I don’t think you can be a Neonatal blogger without writing about the patent ductus arteriosus from time to time. It’s been a little while so when something floats past my desk that I find interesting I share it with you. When that article is Canadian and written by someone I collaborate with on the Canadian Pediatric Society Fetus and Newborn Committee I am even more apt to do so. In the last few years the idea of letting nature take its course with respect to the PDA has been growing. The evidence is lacking that treatment for most infants in the first two weeks of life makes a difference to important pulmonary outcomes ie. BPD. There is a growing movement asking whether treatment at all really makes a difference to these infants or whether we should just be managing the medical complications of increased pulmonary bloodflow with diastolic steal from the kidneys and intestine. The alternative of course is to treat these infants most commonly with NSAIDs and hope that side effects such as renal impairment and spontaneous intestinal perforation don’t happen. Full disclosure, I was raised to find the PDA and if hemodynamically significant treat it, so that has been my general approach. I am open to suggestion though so without further adieu let’s talk about a recent Quebec study on the topic.
University of McGill in Montreal
Anchored by Dr. Altit with the lead author being De Carvalho Nunes the experience at this hospital was recently published as Natural evolution of the patent ductus arteriosus in the extremely premature newborn and respiratory outcomes. The authors looked a specific population of infants born at <29 weeks gestational age (214 infants in total) and importantly had a reasonable number of small infants >26 weeks at birth (84) to see what happened to their PDAs in the long run. Many years ago the unit adopted a non-intervention policy with respect to treatment of PDAs and since 2015 were in a new hospital. This afforded them the opportunity to look retrospectively at a modern cohort of infants all cared for in the same environment from Feb 2015 – Sept 2019 and see what happened to respiratory morbidity over time. While this was retrospective and lacks a control group the concept here was that one could look at the rate of BPD over time and see if it was static, rising or falling and in turn you could also compare to the Canadian Neonatal Network (not done in this study) to see if your approach was leading to all sorts of morbidity.
What did they find?
The authors chose to standardize the definition of BPD:
Grade I (nasal flow cannula <1 L/min with FiO2 ≤ 70%; nasal cannula with flow of 1 to 3 L/min and FiO2 between 22 and 29%; CPAP, noninvasive positive pressure ventilation [NIPPV] or nasal cannula with flow >3 L/min with FiO2 of 21%),
Grade II (nasal flow cannula <1 L/min with FiO2 > 70%; nasal cannula with flow of 1 to 3 L/min and FiO2 ≥ 30%; CPAP, NIPPV or nasal cannula with flow >3 L/min with FiO2 between 22 and 29%; invasive mechanical ventilation [IMV] with FiO2 of 21%)
Grade III (NIMV, NIPPV or nasal cannula with flow >3 L/min with FiO2 ≥ 30%, IMV with FiO2 > 21%).
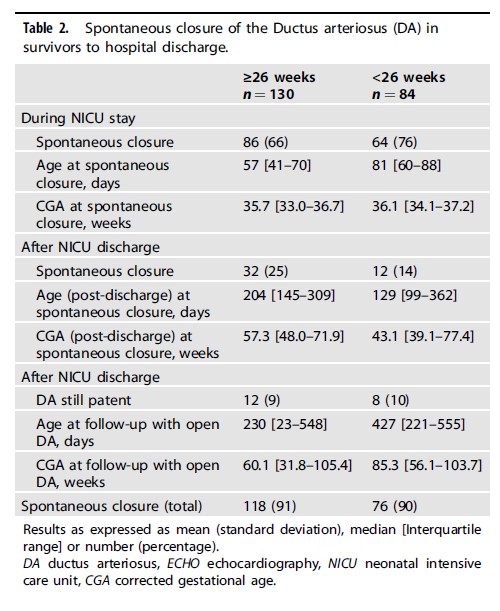
When looking at the total population including after discharge 91% of all babies greater than or equal to 26 weeks experienced ductal closure without intervention. Secondly, if you look under 26 weeks the results were hardly any different with 90% closing. Before discharge from the hospital 66% of the larger infants experienced closure prior to discharge and 76% of those under 26 weeks. Interesting finding that more infants under 26 weeks by percentage had closure.
