It’s been a while since my last post. Like many centers across North America and worldwide the resuscitation of premature infants as young as 22 weeks is becoming more commonplace. Our own center is in the process of working towards coming up with evidence-based approaches to the care of these fragile infants. One of the questions that has long been asked is whether antenatal steroids really make a difference at these earliest gestational ages. The argument against effectiveness would be that the cards are just so stacked up against these preemies that even steroids may not help. Making matters worse is that the number of babies at this early gestational age included in antenatal steroid trials are extremely small making any conclusions difficult.
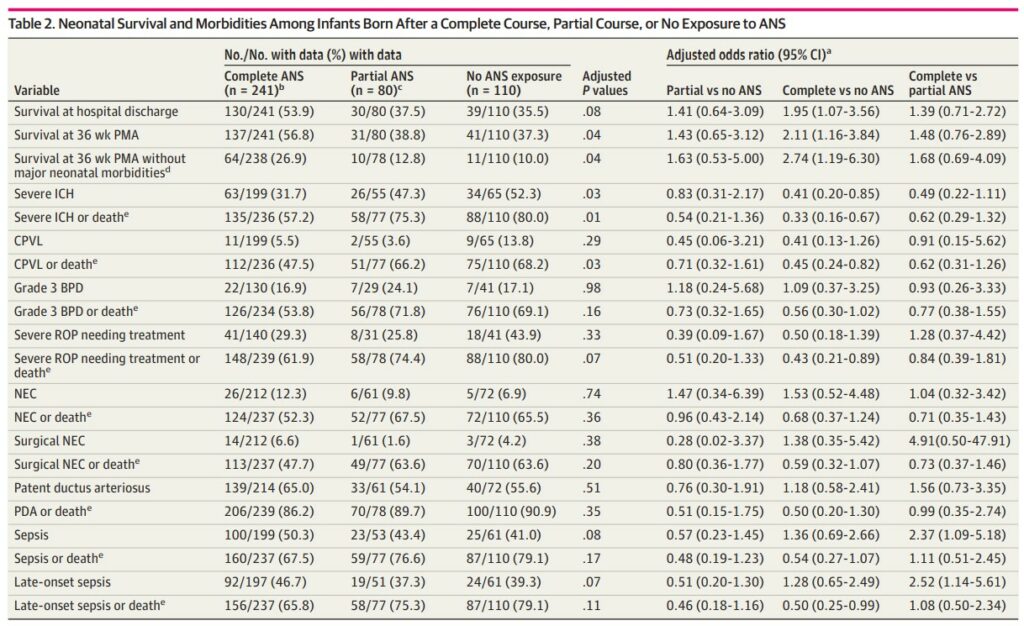
In short, the goal of the study was to look at survival and survival without major morbidities for infant born between 22 and 0 days to 23 weeks and 6 days gestational age who either received no antenatal steroids, 1 dose or 2 doses 24 hours apart. Only those mothers who received betamethasone were included and the doses were provided at either 21 or 22 weeks of gestation prior to delivery at 22 and 23 weeks of gestation. The study was retrospective and looked at NICHD neonatal research network data from January 1, 2016 to December 31, 2019. In comparison to all the previous prospective studies in existence which recruited less than 50 preterm infants this young this study managed to recruit 431 infants. In the groups analyzed, there were 25.5% infants who received no antenatal steroids, 18.6% infants receiving a partial course and 55.9% infants receiving complete antenatal steroids.
What did they find?
The authors found evidence that I believe will be reassuring to practitioners deciding whether to provide a course of steroids at these gestational ages. There are questions though that will be raised when looking at this data as well.
The data in table to show a number of interesting findings. Most notably a primary outcome of survival at hospital discharge was improved with a complete course of steroids but not with partial or none. Similarly there were reductions in severe intracranial hemorrhage and survival at 36 weeks postmenstrual age without major medical morbidities.
