If you have been following this blog for awhile you may recall a post from a couple years back on Physiological based cord clamping. The premise of that paper was that rather than arbitrarily choosing a time to clamp the cord, one should look for the following three features that indicate adequate pulmonary blood flow has been established:
1. Establishment of adequate breathing(average tidal volume > 4 ml/kg) on CPAP – using a mask capable of measuring expired volumes
2. HR above 100 BPM
3. SpO2 above the 25th percentile using an FiO2 <0.4
In the original trial it was a proof of concept design that sought to determine if resuscitation on their “Concord” table was feasible and how long would it take for the above criteria to be met so the cord could be clamped.
The mean time for cord clamping in that trial was 4 minutes and 23 seconds. This is much longer than the typical delayed clamping of 30 -60 seconds and even longer than the few studies that have looked at delays of 1- 3 minutes.
The Next Phase
The same group now sought to compare DCC of 30 – 60 seconds with the PBCC approach for infants <32 weeks gestational age in the paper Physiological-based cord clamping in very preterm infants – Randomised controlled trial on effectiveness of stabilisation. This trial was set up as a non-inferiority trial to see if the pre-defined difference in time to stability of 75 seconds would be crossed. A power calculation was performed that indicated the authors would need to recruit 64 infants with 32 in each arm. Due to poor recruitment the authors chose to stop the trial early with only 17 infants in the DCC group and 22 infants in the PBCC arm. An analysis with those patients identified that the non-inferiority limit had been met already.
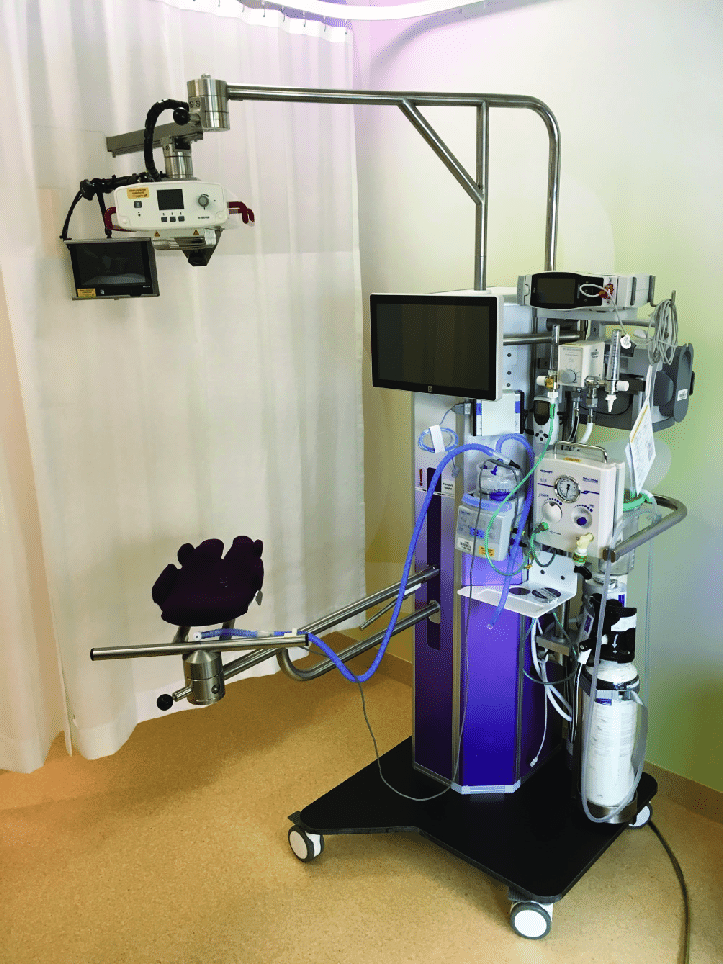
Difference in resuscitation
Infants randomised to the DCC group had their cords clamped at 30-60 seconds and had their resuscitation started on a resuscitation table. Infants in the PBCC arm were placed on the Concord after delivery and had their resuscitation performed there. Care afterwards would have been similar.