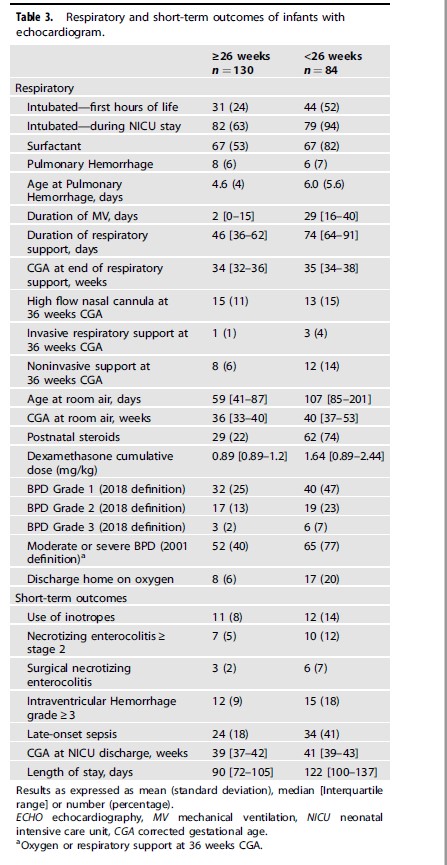
Looking at the respiratory outcomes a total of 77% had BPD under 26 weeks of varying severity compared to 40% in the larger infants. Other morbidities were not different.
Interestingly the authors also noted a decline in Grade 2 BPD over the 5 year study.
Thoughts on the results
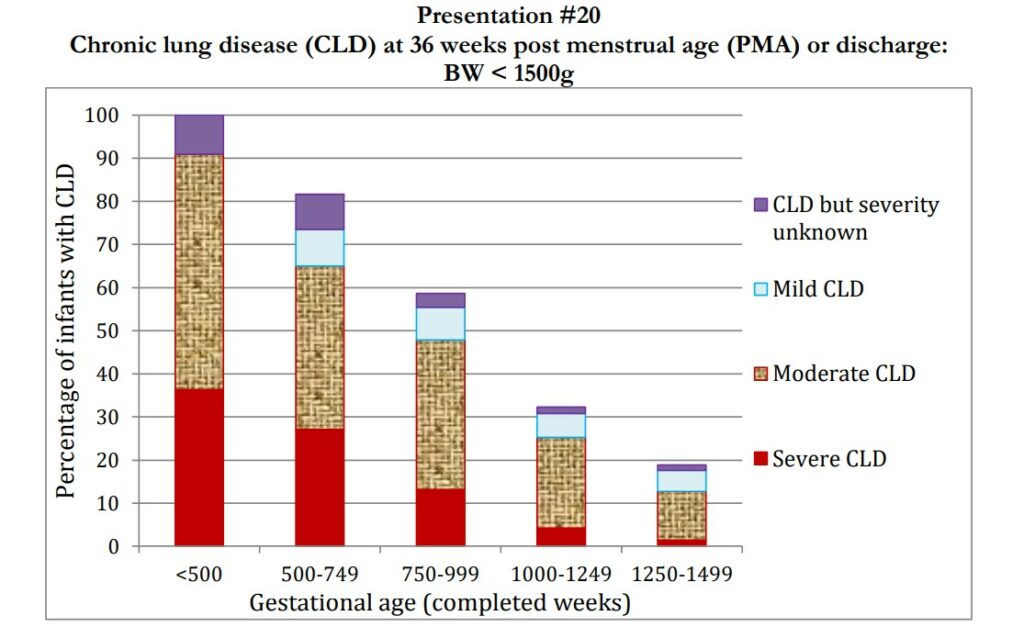
It’s important to look at the overall results from the Canadian Neonatal Network to see how this group compares to the rest of the country. What follows is not perfect but its a start for a discussion.