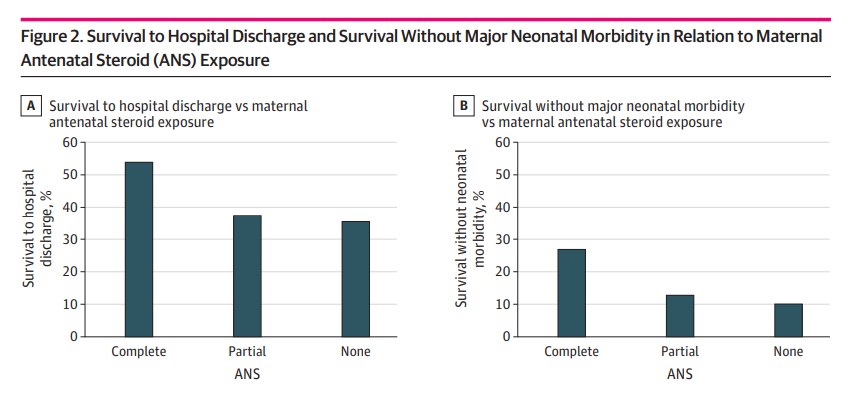
Figure 2 shows survival to hospital discharge and survival without major neonatal morbidities graphically. What one can more clearly see is that if you are going to give steroids the outcome is best if the mother receives both doses.
Challenges
On the one hand you might say that this is a slam dunk finding and we should be giving antenatal steroids to all women presenting at 21 and 22 weeks gestational age. I mentioned there would be questions and one of them will have to do with the avoidance of a repeat course of antenatal steroids. There is some literature that suggests repeat dosing of antenatal steroids later in pregnancy is associated with adverse developmental outcomes and also structural changes to the developing brain. This then leads the practitioner and a bit of a quagmire. If the woman presents at 21 or 22 weeks with threatened preterm labor do give her the steroids knowing that only a full course will help her versus waiting to see if she is truly in labor as you are considering whether you should save dosing for a later time in pregnancy. I have no doubt there will be some providers that we will hesitate to give the 1 course if that is their institution practice at this gestational age. This will not be an easy selection to make.
The other question that we will come up as we start to see a single dose antenatal steroid trials coming out is whether such infants will be included in prospective trials. The upcoming SNACS trial which we are participating in is one such trial that will include infants as young as these. It will be interesting to see if prospectively collected clinical trials with adequate numbers of such small infants will demonstrate similar findings that 2 doses really are required to make a meaningful reduction in adverse outcomes. As we have seen with many retrospective studies though such as this one the outcomes may in fact be different when you randomize patients in a prospective fashion.
For now I think the evidence as good as it is we will favor giving steroids to mother’s presenting at these gestational ages. Curious what you think?
As time goes by, I find myself gravitating to reviews of Canadian research more and more. We have a lot of great research happening in this country of ours and especially when I see an author or two I know personally I find it compelling to review such papers. Today is one of those days as the lead author for a paper is my colleague Dr. Louis here in Winnipeg. Let me put his mind at ease in case he reads this by saying that what follows is not a skewering of the paper he just published using Canadian Neonatal Network data (CNN). Over the last twenty years that I have had the privilege of working in the field of Neonatology we continue to discuss the same things when it comes to the PDA. Does it really cause problems or is it an association for many outcomes? Does treatment make a difference? If you treat then what should you use (ibuprofen, indomethacin, paracetamol)? When should you treat and if you treat early should it be in the first few days or right after birth using a prophylactic approach (provided within 12 hours of delivery)? It is the prophylactic approach which is the subject of this post!
Why treat prophylactically?
The TIPP trial reported the results in 2001 of the study whose goal was to determine if prophylactic indomethacin use could improve neurosensory impairment at 18 months by reducing rates of severe IVH. The results of the study are well known and showed that while the rates of severe IVH and PDA ligations were reduced through this approach, there was no actual effect on long term outcome. The use of this approach fell off after that for many years but recently resurfaced as some units in Canada opted to start the practice again as the two benefits seen above appeared to be worth using the approach. The thought from a family centred approach, was that eliminating the stress for families of informing them their tiny preterm infant had a serious intracranial bleed and potentially avoiding a surgical ligation with probably vocal cord impairment afterwards were good enough outcomes to warrant this practice. Having used this approach myself I have to admit one consequence is that indomethacin was so effective at closing the PDA most of the time that over time one begins to assume the PDA is in fact closed and is less likely to go hunting for one when the baby is misbehaving later on in their course. What if it didn’t close though? Are there any predictors that can increase our index of suspicion?
