
by All Things Neonatal | Oct 13, 2016 | preemie, Prematurity
I had a chance recently to drive a Tesla Model S with autopilot. Taking the car out on a fairly deserted road near my home I flicked the lever twice to activate the autopilot feature and put my hands behind my head while the vehicle took me where I wanted to go.  As I cruised down the road with the wheel automatically turning with the curves in the road and the car speeding up or slowing down based on traffic and speed limit notices I couldn’t help but think of how such technology could be applied to medicine. How far away could the self driving ventilator or CPAP device be from development?
As I cruised down the road with the wheel automatically turning with the curves in the road and the car speeding up or slowing down based on traffic and speed limit notices I couldn’t help but think of how such technology could be applied to medicine. How far away could the self driving ventilator or CPAP device be from development?
I have written about automatic saturation adjustments in a previous post but this referred to those patients on mechanical ventilation. Automatic adjustments of FiO2. Ready for prime time? Why is this goal so important to attain? The reasoning lies in the current design trends in modern NICUs. We are in the middle of a large movement towards single patient room NICUs which have many benefits such as privacy which may lead to enhanced breastfeeding rates and increased parental visitation. The downside, having spoken to people in centres where such designs are already in place is the challenge nursing faces when given multiple assignments of babies on O2. If you have to go from room to room and a baby is known to be labile in their O2 saturations it is human nature to turn the O2 up a little more than you otherwise would to give yourself a “cushion” while you are out of the room. I really don’t fault people in this circumstance but it does pose the question as to whether in a few years we will see a rise in oxygen related tissue injury such as CLD or ROP from such practice. In the previous post I wrote about babies who are ventilated but these infants will often be one to one nursed so the tendency to overshoot the O2 requirements may be less than the baby on non- invasive ventilation.
A System For Controlling O2 Automatically For Infants on Non-Invasive Ventilation
This month in Archives Dr. Dargaville and colleagues in Australia provide two papers, the first demonstrating the validation of the mathematical algorithm that they developed to control O2 and the second a clinical report outlining how well the system actually performed on patients. The theoretical paper Development and preclinical testing of an adaptive algorithm for automated control of inspired oxygen in the preterm infant. is a challenge to comprehend although validates the approach in the end while the clinical paper at least for me was easier to digest Clinical evaluation of a novel adaptive algorithm for automated control of oxygen therapy in preterm infants on non-invasive respiratory support.
The study was really a proof of concept with 20 preterm infants (mean GA 27.5 weeks, 8 days of age on average) included who each underwent two hours of manual control by nursing to keep saturations between 90-94% and then 4 hours of automated control (sats 91 – 95%) then back to manual for two hours. The slightly shifted ranges were required due to the way in which midpoint saturations are calculated. The essential setup was a computer equipped with an algorithm to make adjustments in FiO2 using an output to a motor that would adjust the O2 blender and then feedback from an O2 saturation monitor back to the computer. The system was equipped with an override to allow nursing to adjust in the event of poor signal or lack of response to the automatic adjustment.
The results though demonstrate that the system works and moreover does a very good job! The average percentage of time that the saturations were in the target range were significantly better with automated control (81% automated, 56% manual). As well as depicted in the following figure the amount of time spent in both hypoxic and hyperoxic ranges was considerable with manual control but non-existent on either tail with automated control (defined as < 85% or > 98% where black bars are manual control and white automatic).
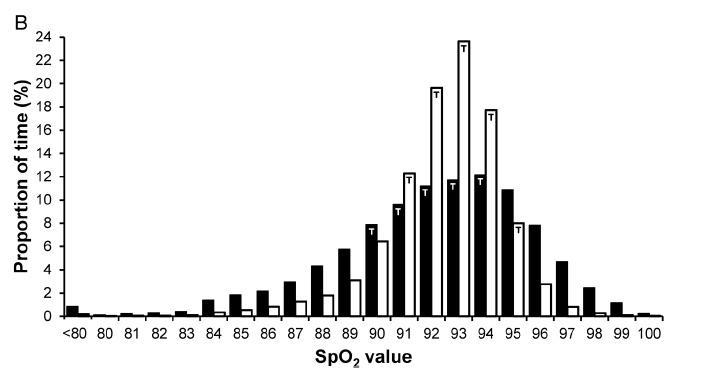
From the figure you can see that the amount of time the patients are in target range are much higher with automatic control but is this simply because in addition to automatic control, nurses are “grabbing the wheel” and augmenting the system here? Not at all.