This includes all babies in the CNN under 1500g. If we use <1250g as a rough cutoff for under 29 weeks you can see that by weight the rate of chronic lung disease ranges from 30 – 100%. At 77% under 26 weeks which corresponds to babies around 750g or less (some are a little more) then the rate should be somewhere between 60 – 80% if you count babies 500 – 750g. I would say the rate of 77% overall is not bad in terms of comparison. Secondly if you look at the distribution of CLD for this group it was at their centre it was 47, 24 and 7% for Grade 1 – 3 respectively. This is particularly interesting as when you look at mild, moderate and severe in the bars above it would suggest their babies on average with a “benign neglect” approach are more mild. This approach is looking up!
One thing that I note though is that the rate of postnatal steroid use in this group was 75% under 26 weeks and 22% for those from 26-28 weeks. This represents a large increase over the mean in the CNN back in 2019 of 11.9% for postnatal steroid use. The babies under 26 weeks were also ventilated invasively for a median of 29 days. That seems a little long to me but there are no comparisons with the CNN to know for sure.
I can’t help but wonder if you are trading short term pain for long term gain. It’s hard to argue with the long term results in terms of a shift towards better rates of lower grade BPD. I do wonder though if the eventual closure of the PDA is being helped along with use of more postnatal dexamethasone. There is some data suggesting increased rates of closure with use of dexamethasone so maybe what is going on here is that rather than using NSAIDs there is a shift to long durations of ventilation and increased rates of dexamethasone use. Something for the authors to look at though.
With everything there are trade offs so maybe less NSAID use means longer ventilation and more postnatal steroids but in the end the pulmonary outcome is better? I see a prospective RCT coming to eventually settle this debate!
Jaundice has to be one of the most common issues facing newborns and their families. Whether in the NICU or on the post-partum floor all babies get jaundiced to a certain degree and some become so much so that they require treatment. Many centers the world over have developed home phototherapy programs to allow treatment to be done at home and they are known to be effective. In Sweden such programs exist and in theory sending infants home rather than keeping them in hospital could have positive effects for both the infant and parent dyad in terms of bonding. Keeping the infants in hospital and in particular over the last couple years when in many places of the world COVID protocols made visiting more difficult there is the real potential to disrupt bonding if a baby is otherwise ready for discharge. Researchers in Sweden with such programs in Uppsala recently decided to explore this question about bonding so here we go.
The Study
This was a multicentre study in Sweden by Pettersson M et al entitled Home phototherapy of term neonates improves parental bonding and stress: findings from a randomised controlled trial. The study intended to enroll 250 infant-parent pairs into an RCT comparing in-hospital phototherapy to home phototherapy and determine the status of bonding between child and parents at various time points. The inclusion criteria required infants to be >36 weeks at birth, have non-immune jaundice (DAT -ve) and have a bilirubin at inclusion from 300-400 micromol/L from 48 – 60 hours of age. Infants with asphyxia and weight loss >10% were excluded. Infants were also excluded if their parents did not speak Swedish or if the physician felt they would not be able handle home phototherapy.
In both environments treatment was provided with a biliblanket or overhead blue lights 25 cm from the skin which the infant would lay on or be placed under. These infants did not have severe bilirubin levels so it appears they had only standard phototherapy. This makes sense as babies with higher risk would not be suitable for consideration of home phototherapy.
Several validated tools were used to determine such things as bonding, risk of depression and stress. The primary outcome was based on use of the Postpartum Bonding Questionnaire (PBQ). Higher scores indicate worse bonding. The sample size was calculated on results from previous studies showing a mean (SD) of 10.7 (8.5) in 250 newborns with 90% power to detect a three-point difference in mean PBQ-sum for mothers at the 5% significance level, with a pre-planned interim analysis after 125 inclusions.
Enrollment was slow and after the preplanned analysis it was decided to stop the study recruitment and see where the results landed.