Answering the question
The CNN provides a large database to look retrospectively to answer such a question. In this article, the authors looked at a period from 2010 to 2015 including all infants < 28 weeks gestational age at birth yielding a very large sample of 7397 infants. Of these 843 or 12% received prophylactic indomethacin and from there a little over half (465) still had a PDA. From there, 367 received treatment with eventually 283 needing only medical, 11 having a PDA ligation and 73 having both medical and surgical closure. From this analysis so far I can tell you that providing prophylactic indomethacin certainly does not guarantee closure!
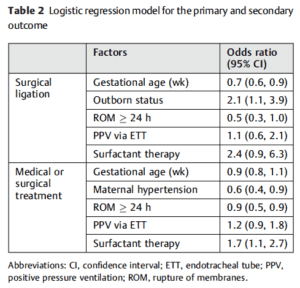
When a myriad of risk factors were put into logistic regression a number of interesting risk factors arose accounting for more of less risk of a PDA that needed surgical ligation despite prophylactic treatment. Much like all infants in the NICU, the risk for a persistent PDA was highest with declining GA. The combination of outborn status and short interval of ruptured membranes predicted higher risk. No doubt this is reflective of less frequent antenatal steroid use and even if provided time for it to work. Looking at medical or surgical treatment, surfactant therapy increased risk which may be explained by an improvement in oxygenation contributing to increased left to right shunting as PVR drops. Maternal hypertension and longer duration of rupture of membranes again play a role in reducing risk likely through the mechanism of the former increasing endogenous steroid production and the latter again allowing for steroids to be provided.
What can we learn from this paper?
I suppose the biggest benefit here is the realization that even with prophylactic indomethacin we are not assured of closure. In particular if there is a lack of antenatal steroid use or a stressed fetus one should be vigilant for the PDA. Interestingly, all of the risks seem to point towards antenatal steroid use. The bottom line then is that this reinforces what is already known and should be the focus of improvement strategies for centres. Increase the rate of antenatal steroid use and you will reduce the risk of a PDA even in the baby receives prophylactic indomethacin. I am happy to report that our centre has taken one step towards this goal by reinforcing to our Obstetrical colleagues that when they receive a call from a referring centre and have a woman who might be in labour it is better to err on the side of caution and just give the steroid course. If they are wrong on arrival then one can always repeat a course later on as we do although repeated courses of steroids are in and of themselves a contentious issue. What can your centre do to improve your results when it comes to antenatal steroid coverage?
In April of this year the ALPS trial results were published in the New England Journal of Medicine (Antenatal Betamethasone for Women at Risk for Late Preterm Delivery) and I took the time to review the paper at the time Antenatal Steroids After 34 weeks. Believe the hype? In the analysis I focused on an issue which was relevant at the time, being a shortage of betamethasone. In a situation when the drug of choice is in short supply I argued that while the benefits of giving steroid to women at risk of delivery between 34 0/7 to 36 6/7 weeks was there, if I had to choose (as I did at the time) I would save the doses for those at highest risk of adverse outcome. Since the blog post though a couple of things have come out in the literature that I believe are worth sharing as it could truly influence practice.
The American College of Obstetricians and Gynecologists, moved by the results of the ALPS trial issued the following recommendations (shortened in places).
Betamethasone may be considered in women with a singleton pregnancy between 34 0/7 and 36 6/7 weeks gestation at imminent risk of preterm birth within 7 days.
Monitoring of late preterms for hypoglycemia (already being done)
Do not give in the setting of chorioamnionitis.
Tocolysis or delayed delivery for maternal indications should not be done in order to to allow for administration of late preterm antenatal corticosteroids.
Do not provide if the pregnancy was already exposed to antenatal corticosteroids.
The exclusions above such as twins and triplets, diabetic pregnancies and previous receipt of steroids were included since the study had not included these patients. As the ACOG states in the summary, they will be reviewing such indications in the future and providing recommendations. I would imagine that if I were in a US based practice then this post might seem like old news since many centres would have started doing this. Given that the readers of this blog are based in many different countries around the globe and at least in Canada this has not become commonplace I thought it would be worth the update!
I posted the abstract for this review on my Facebook page the other day and it certainly garnered a lot of interest. Some of my readers indicated the practice is already underway. I was curious what a systematic review would reveal about the topic since the ACOG was so moved by the ALPS study in particular. Perusing through the Society of Obstetricians and Gynecologists of Canada (SOGC) I can’t find any commentary on this topic and certainly there are no new clinical practice guidelines since the ALPS study landed on my desktop.