“During manual control epochs, FiO2 adjustments of at least 1% were made 2.3 (1.3–3.4) times/hour by bedside staff. During automated control, the minimum alteration to FiO2 of 0.5% was being actuated by the servomotor frequently (9.9 alterations/min overall), and changes to measured FiO2 of at least 1% occurred at a frequency of 64 (49–98) /hour. When in automated control, a total of 18 manual adjustments were made in all 20 recordings (0.24 adjustments/hour), a reduction by 90% from the rate of manual adjustments observed during manual control (2.3/hour).”
From the above quote from the paper it is clear that automated control works to keep the saturation goal through roughly 7 X the number of adjustments than nursing makes per hour. It is hard to keep up with that pace when you have multiple assignments but that is what you need I suppose! The use of the auto setting here reduced the amount of nursing interventions to adjust FiO2 by 90% and yields tighter control of O2 saturations.
Dare to Dream
Self driving oxygen administration is coming and this proof of concept needs to be developed and soon into a commercial solution. The risk of O2 damage to developing tissues is too great not to bring this technology forward to the masses. As we prepare to move into a new institution I sincerely hope that this solution arrives in time but regardless I know our nurses and RRTs will do their best as they always do until such a device comes along. When it does imagine all of the time that could be devoted to other areas of care once you were able to move away from the non-invasive device!

by All Things Neonatal | Jun 15, 2016 | Uncategorized, ventilation
As the saying goes the devil is in the details. For some years now many centres worldwide have been publishing trials pertaining to high flow nasal cannulae (HFNC) particularly as a weaning strategy for extubation. The appeal is no doubt partly in the simplicity of the system and the perception that it is less invasive than CPAP. Add to this that many centres have found less nasal breakdown with the implementation of HFNC as standard care and you can see where the popularity for this device has come from.
This year a contact of mine Dominic Wilkinson on twitter (if you don’t follow him I would advise having a look!) published the following cochrane review, High flow nasal cannula for respiratory support in preterm infants. The review as with most cochrane systematic reviews is complete and comes to a variety of important conclusions based on 6 studies including 934 infants comparing use of HFNC to CPAP.
1. No differences in the primary outcomes of death (typical RR 0.77, 95% CI 0.43 to 1.36; 5 studies, 896 infants) or CLD.
2. After extubation to HFNC no difference in the rate of treatment failure (typical RR 1.21, 95% CI 0.95 to 1.55; 5 studies, 786 infants) or reintubation (typical RR 0.91, 95% CI 0.68 to 1.20; 6 studies, 934 infants).
3. Infants randomised to HFNC had reduced nasal trauma (typical RR 0.64, 95% CI 0.51 to 0.79; typical risk difference (RD) -0.14, 95% CI -0.20 to -0.08; 4 studies, 645 infants).
4. Small reduction in the rate of pneumothorax (typical RR 0.35, 95% CI 0.11 to 1.06; typical RD -0.02, 95% CI -0.03 to -0.00; 5 studies 896 infants) in infants treated with HFNC but the RR crosses one so this may be a trend at best.
If one was to do a quick search for the evidence and found this review with these findings it would be very tempting to jump on the bandwagon. Looking at the review a little closer though there is one line that I hope many do not miss and I was happy to see Dominic include it.
“Subgroup analysis found no difference in the rate of the primary outcomes between HFNC and CPAP in preterm infants in different gestational age subgroups, though there were only small numbers of extremely preterm and late preterm infants.”
In his conclusion he further states:
Further evidence is also required for evaluating the safety and efficacy of HFNC in extremely preterm and mildly preterm subgroups, and for comparing different HFNC devices.
With so few ELBW infants included and with these infants being at highest risk of mortality and BPD our centre has been reluctant to adopt this mode of respiratory support in the absence of solid evidence that it is equally effective to CPAP in these smallest infants. A big thank you to our Respiratory Therapy Clinical Specialist for harping on this point over the years as the temptation to adopt has been strong as other centres turn to this strategy.