The Findings
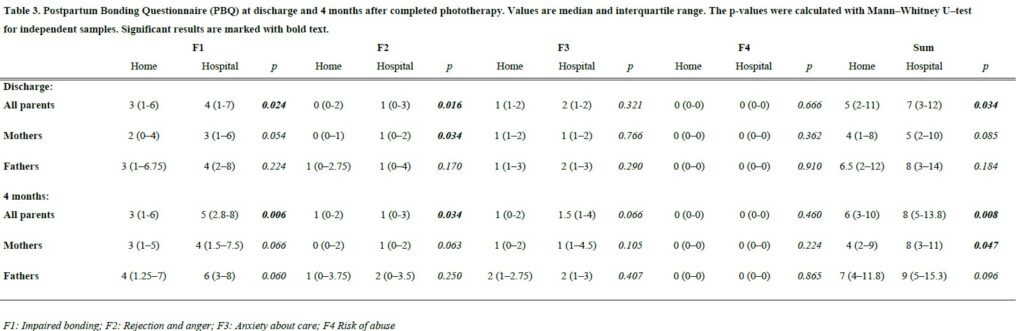
Both groups of infants were treated for a total of about 4 days with testing for bilirubin levels and treatment with phototherapy (about 18 hours of total treatment both groups). The results of the PBQ found a statistical difference in measures of bonding favouring the home phototherapy group as found in the table below at both discharge and 4 months.
Interestingly when breaking down the results by mothers and fathers there was no impact on bonding for the fathers after this four day period of investigation and treatment at hospital vs in the home but at both time points it was the mother that drove the benefit seen. This likely speaks to differences in the way mothers and fathers experience bonding or perhaps how they process threats to it. No differences in stress could be found between the two groups but it is important to note that the small sample size and the fact that it was a secondary outcome make it difficult to say with certainty that there is no impact on stress.
Thoughts
You would be well within your rights to say “so what? It’s what we expected”. The difference seen in bonding while favouring the at home group has statistical significance but I am not sure to what degree this represents clinical significance. Can you truly perceive a difference in bonding based on a two point difference? Would that be meaningful functionally in the home in the way that parents relate to and respond to their infant? Not sure.
What I think we can say though is that the direction of the effect is certainly positive. We can also say from a systems standpoint that not only is phototherapy using a biliblanket safe and effective but it also moves care to the home and thereby creates room in the hospital for babies who truly need to be admitted.
Given the direction of the effect I think what the study does is provide one more argument aside from improving patient flow to aid in the establishment of home phototherapy programs. There are benefits not only to the family from an earlier discharge but also to some degree improvements in bonding certainly between mother and baby. This brief four day period has impacts that can last all the way out to four months. If you were looking for some evidence to support building such a program, maybe this will help!
Every parent the world over waits for that moment after birth when they first hear the cry of their child. The cry is a sign of health, of vigour and a relief that all should be ok. I had never questioned when the infant cry develops but one thing is for sure, it doesn’t matter whether you are born at 25 , 30 or 37 weeks, the babies all seem to make it after delivery. Much like suck, rooting and swallowing which we know begin in utero as we can see fetal swallowing movements the question is does cry begin in utero.
Evidence for an In-Utero Start
Before I get into the answer to this let me address the title question. A cry is produced as a baby exhales and moves air in a turbulent fashion across the vocal cords. Since a fetus is not breathing air it would seem impossible for a cry to be produced by a fetus. It doesn’t mean though that a fetus can’t try to at least practice and get ready for birth.
Back in 2005, a research team from New Zealand sought to answer this question in their paper Fetal homologue of infant crying. The authors described a case of a 33 week infant who was exposed to an artificial larynx generating a sound on the maternal abdomen while she was undergoing an ultrasound. The artificial larynx produced a vibroacoustic stimulation (VAS) after first keeping monitoring the fetus with ultrasound for a period of 20 minutes. The duration of the VAS was for 40 seconds and during this time the fetus was found to turn its head upon hearing the VAS and appeared to startle.
As per the authors the fetus underwent the following steps after the stimulation.