Here are the pooled results from 6 trials:
Lower risk of RDS (relative risk 0.74, 95% confidence interval 0.61 to 0.91)
Mild RDS (0.67, 0.46 to 0.96)
Moderate RDS (0.39, 0.18 to 0.89)
Severe RDS (0.55, 0.33 to 0.91)
Transient tachypnea of the newborn (0.56, 0.37 to 0.86)
Shorter stay on a neonatal intensive care unit (−7.64 days, −7.65 to −7.64)
So across the board patients who receive antenatal steroids after 34 weeks still continue to see a benefit but looked at a different way the real benefit of the intervention is easier to see and that is through looking at the number needed to treat (NNT). For those of you who are not familiar with this analysis, this looks at how many patients one would need to treat in order to avoid the outcome in 1 patient.
For the outcomes above as an example the NNT for RDS overall is about 59 while for TTN 31 patients. Severe RDS which is less common after 34 weeks you might expect to require more patients to treat to help 1 avoid the outcome and you would be correct. That number is 118 patients. It is interesting to look at the impact of steroids in pregnancies below 34 weeks (taken from the Cochrane review on the subject) as the NNT there is 23! If you were to break these benefits down from 23-27 weeks though where the risk of RDS is quite high the NNT would be even lower. Steroids help, no question to reduce neonatal complications but as you can see even when there is a reduction in risk for various outcomes, the number of women you need to treat to get one good outcome is quite different.
Some Discussion With Obstetrics Is Needed Here
As you read through this post you may find yourself saying “Who cares? if there is a benefit at all most moms would say give me the steroids!” The issue here has to do with long term outcome. To put it simply, we don’t know for this type of patient. We know clearly that for patients at high risk of adverse outcomes eg. 24 week infant, the reduction in risks of infection, NEC, PDA, BPD etc from receiving antenatal steroids translates into many long term benefits. What about the patient who say is 35 weeks and would have none of those risks? Yes we are avoiding some short term outcomes that let’s be honest can be scary for a new parent but what are we trading this benefit for. The concern comes from what we know about steroids impact on the developing brain. Steroids lead to a developmental arrest but in very preterm infants there is no doubt that the protective effect on all of these other outcomes more than offsets whatever impact there is there. Incidentally I wrote about this once before and the section of interest appears at the end of the relevant post Not just for preemies anymore? Antenatal steroids for elective c-sections at term. In the absence of these other conditions could there be a long term impact in babies 34 – 36 6/7? My suspicion is that the answer is no but discussion is needed here especially in the absence of an endorsement by our Canadian SOGC. Having said all that I expect the future will indeed see an expansion of the program but then I do hope that someone takes the time to follow such children up so we have the answer once and for all.
What a hard topic to resist commenting on. This was all over twitter and the general media this week after the New England Journal published the following paper; Antenatal Betamethasone for Women at Risk for Late Preterm Delivery. The fact that it is the NEJM publishing such a paper in and of itself suggests this is a top notch study…or does it?
Is there a benefit to giving antenatal steroids from 34 0/7 – 36 5/7 weeks?