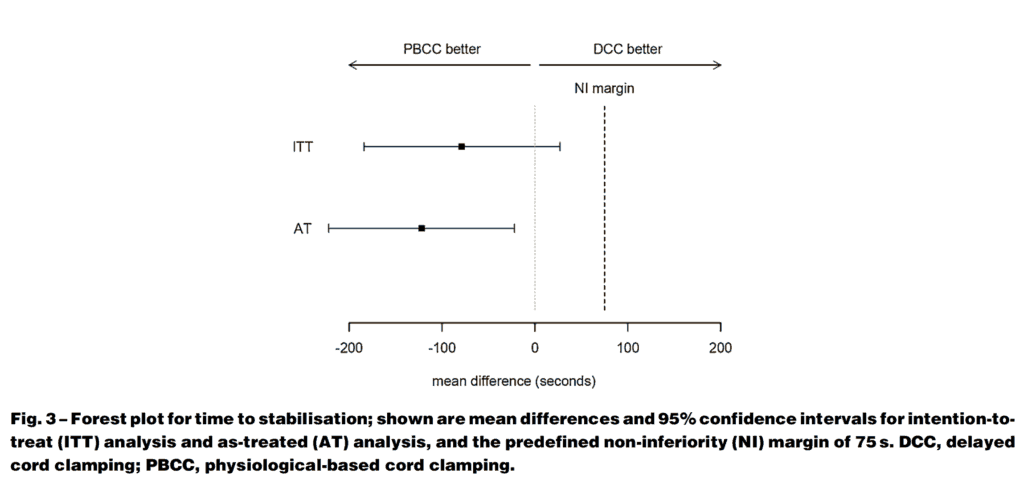
They found that the mean time to stabilisation was 5:54 +/- 2:27 in the PBCC group and 7:07 +/-2:54 in the DCC groups. The mean difference was 1:19 min (95% CI -3:04 to 0:27 min). The results clearly demonstrated a finding of shorter time to stabilisation in the PBCC arm as shown in the figure.
As the confidence interval crossed 0 though in the intention to treat analysis we can say that PBCC is no worse than DCC but can’t say it is superior as a strategy overall. Perhaps larger numbers may have shown something different but at least we know it isn’t worse.
Other Findings
One thing that I would imagine Obstetricians would be concerned with here is the potential for significant blood loss since uterotonics were not provided until the cord was clamped which in PBCC was quite a bit longer, Opposite to what one would have expected the mean blood loss in the DCC group was 450 mL compared to 300 mL in the PBCC arm. Not different statistically though given the small numbers.
There were almost twice the number of females in the PBCC group which could account for some of the findings here. Another difference worth noting was that respiratory support was initiated earlier on the concord than on the standard resuscitation table which the authors acknowledge may be due to familiarity with doing so from experience with the specialized set up. Earlier ventilation (1:11 min vs 2 min in the DCC) could indeed lead to earlier reaching of the end points of the stabilisation criteria.
Regardless of the last couple points, what is needed now is a much larger study to look at clinical outcomes. The numbers were so small here to really examine such clinical points but this is where I believe we are now headed. If the pattern continues I guess we will see another study coming from this group in a couple years so stay tuned!
Delayed cord clamping has been written about before on this blog. In fact between the blog and facebook posts I think it has been discussed many times. What hasn’t really been touched upon whether one type of cord management is superior to another. Is delayed cord clamping equivalent to cord milking or is one better than the other? The answer is a complicated one as you first need to define what both are. For delayed cord clamping it could be as short as 3 minutes and as long as 5 minutes or so as was seen in the post on physiological based cord clamping. For cord milking I suppose the definition is a little less broad but typically involves stripping of the cord after allowing the cord to fill with placental blood to enhance flow over a shorter time than DCC from the placenta to the newborn.
A Head to Head Comparison
Katheria A et al published Association of Umbilical Cord Milking vs Delayed Umbilical Cord Clamping With Death or Severe Intraventricular Hemorrhage Among Preterm Infants this past month in JAMA. The authors compared two well defined approaches to care after delivery. Delayed cord clamping was defined as being at least 60 seconds (mean time was about that) while cord milking was done by using 20 cm of the umbilical cord and milking for 2 seconds allowing refill, and then repeating 3 more times. The primary outcome under study was the incidence of death or severe IVH at 6 month’s corrected gestational age. The goal was to enroll 502 per group based on their power calculation. Furthermore the study design included randomization into two strata of 23 weeks 0 days to 27 weeks and 6 days and 28 weeks o days to 31 weeks 6 days. They managed to enroll 474 infants and in each arm there was good compliance with the allocated intervention (98% for cord milking and 93% for delayed cord clamping. What makes the study interesting though is that it was stopped by the data safety monitoring board after 236 were enrolled in the cord milking group and 238 in the delayed arm.
What happened?