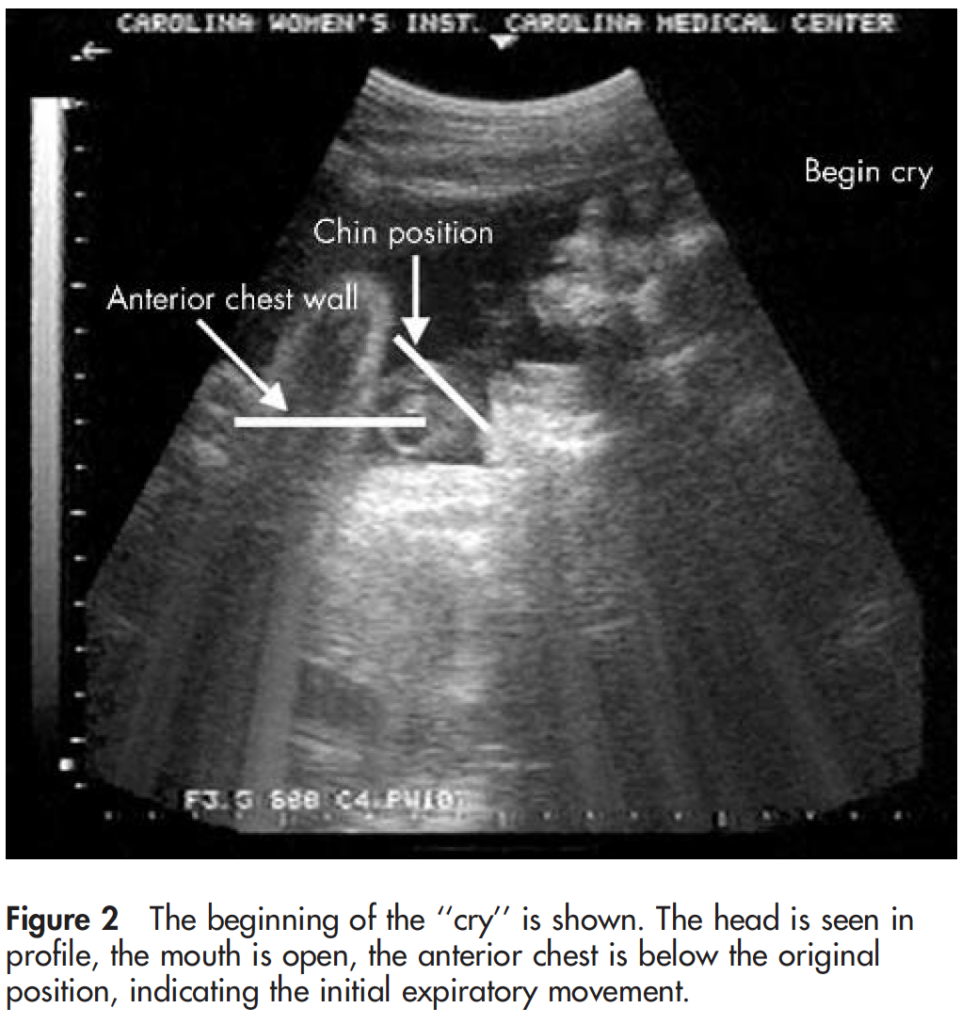
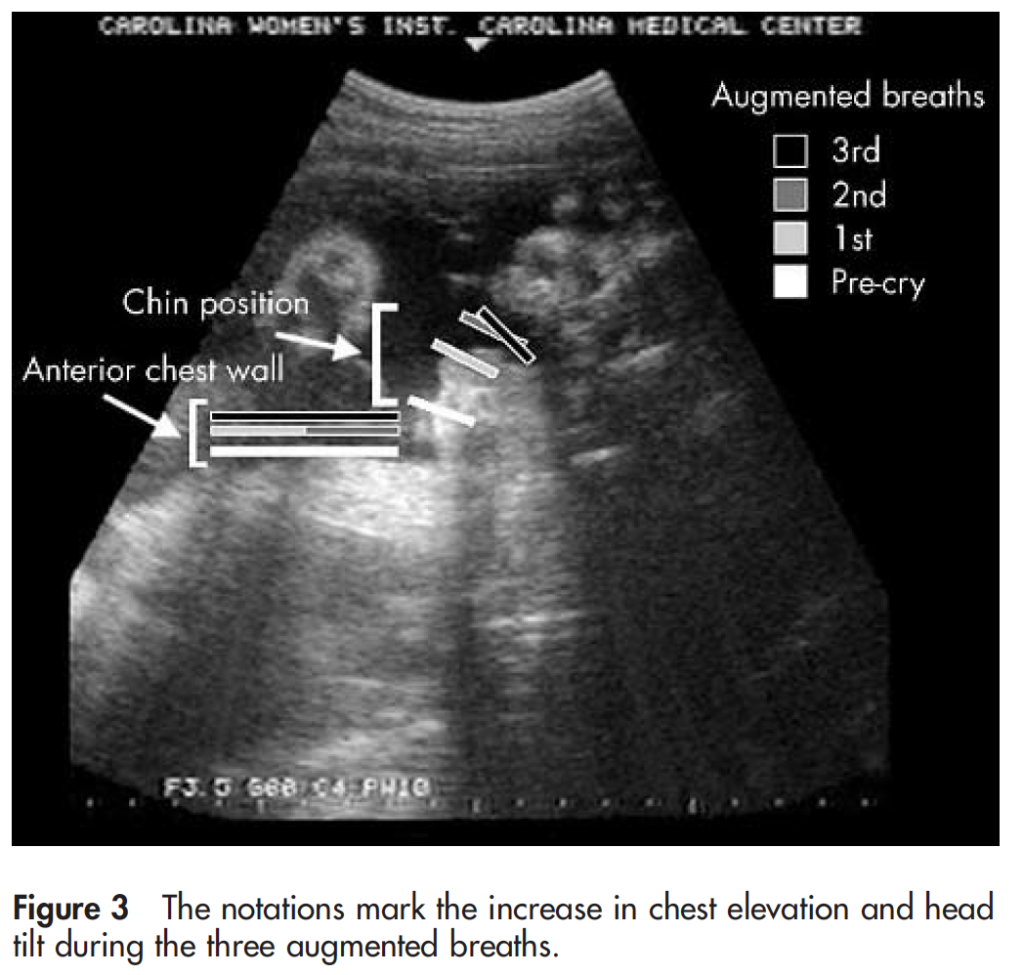
“There is a brief expiration that is followed by a deep inspiratory phase with a subsequent pronounced expiratory phase. This expiration is associated with jaw opening, taut tongue, and chest depression (fig 2). It is immediately followed by three augmented breaths with progressive increase in chest rise and head tilt (fig 3).”
At the end of this episode the chin was found to be quivering. This as I see it is the best and first description of fetal crying. While it doesn’t make a sound I believe at least that this is the beginning of an important step in development that will prepare the infant after birth to clear its lungs and inflate them with air.
The question now I ask is when does this develop? As I mentioned earlier the ability to cry is definitely present in preterm infants at pretty much any gestational age I have seen all the way down to 22 weeks. Much like other reflexes present at birth and the swallowing function mentioned earlier this must develop for a reason and I am hopeful that future work will uncover when this first appears and eventually add an explanation of what function this in-utero crying movements serve!
For commentary on this including a video of the first and second cry for this infant have a look at the full video below
I couldn’t think of a better topic for World Prematurity Day 2021 than what constitutes the edge of viability. Thinking back over my career, when I was a resident and fellow infants born at 25 and 26 weeks were deemed about as low as “we should” go but we certainly resuscitated infants at 24 weeks but this was considered heroic. Jump ahead to the last decade and we began caring for infants at birth at 23 weeks so commonly that the thought of offering comfort care only to infants at 24 weeks became almost unthinkable for many health care providers. Before I get jumped on, let me say that I am not saying I agree or disagree with that sentiment but it is something that is felt by many.
The Shared Decision Model
In the last few years a rethink again has occurred whereby the concept of the treating team knowing best has been replaced by the “shared decision model”. In this line of thinking, it is not up to us as health care providers to “tell the parents” what to do but rather come to a shared decision based on an assessment of the wishes and values of the parents in conjunction with hearing about both short and long term problems their infants may face if resuscitated. This concept was central to the statement by the Canadian Pediatric Society that I am proud to have been part of with respect to its development. The statement for those that are interested is Counselling and management for anticipated extremely preterm birth
What’s next? Going below 22 weeks?