Might Not Be So Safe After All
Now do not take what I am about to say as a slight against my twitter friend. The evidence to date points to exactly what he and his other coauthors concluded but with the release of an important paper in May by Taka DK et al, I believe caution is needed when it comes to our ELBW infants.
High Flow Nasal Cannula Use Is Associated with Increased Morbidity and Length of Hospitalization in Extremely Low Birth Weight Infants
This paper adds to the body of literature on the topic as it truly focuses on the outcome of infants < 1000g. While this study is retrospective in nature it does cover a five year period and examines important outcomes of interest to this population.
The primary outcome in this case was death or BPD and whether HFNC was used alone or with CPAP, this was more frequent than when CPAP was used alone. Other important findings were the need for multiple and longer courses of ventilation in those who received at least some HFNC. In these times of overburdened health care systems with goals of improving patient flow, it is also worth noting that there was a significant prolongation of length of stay with use of HFNC or HFNC and CPAP.
One interesting observation was that the group that fared the worst across the board was the combination of CPAP and HFNC rather than HFNC alone.
|
CPAP (941) |
HFNC (333) |
HFNC +/- CPAP (1546) |
| CPAP d (median, IQR) |
15(5-28) |
|
7 (1-19) |
| HFNC d (median, IQR) |
14(5-25) |
13 (6-23) |
| HFNC +/- CPAP |
15 (5-28) |
14(5-25) |
26 (14-39) |
| BPD or death % |
50.40% |
56.80% |
61.50% |
| BPD % |
42.20% |
52.20% |
59.00% |
| Multiple ventiation courses |
51.10% |
53.10% |
64.70% |
| More than 3 vent courses |
17.60% |
21.00% |
29.40% |
| Ventilator d (median, IQR) |
18(5-42) |
25 (6-52) |
30 (10-58) |
I believe the finding may be explained by the problem inherent with retrospective studies. This is not a study in which patients were randomized to either CPAP, HFNC or CPAP w/HFNC. If that were the case one would expect lung pathologies and severity of illness to even ou,t such that differences between groups might be explained by the difference in treatments. In this study though we are looking though the rearview mirror so to speak. How could we account for the combination being worse than the HFNC alone? I suspect it relates to the severity of lung disease. The babies who were placed on HFNC and did well on it might have had less severe chronic changes. What might be said about those that had the combination? Well, one could postulate that there might be some who were extubated to HFNC and collapsed needing escalation to CPAP and then failing that therapy were reintubated. Another explanation could be those babies who were placed on CPAP after extubation and transitioned before their lungs were ready to HFNC may have failed and lost FRC thereby going back to CPAP and possibly intubation. Exposure in either circumstance to HFNC would therefore put them at risk of further positive pressure ventilation and subsequent further lung injury. The babies who could tolerate transition to HFNC without CPAP might be intermediary in their outcomes (as they were found to be) as they lost FRC but were able to tolerate it but consumed more calories leaving less for growth and repair of damaged tissue leading to prolonged need for support.
Either way, the use of HFNC was found to lead to worse outcomes and in the ELBW infant should be avoided as routine practice pending the results of a prospective RCT on the subject.
Is it a total ban though?
As with many treatments that one should not consider standard of care there may be some situations where there may be benefit. The ELBW infant with nasal breakdown from CPAP that despite excellent nursing and RRT attention continues to demonstrate tissue damage is one patient that could be considered. The cosmetic implications and potential for surgical correction at a later date would be one reason to consider a trial of HFNC but only in the patient that was close to being able to come off CPAP. In the end I believe that if a ELBW infant needs non invasive pressure support then it should be with CPAP but as there saying goes there may be a right time and a place for even this modality.

by All Things Neonatal | May 19, 2016 | resuscitation, Uncategorized
As I was preparing to settle in tonight I received a question from a reader on my Linkedin page in regards to the use of sustained inflation (SI) in our units. We don’t use it and I think the reasons behind it might be of interest to others. The concept of SI is that by providing a high opening pressure of 20 – 30 cm H2O for anywhere from 5 to 15 seconds one may be able to open the “stiff” lung of a preterm infant with RDS and establish an adequate functional residual capacity. Once the lung is open, it may be possible in theory to keep it open with ongoing peep at a more traditional level of 5 – 8 cm of H20.