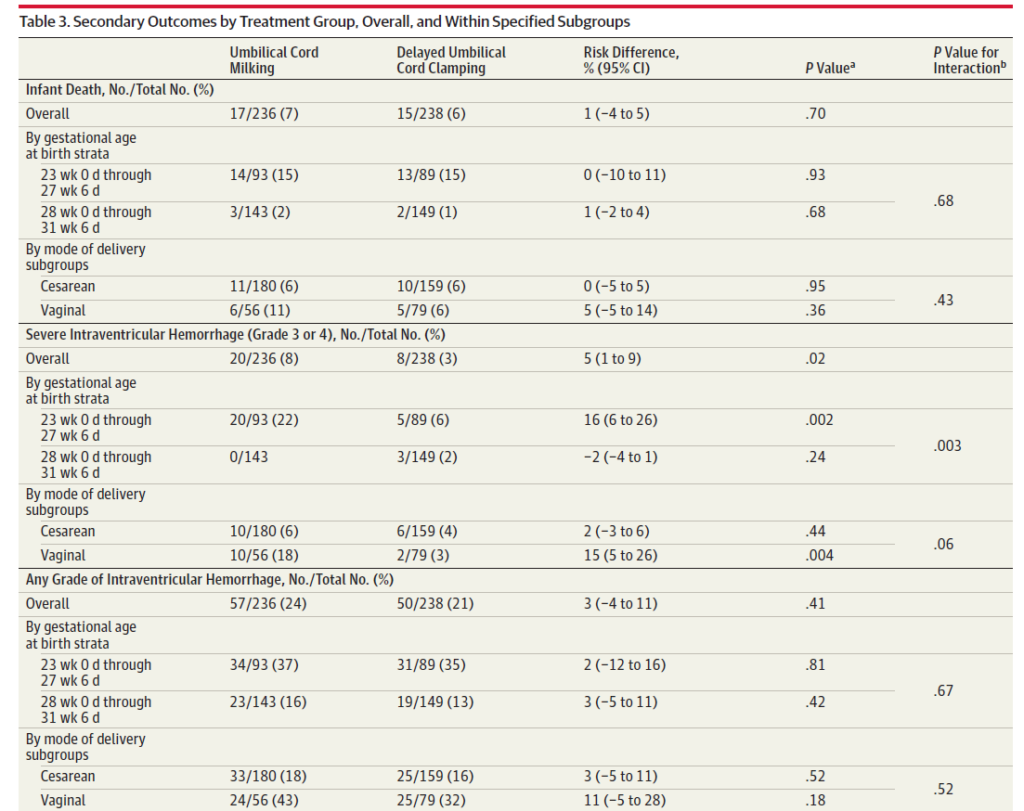
There were no significant differences between the maternal and neonatal demographics between groups. The mean time to clamping in the delayed group was 57.5 seconds compared to 22.8 seconds in the cord milking arm. The primary outcome at this point showed no difference between groups. What was concerning though was the pre-planned secondary outcome of severe intraventricular bleeding alone and is shown below.
The incidence of death from the above table was no different but in the group of infants between 23+0 and 27 +6 weeks there was a finding of 22% with severe IVH compared to only 6% in the delayed cord clamping group. This finding was understandably enough to shut down the study from enrolling further patients.
Why could this have happened?
I suppose we don’t know for sure but one of the benefits of writing a blog is that I get to speculate! The cerebral vasculature of small infants is quite fragile and furthermore is very poor at autoregulating its circulation. With cord milking I imagine it is similar to small boluses of blood. In a small preterm infant it may be that the baby is unable to limit the flow of blood adequately into the cerebral circulation leading to acute bleeding. Contrast this with the slow trickle of blood that one gets over a minute while the cord is not clamped.
This study is going to be a tough one to get past I suspect for those centres grappling with whether cord milking or delayed cord clamping in the best strategy. The question I think really these days should not be between these two but rather as I have written about before, how long should a delay in clamping really be? One minute is likely far too short while 5 minutes probably too long for most to be comfortable. I suspect the 2-3 minute range is where things will settle out. Additionally, strategies to allow resuscitation with an intact cord can and should be explored as those who are most sick at birth are likely the ones who could most benefit from a delay in clamping. More research is needed and I suspect you will hear about some before long on this site!
Much has been written on the topic of cord clamping. There is delayed cord clamping of course but institutions differ on the recommended duration. Thirty seconds, one minute or two or even sometimes three have been advocated for but in the end do we really know what is right? Then there is also the possibility of cord milking which has gained variable traction over the years. A recent review was published here.
Take the Guessing Out of the Picture?
Up until the time of birth there is very little pulmonary blood flow. Typically, about 10% of the cardiac output passes through the lungs and the remained either moves up the ascending aorta or bypasses the lungs via the ductus arteriosus. After birth as the lung expands, pulmonary vascular resistance rapidly decreases allowing cardiac output to take on the familiar pattern which we all live with. Blood returning from the systemic venous circulation no longer bypasses the lung but instead flows through pulmonary capillaries picking up oxygen along the way. One can imagine then that if a baby is born and the cord is clamped right away, blood returning from the systemic circulation continues to bypass the lung which could lead to hypoxemia and reflexive bradycardia. This has been described previously by Blank et al in their paper Haemodynamic effects of umbilical cord milking in premature sheep during the neonatal transition.