The challenge of the shared decision model is that there comes a point where the answer is simply “no”. If for example a family at 19 weeks gestation demanded an attempt at resuscitation I would have to inform them that survival is not possible (assuming ultrasound confirmed anthropometric measurements consistent with that age). The question though becomes a little more difficult to answer at 21 weeks and was the subject of a recent article in the New York Times about a survivor at 21 weeks gestation.
Even with the best gestational age dating the estimate can be off by up to 5 days so it’s possible that the infant in this story was closer to 22 weeks or even midpoint between 22 and 23 weeks in reality. Regardless it does raise the question about what to do at 21 weeks and I suspect we will begin to see more stories about this now that the glass ceiling of 22 weeks has been breached. What about below 21 weeks? Sounds impossible I know but with research that remains at the stage of animal studies this may become possible. Maybe not in the next 5-10 years but it could happen in my lifetime in this chosen field.
The Artificial Placenta
This made headlines a few years ago with the news that the Children’s Hospital of Philadelphia had successfully kept a lamb alive for a period of 4 weeks using an artificial placenta and amniotic fluid.
You might think that this was a one-off experiment that will never see the light of day but similar work is being done in Toronto, Canada where they have been able to do similar work with preterm piglets in their paper Achieving sustained extrauterine life: Challenges of an artificial placenta in fetal pigs as a model of the preterm human fetus. Incidentally as my colleague Dr. Ayman Sheta worked on this project while in Toronto I am particularly pleased to share this research. Similar to the experience in CHOP the team in Toronto has been able to keep piglets alive for progressively longer durations. My understanding is that despite the best efforts infectious complications over arise limiting how long one can sustain such animals.
This leads me to my final thoughts on where we might be able to go. I see a future where we apply such technology to humans but not in the way that people might have thought. Keeping a fetus after delivery at 21 or 20 weeks on an artificial placenta for many weeks is not likely a realistic goal. What if we could get 1 or 2 weeks though and allow the fetus to be oxygenated without using positive pressure on their developing lungs and transition them at 23 or 24 weeks gestation? We may in this way be able to allow for postnatal maturation in a artificial uterine environment and give babies a chance who would otherwise never had the opportunity for a shared decision with medical staff.
Sound like science fiction? Well the beauty of the internet as my friend told me today is that once it’s out there it out there for good. Let’s see how this post stands the test of time and to all the babies out there in NICUs and to their families I wish you all a good and uneventful World Prematurity Day wherever you may be!
If you work in Neonatology then you can’t help but see babies with jaundice. It is so common in the NICU that I would call it normal. While mild jaundice is part of neonatal life, sometimes levels increase to the point that it can be dangerous to the developing brain and in the short term cause acute bilirubin encephalopathy. Chronic injury can lead to hearing impairment and kernicterus with staining of the basal ganglia and cerebral palsy. Phototherapy has been the mainstay of treatment with exchange transfusion reserved for exceptionally high levels of bilirubin. In recent years people have utilized IVIG when hemolysis is present to reduce the risk of exchange transfusion. There hasn’t been much else that one could use but many years ago, proto-porphyrins (SnPP)were looked at as a class of drug that might help reduce the burden of bilirubin by blocking where the substance comes from. Bilirubin is liberated when heme is broken down by heme-oxygenase so an inhibitor of this enzyme (of which the metallo-porphyrins (Sn-MP)might be the right candidate for the job. While initial trials seemed to show benefit there was a side effect of studies in rats indicated that exposure to Sn-PP (but not Sn-MP) led to photosensitivity if exposed to UV light and phototherapy. Given that the Sn-MP class of drugs didn’t seem to have the same issues an interest in this class of drugs has experienced a resurgence.
Phase IIb clinical trial
In the development of drugs there are different phases of trials. In a phase IIb trial, researchers believing from previous research that there is a treatment effect, perform a larger study using different dosing to see if there is still a benefit. In the case of Sn-MP this was done by Rosenfeld WN et al in their recent trial Stannsoporfin with phototherapy to treat hyperbilirubinemia in newborn hemolytic disease. The trial design included infants with hemolytic disease with 91 patients divided into three groups; 31 controls, 30 receiving a 3 mg/kg IM dose and 30 receiving a 4.5 mg/kg IM dose of stannsoporfin along with phototherapy. The goal of the study was to see whether infants receiving such treatments would experience different trajectories in their levels of bilirubin. In order to standardize things as much as possible, all infants were enrolled once they reached a pre-specified level using the AAP phototherapy curves and underwent serial TsB measurements at 2,6,12,24,36 and 48 hours after study entry.