The concept was tested 25 years ago by Vyas et al in their article Physiologic responses to prolonged and slow-rise inflation in the resuscitation of the asphyxiated newborn infant. In this study, 9 newborn infants were given a relatively short 5 second sustained inflation and led to earlier and larger lung volumes with good establishment of FRC. Like many trials in Neonatology though sceptics abound and here we are 25 years later still discussing the merits of this approach.
As I have a warm place in my heart for the place that started my professional career whenever I come across a paper published by former colleagues I take a closer look. Such is the case with a systematic review on sustained inflation by Schmolzer et al. The inclusion criteria were studies of infants born at <33 weeks. Their article provides a wonderful assessment of the state of the literature on the topic and I would encourage you to have a look at it if you would like a good reference to keep around on the topic. What it comes down to though is that there are really only four randomized human studies using the technique and in truth they are fairly heterogeneous in their design. They vary in the length of time an SI was performed (5 – 20 seconds), the pressures used (20 – 30 cm H2O), single or multiple SIs and lastly amount of oxygen utilized being 21 – 100%. In fact three of the four studies used either 100% or in one case 50% FiO2 when providing such treatments.
What Did They Show?
This is where things get interesting. SI works in the short term by reducing the likelihood that an infant will need mechanical ventilation at 72 hours with a number needed to treat of only 10! In medicine we normally would embrace such results but sadly the results do not translate into long term benefits as the rate of BPD, mortality and the combined outcome do not remain significant. Interestingly, the incidence of a symptomatic PDA needing treatment with either a medical or surgical approach had a number needed to harm of 11; an equally impressive number but one that gives reason for concern. 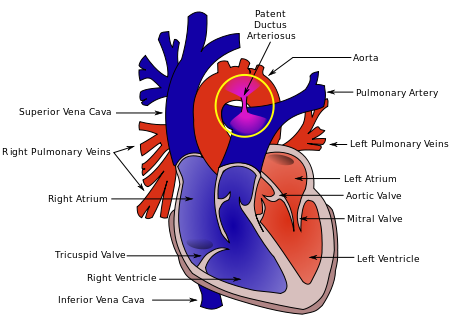 As the authors speculate, the increased rate of PDA may be in fact related to the good job that the SI does in this early phase. By establishing an open lung and at an earlier time point it may well be that there is an accentuation in the relaxation of the pulmonary vasculature and this leads to a left to right shunt that by being hemodynamically significant helps to stent the ductus open at a time when it might otherwise be tending to close. This outcome in and of itself raises concern in my mind and is the first reason to give me reason to pause before adopting this practice.
As the authors speculate, the increased rate of PDA may be in fact related to the good job that the SI does in this early phase. By establishing an open lung and at an earlier time point it may well be that there is an accentuation in the relaxation of the pulmonary vasculature and this leads to a left to right shunt that by being hemodynamically significant helps to stent the ductus open at a time when it might otherwise be tending to close. This outcome in and of itself raises concern in my mind and is the first reason to give me reason to pause before adopting this practice.
Any other concerns?
Although non-significant there was a trend towards increased rates of IVH in the groups randomized to SI. There is real biologic plausibility here. During an SI the increased positive pressure in the chest could well simulate a similar effect to a pneumothorax and impede the passive drainage of blood from the head into the thorax. In particular, longer durations and/or frequent SIs could increase such risk. Given the heterogeneous nature of these studies it is difficult to know if they all had been similar in providing multiple SIs could we have seen this cross over to significant?
I believe the biggest concern in all of this though is that I would have a very hard time applying the results of these studies to our patient population. The systematic review addresses the question about whether SI is better than IPPV as a lung recruitment strategy in the preterm infant with respiratory distress. I have to say though we have moved beyond IPPV as an initial strategy in favour of placement of CPAP on the infant directly after birth. The real question in my mind is whether providing brief periods of SI followed by CPAP of +6 to +8 is better than placement on CPAP alone as a first strategy to establish good lung volumes.
If I am to be swayed by the use of SI someone needs to do this study first. The possibility of increasing the number of hemodynamically significant PDAs and potentially worsening IVH without any clear reduction in BPD is definitely placing me firmly in the camp of favouring the CPAP approach. Having said all that, the work by the Edmonton group is important and gives everyone a glimpse into what the current landscape is for research in this field and opens the door for their group or another to answer my questions and any others that may emerge as this strategy will no doubt be discussed for years to come.