The cord was clamped after each of the following was achieved for an infant indicating successful transition with opening of the lung and establishment of an FRC.
1. Establishment of adequate breathing (average tidal volume ≥4 mL/kg) on CPAP. They used a mask capable of measuring expired tidal volumes.
2. HR above 100 bpm
3. SpO2 above 25th percentile using FiO2 <0.4
In this way, the cord was only clamped once the baby appeared to have physiologically made the transition from dependence on umbilical cord blood flow to ventilation perfusion matching in the lung. Although 82 mothers consented only 37 preterm infants were included in the end. Exclusion criteria were signs of placental abruption or placenta praevia, signs of severe fetal distress determined by the clinician and the necessity for an emergency caesarean section ordered to be executed within 15 min. This really was a proof of concept study but the results are definitely worth looking at.
How Did These Babies Do?
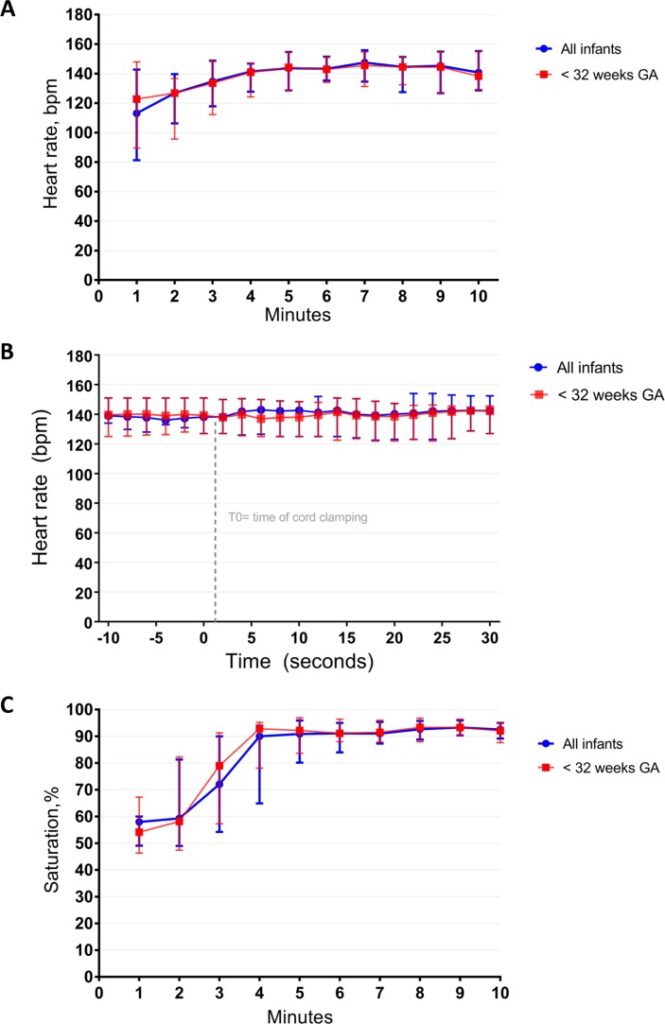
There are many interesting findings from this study. The mean time of cord clamping was 4 minutes and 23 seconds (IQR 3:00 – 5:11). Heart rate was 113 (81–143) and 144 (129–155) bpm at 1 min and 5 min
after birth. Only one patient developed bradycardia to <60 BPM but this was during a mask readjustement. The main issue noted as far as adverse events was hypothermia with a mean temperature of 36.0 degrees at NICU admission. Almost 50% of infants had a temperature below 36 degrees. Although the authors clearly indicate that they took measures to prevent heat loss it would appear that this could be improved upon!
What stands out most to me is the lengthy duration of cord clamping. This study which used a physiologic basis to determine when to clamp a cord has demonstrated that even at 1 minute of waiting that is likely only 1/4 of the time needed to wait for lung expansion to occur to any significant degree. I can’t help but wonder how many of the patients we see between 26-35 weeks who have a low heart rate after delivery might have a higher heart rate if they were given far more time than we currently provide for cord clamping.
I can also see why cord milking may be less effective. Yes, you will increase circulating blood volume which may help with hemodynamic stability but perhaps the key here is lung expansion. You can transfuse all the blood you want but if it has nowhere to go just how effective is it?
As we do more work in this area I have to believe that as a Neonatal community we need to prepare ourselves for the coming of the longer delay for cord clamping. Do we need to really have the “Concord” in every delivery or perhaps it is time to truly look at durations of 3-4 minutes before the team clamps the cord.





 The intervention here was applied to infants 26 to 35 weeks gestational age.
The intervention here was applied to infants 26 to 35 weeks gestational age.