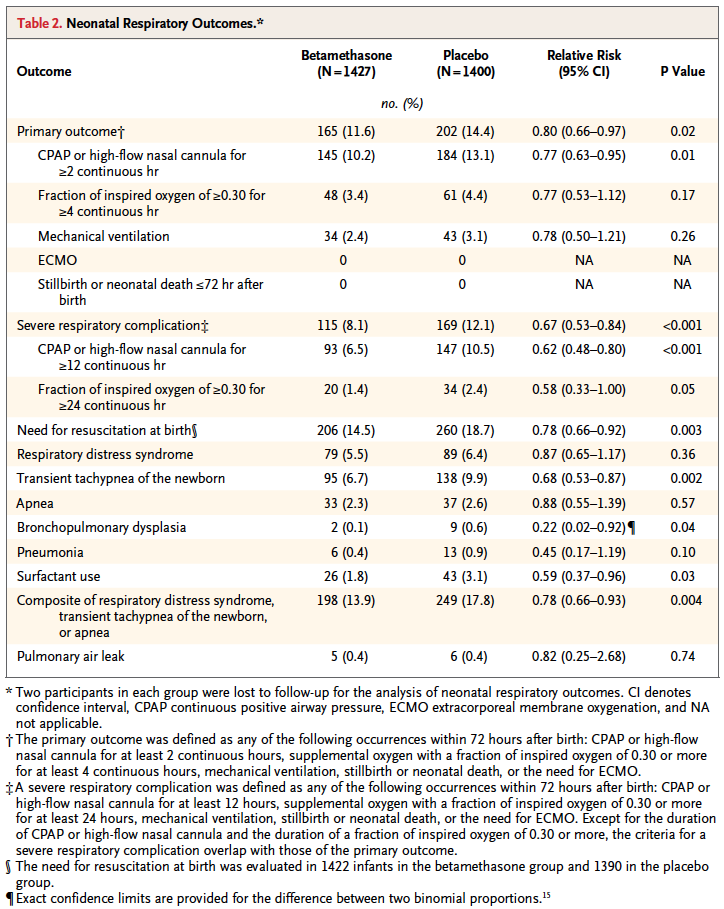
That is the central question the authors here sought to answer. Would women who had a high risk of delivering during this time period have less risk of a composite primary outcome of treatment in the first 72 hours (the use of continuous positive airway pressure or high-flow nasal cannula for at least 2 hours, supplemental oxygen with a fraction of inspired oxygen of at least 0.30 for at least 4 hours, extracorporeal membrane oxygenation, or mechanical ventilation) or stillbirth or neonatal death within 72 hours after delivery.
On the surface this seems like a very worthwhile set of outcomes to look at and the authors found in the end some pretty remarkable findings in a total of 2827 women randomized to placebo or betamethasone.
Looking at the results one sees that the primary outcome showed a significant difference with 2.8% less infants experiencing these conditions. However, when one looks at the details the only contributor to this difference was the need for CPAP or HFNC for >= 2 hours. A need for over 30% FiO2 for > 4 hours was also not different. No differences were noted in mechanical ventilation, ECMO, deaths whether stillbirths or neonatal deaths. Curiously, significant differences for secondary outcomes were seen with incidence of severe respiratory distress, and need for CPAP for over 12 hours.
These results are not truly that surprising at least for the primary outcome as if you asked most people working in the field of Neonatology how likely death, need for ECMO or even mechanical ventilation are from 34 – 36 weeks they would tell you not very likely. The other thing to consider is that the only real significant difference was noted for infants needing CPAP or HFNC for at least 2 hours. While this would interrupt maternal infant bonding, it wouldn’t necessarily mean an admission but rather in some cases observation and then transfer to the mother’s room.
Is it worth it?
To answer this question you need to know the best and worst case scenarios I suppose. Based on the reduction of 2.8%, you would need to treat 35 women with betamethasone to avoid the primary outcome but of course there is a range based on the confidence intervals around this estimate. The true estimate lies somewhere between 18 – 259 to avoid the outcome. Having said that, the estimate to avoid severe distress is 25 patients with a range of 16 – 56 which is pretty good value. In a perfect world I would probably suggest to women that there seems to be a benefit especially if one notes that in this study only 60% of the women received 2 dose of betamethasone so if rates of administration were higher one might expect and even better outcome. Ah but the world is not perfect….
There is only so much betamethasone to go around.
I find it ironic but the same day that this article came across my newsfeed so did a warning that we were about to run out of betamethasone vials in a certain concentration and would need to resort to another manufacturer but that supply may also run out soon as well. The instructions were to conserve this supply in the hospital for pregnant women.
In Canada as reported by the Canadian Neonatal Network in 2010, 38.1% of babies admitted to NICUs were below 34 weeks. Given that all babies would be admitted to NICUs at this gestational age and below that likely represents the percentage of births in those ages. An additional 31.8% or almost an equal number of babies will be born between 34 0/7 to 37 0/7 weeks meaning that if we were to start treating women who were deemed to be at risk of preterm delivery in that age range we would have a lot of potential women to choose from as these are the exact women in this strata who actually delivered early in Canada.
If I am forced to choose whether to give betamethasone to the mothers under 34 weeks or above when the resource we need is in scarce supply I don’t think there is much choice at all. Yes, this article comes from a reputable journal and yes there are some differences some of which are highly significant to consider but at least at this time my suggestion is to save the supply we have the babies who will benefit the most.