Phototherapy was standardized based on measurement of spectral irradiance at the skin surface with maintenance of 30 microW/cm2/nm to ensure that each infant received the same level of phototherapy.
The Findings
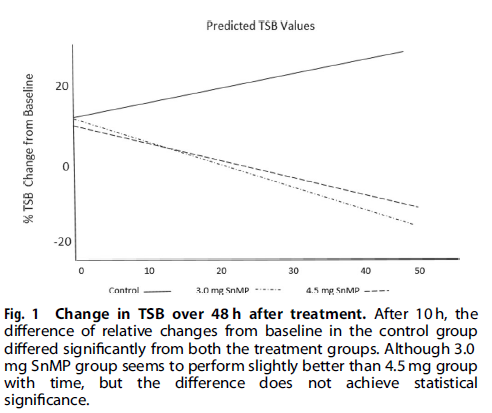
I suppose it shouldn’t shock anyone that the drug works as the class of drug was found to work almost 40 years ago! Looking at the three groups over the 48 hour time frame shows a markedly different trajectory for the patients.
Using an intention to treat analysis the authors noted a 17.5% increase in bilirubin from baseline over 48 hours in the control group and a -13.0 % change in the 3 mg/kg and -10.5% in the 4.5 mg/kg arm. The differences between the two treatment groups compared to the control arm was significant but between the two dosing levels not.
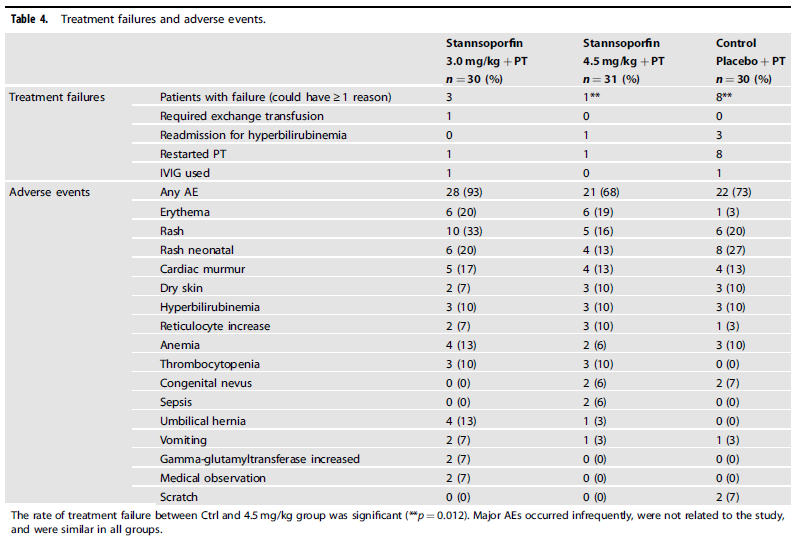
From a side effect standpoint, the following was noted:
Looking at the data, rashes and flushing may be relatively more common yet are transient. Curiously, the number of treatment failures in the control arm was significantly higher meaning of the 30 patients treated with phototherapy alone, 8 had to restart after the predetermined threshold for stopping phototherapy was reached.
Is this ready for prime time?
The purpose of sharing this information with you is not to promote it as a treatment that we should all jump on. I think this story is still early. What will be needed from here are larger studies with well designed follow-up targeting long term outcomes. This study will be following up patients to see how they did but larger numbers will no doubt be wanted before people embrace this wholeheartedly. A quick search of trials on clinicaltrials.gov shows that there are several trials completed and no doubt some to come. Having an exchange transfusion is no laughing matter as there are risks related to clotting, bleeding, platelets etc so having another tool in our toolkit to deal with this common issue in neonates is of interest to me. Maybe it is of interest to you as well.