by All Things Neonatal | Feb 25, 2016 | preemie, Prematurity, Uncategorized
It is hard to believe but All Things Neonatal is a year old. When I started this little concept I had no idea what was to come but am delighted with where it has gone. While the Blog site itself has about 200 followers, the Facebook page is home to nearly 4200 followers with twitter accounting for over 500 more. What began as a forum for me to get some thoughts off my chest about neonatal topics or articles of interest has morphed into a place to create change. As I look back over the last year I thought I would update the readers of this page and other social media platforms what the outcome has been for some of the ideas that I have brought forward. We have implemented some of these suggestions into our own unit practices, so without further ado here are the updates for some (but not all!) of the changes we have introduced.
Articles pertaining to use of Telehealth in all aspects of medicine are becoming commonplace.  Locally we have seen expansion of rural sites that can connect with us and a strong desire by existing sites to connect via telehealth for a variety of reasons. While the thrust of the program was to deliver advice to rural practitioners and support our level I and II units we have found such support leading to possibilities we had not dreamed of. Initial discussions via telehealth and in person have occurred examining whether such treatments as CPAP stabilization and NG feedings could be done in these sites. Being able to provide such care will no doubt lead to more stable infants being transported to our site and moreover the possibility of moving the care for infants needing only gavage feeding back to their home communities. Who knows what the future will hold for us as we also look forward to the hiring of a telehealth coordinator for NICU!
Locally we have seen expansion of rural sites that can connect with us and a strong desire by existing sites to connect via telehealth for a variety of reasons. While the thrust of the program was to deliver advice to rural practitioners and support our level I and II units we have found such support leading to possibilities we had not dreamed of. Initial discussions via telehealth and in person have occurred examining whether such treatments as CPAP stabilization and NG feedings could be done in these sites. Being able to provide such care will no doubt lead to more stable infants being transported to our site and moreover the possibility of moving the care for infants needing only gavage feeding back to their home communities. Who knows what the future will hold for us as we also look forward to the hiring of a telehealth coordinator for NICU!
This has been one of my favourite topics to write about. The ability to sample CO2 from an area near the carina has been demonstrated to be accurate and to save pokes in the long run.  Since writing this piece we have tried it on several babies by using a double lumen tube and found the results to be as accurate as described in the Israeli papers. In practice though, secretions have proved difficult to handle for longer periods of use as they can travel up the sampling lines and damage the filters in the analyzers. A costly issue to deal with that we are currently trying to solve. Being able to continuously sample CO2 and adjust ventilation without drawing frequent blood gases is somewhat of a dream for me and we will continue to see how we can go about making this an established practice but there is work to be done!
Since writing this piece we have tried it on several babies by using a double lumen tube and found the results to be as accurate as described in the Israeli papers. In practice though, secretions have proved difficult to handle for longer periods of use as they can travel up the sampling lines and damage the filters in the analyzers. A costly issue to deal with that we are currently trying to solve. Being able to continuously sample CO2 and adjust ventilation without drawing frequent blood gases is somewhat of a dream for me and we will continue to see how we can go about making this an established practice but there is work to be done!
I think most people in Winnipeg would say the answer is yes. On this front two major positive changes have occurred in the last year in this regard.  The first is that through a generous donation and the blessing of our health region we have been able to expand the use of donor breast milk from < 1250g for a two week period to < 1500g for a one month period. This wonderful change came about after much effort and was celebrated in December as we not only expanded the eligibility criteria but partnered with the NorthernStar Mother’s Milk Bank to provide donor milk to Manitobans (Manitobans Now Able To Support Premature Infants Through Donor Milk Program!). The other change which the above post also spoke of was the potential to eliminate bovine milk altogether with the use of Prolacta (Human based human milk fortifier). While we don’t have the approval to use the product as traditionally indicated, we have used it as a “rescue” for those patients who demonstrate a clear intolerance of bovine fortifier. Such patients would traditionally receive inadequate nutrition with no other option available but now several have received such rescue and we look forward to analyzing the results of such a strategy shortly!
