for the primary outcome as if you asked most people working in the field of Neonatology how likely death, need for ECMO or even mechanical ventilation are from 34 – 36 weeks they would tell you not very likely. The other thing to consider is that the only real significant difference was noted for infants needing CPAP or HFNC for at least 2 hours. While this would interrupt maternal infant bonding, it wouldn’t necessarily mean an admission but rather in some cases observation and then transfer to the mother’s room.
Is it worth it?
To answer this question you need to know the best and worst case scenarios I suppose. Based on the reduction of 2.8%, you would need to treat 35 women with betamethasone to avoid the primary outcome but of course there is a range based on the confidence intervals around this estimate. The true estimate lies somewhere between 18 – 259 to avoid the outcome. Having said that, the estimate to avoid severe distress is 25 patients with a range of 16 – 56 which is pretty good value. In a perfect world I would probably suggest to women that there seems to be a benefit especially if one notes that in this study only 60% of the women received 2 dose of betamethasone so if rates of administration were higher one might expect and even better outcome. Ah but the world is not perfect….
There is only so much betamethasone to go around.
I find it ironic but the same day that this article came across my newsfeed so did a warning that we were about to run out of betamethasone vials in a certain concentration and would need to resort to another manufacturer but that supply may also run out soon as well. The instructions were to conserve this supply in the hospital for pregnant women.
In Canada as reported by the Canadian Neonatal Network in 2010, 38.1% of babies admitted to NICUs were below 34 weeks. Given that all babies would be admitted to NICUs at this gestational age and below that likely represents the percentage of births in those ages. An additional 31.8% or almost an equal number of babies will be born between 34 0/7 to 37 0/7 weeks meaning that if we were to start treating women who were deemed to be at risk of preterm delivery in that age range we would have a lot of potential women to choose from as these are the exact women in this strata who actually delivered early in Canada.
If I am forced to choose whether to give betamethasone to the mothers under 34 weeks or above when the resource we need is in scarce supply I don’t think there is much choice at all. Yes, this article comes from a reputable journal and yes there are some differences some of which are highly significant to consider but at least at this time my suggestion is to save the supply we have the babies who will benefit the most.