The first is that through a generous donation and the blessing of our health region we have been able to expand the use of donor breast milk from < 1250g for a two week period to < 1500g for a one month period. This wonderful change came about after much effort and was celebrated in December as we not only expanded the eligibility criteria but partnered with the NorthernStar Mother’s Milk Bank to provide donor milk to Manitobans (Manitobans Now Able To Support Premature Infants Through Donor Milk Program!). The other change which the above post also spoke of was the potential to eliminate bovine milk altogether with the use of Prolacta (Human based human milk fortifier). While we don’t have the approval to use the product as traditionally indicated, we have used it as a “rescue” for those patients who demonstrate a clear intolerance of bovine fortifier. Such patients would traditionally receive inadequate nutrition with no other option available but now several have received such rescue and we look forward to analyzing the results of such a strategy shortly!
Without question the most talked about change was the change in threshold for recommending resuscitation from 24 to 23 weeks.  The change took almost a year to roll out and could not have been done without a massive educational rollout that so many people (a special thank you to our nurse educators!) took part in. Looking back on the year we have now seen several infants at 23 weeks who survived with a small minority dying in the newborn period. It is too early to look at long term outcomes but I think many of us have been surprised with just how well many of these children have done. Moreover I believe we may be seeing a “creep effect” at work as the outcomes of infants under 29 weeks have also improved as we developed new guidelines to provide the best care possible to these vulnerable infants. Antenatal steroid use is up, IVH down and at least from January to September of last year no infants died at HSC under 29 weeks! I look forward to seeing our results in the future and cannot tell you how impressed I am with how our entire team came together to make this all happen!
The change took almost a year to roll out and could not have been done without a massive educational rollout that so many people (a special thank you to our nurse educators!) took part in. Looking back on the year we have now seen several infants at 23 weeks who survived with a small minority dying in the newborn period. It is too early to look at long term outcomes but I think many of us have been surprised with just how well many of these children have done. Moreover I believe we may be seeing a “creep effect” at work as the outcomes of infants under 29 weeks have also improved as we developed new guidelines to provide the best care possible to these vulnerable infants. Antenatal steroid use is up, IVH down and at least from January to September of last year no infants died at HSC under 29 weeks! I look forward to seeing our results in the future and cannot tell you how impressed I am with how our entire team came together to make this all happen!
What’s Next?
I wanted to share some of the initiatives that came forward or were chronicled on these pages over the last year to show you that this forum is not just a place for my mind to aimlessly wander. It is a place that can create change; some good, some great and no doubt some that won’t take. It has also been a place where ideas are laid out that have come from afar. From readers anywhere in the world who ask a question on one of the social media sites that get me thinking! I have enjoyed the past year and expect I will continue to enjoy what may spring forth from these pages for some time to come. Thank you for your contributions and I hope you get a little something out of this as well!

by All Things Neonatal | Feb 18, 2016 | resuscitation, Uncategorized
Ask almost anyone who has worked in the field of Neonatology for some time and they will tell you that babies are not as sick as they once were. We can give a lot of credit to better antenatal steroid use, maternal nutrition and general management during pregnancy. Additionally, after birth we now rush to place infants on CPAP and achieve adequate expansion of the lungs which in many cases staves off intubation.
The downside to our success though is that the opportunities to provide positive pressure ventilation (PPV) and moreover intubation are becoming less and less. How then do we perform when we are asked to do such procedures on an infrequent basis? The answer as you might expect is not that well. Dr. Schmolzer et al studied the ability of people to keep a good seal and found a 29% leak on average with as high as 63% in one patient. As this was a study in which people were being observed one might think the Hawthorne Effect might artificially decrease the percentage leak compared to real world scenarios when you know you aren’t being watched.
What is the cause of the leak?
Leaks most commonly occur on either side of the nasolabial folds. Although at least in my experience we educate trainees about this issue it remains a problem. I would also speculate that at the times when we need to be at our best during an advanced resuscitation involving chest compressions we may well function at our worst. This is the effect of the adrenalin rushing through our system as our sympathetic system turns into overdrive. The question therefore is one of getting around human error in particular when we need to minimize such inefficiency the most.
The Solution?
If the masks are prone to leaking and with it the ability to properly ventilate compromised, how could we minimize such human error. The answer may lie in what I consider to be an ingenious way to apply a mask. The concept and it is just that at the moment is to use suction to apply the mask to the face without risk of leak. 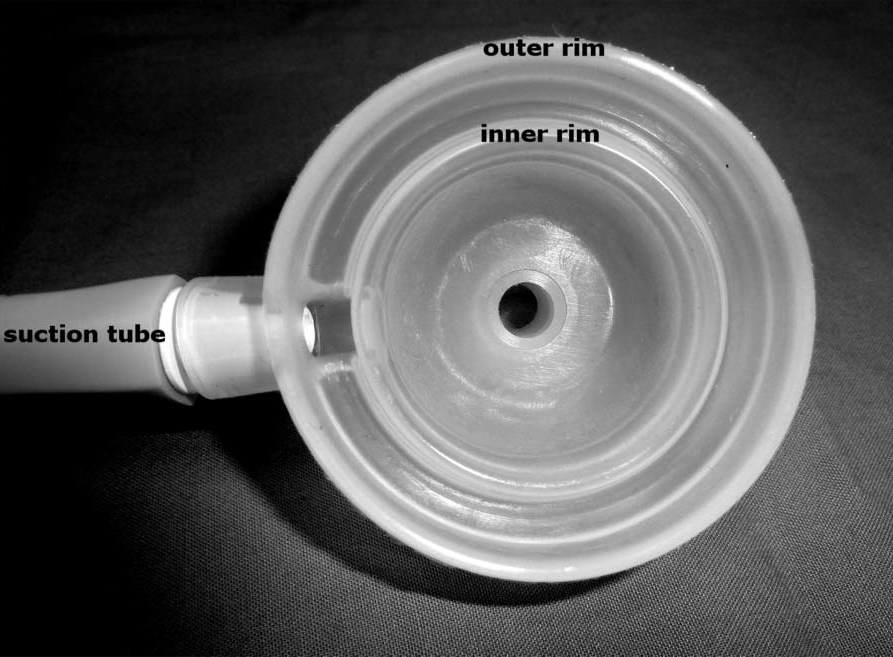 Lorenz L et al have just published a proof of concept study utilizing a mannequin with a “seal skin” layer applied to the face to simulate human skin. The article is entitled A new suction mask to reduce leak during neonatal resuscitation: a manikin study.
Lorenz L et al have just published a proof of concept study utilizing a mannequin with a “seal skin” layer applied to the face to simulate human skin. The article is entitled A new suction mask to reduce leak during neonatal resuscitation: a manikin study.
In this study, the mask was applied to the face of the mannequin and 100 cm H2O pressure was applied through a side port on the mask. There is an inner and outer ring such that the internal 41 mm diameter mask is surrounded by a double wall in which the suction is applied to the space between the two walls leading to the mask seating itself firmly against the face. The authors then studied the amount of leak found when using a Neopuff set to deliver 40 – 60 breaths per minute at pressures of 25/5. For this study 60 courses were tested.
How did it do compared to PPV through a traditional mask?
As you might expect (since you can feel my excitement!) it did very well. The average leaks using a conventional approach were quite good at 12.1% but the suction mask was only 0.7% leak. Importantly the ranges were quite different. PPV through a conventional mask had a range of 0.6 – 39% leak while with the suction version it was 0.2 – 4.6%. These results were statistically different.
What does the future hold?
As mentioned this study is what one would consider a proof of concept study. We do not know how this would fare in the real world and that of course is the next step. In terms of harm, the authors did note that when applied to the forearm of an adult it caused some mild redness from the suction that vanished quickly on breaking of the seal but we do not know if there could be greater harm in a newborn in particular one who is quite small. Such testing will be needed as part of any further study.
Having said that I think this rethink of the mask for PPV could be transformative to those who perform neonatal resuscitation infrequently. If this mask is found not only to be effective in a clinical trial but safe as well I would suggest a change to this type of mask could quite literally be life saving. Placed in the hands of those who are inexperienced in keeping a seal, PPV would become much more effective and in particular for rural sites the infants being transported in much more stable than some are at present.
Keep your eyes peeled for future work using this mask. Something tells me if it proves to be efficacious outside of a seal skin covered mannequin, your toolkit for providing NRP may be in for a change.
