I have to admit I know very little about this field despite having friends are practitioners. Anecdotally there are reports of premature infants who are not progressing as fast as parents want and requests are made for an an alternative healers. Such families may be delighted with the care they were receiving and as they see no adverse effects following treatments they wish the practice to continue.
As I reflected on these reports I turned to the literature to look at the third most common health practitioner in North America after doctors and dentists; the Chiropractor. The truth is I have known for some time that Chiropractors provide treatments for newborns and children but have been somewhat oblivious as to what services they can offer. My curiosity was piqued by finding that Chiropractors have been treating newborns for difficulties with breast-feeding. Before I turn to the evidence for such practice it is worthwhile reviewing what Chiropractic is based on.
Chiropractic is actually a relatively new field having been developed by D.D. Palmer in 1895, who was a magnetic healer. He believed that many diseases were caused by joint subluxations of the vertebrae, which would lead to interruptions of neurological impulses thus creating disease. Having said that the indications for Chiropractic have expanded over time as the profession has developed. While initially practiced in adults the use of such manipulations has expanded over time to include children some as young as newborns. One such goal is to improve success with breastfeeding and a sample manipulation is shown in this video:
When it comes to breast-feeding the number of studies examining efficacy are few and far between but the largest study is worth studying as at the very least it outlines what it is that the Chiropractors believe they are treating. In 2009 JE Miller et al published the following article: Contribution of Chiropractic Therapy To Resolving Suboptimal Breastfeeding: A Case Series of 114 Infants. In this case series, maternal infant dyads who were on average 3 weeks of age at presentation (but the most common age of presentation was 1 week) were referred to a Chiropractor for help in establishing exclusive breastfeeding. The infants in this study most commonly presented with issues latching on rather than drawing milk once latched. In fact the issue more often than not was simply not having the infant show interest in latching. The findings of the Chiropractors assessing these infants as to the etiology of the problem were as follows:
Altered tongue action resulting in ineffective latch
Aberrent cervical range of motion and/or posterior joint restrictions affecting infant posture and position
Hypo or hypertonic orbicularis oris, masseter, digastric muscles causing imbalance in muscle torque
Temporormandibular joint laxity or imbalance
Mechanical changes in neural function relative to cranial or cervical distortion
The number of treatments were from 1 to 9 with a mean of 4. These manipulations typically involve the hyoid bone, TMJ or cervical spine. Exclusive breastfeeding was reached in 78% based on a 10 point numerical scale and discussion with families.
Interestingly the frequency of birth trauma was notably higher in these patients than in the general population, which is used as an argument to suggest that these infants were at risk of injury in need of manipulation.
I have to give credit to the authors of this paper as they presented this information but acknowledged that the improvement in breast-feeding rates could be a function of allowing time for the skill to develop as opposed to the effect of their treatment. The only other study I located was a similar case series from 2012 looking at 19 patients showing similar improvements. The problem though in all of this is the lack of blinding of the interventions. Families that seek out a Chiropractor as they have already seen a lactation consultant, midwife and physician are clearly dedicated to the plan of breastfeeding and are motivated to take that extra step to achieve it. Whether the manipulations provided were effective or it was simply the result of dedication and time one will never know but I suspect that may be the case.
An additional factor that is worth mentioning is that with a higher rate than in the general population of birth trauma it is plausible that the delay in initiation of breastfeeding is related to after effects of birth as opposed to any true subluxation whether true or not.
Lastly one significant concern with respect to manipulations of the head and neck despite being well intended is the risk although small of vertebral artery dissection and stroke. This has been reported in adults and only once in Pediatrics but all families need to ask whether the proposed benefit is worth the small risk of a significant neurologic injury. My bias as you can probably guess is that implementing unproven therapy that carries a small but devastating risk is not worth it.
There is no doubt that the literature will become scattered with such case reports showing the benefits of Chiropractic care in achieving breast-feeding but my suggestion is to give it time. If it is meant to happen it will and exposing your infant to manipulation of the hyoid bone or neck is too fraught with danger to be worth pursuing.
The benefits of antenatal steroids before preterm birth have been clearly demonstrated in the literature and have been nicely summarized in a Cochrane Review. From this report the evidence is clear. Treatment with antenatal corticosteroids prior to preterm birth is associated with an overall reduction in neonatal death (relative risk (RR) 0.69, 95% confidence interval (CI) 0.58 to 0.81, 18 studies, 3956 infants), RDS (RR 0.66, 95% CI 0.59 to 0.73, 21 studies, 4038 infants), cerebroventricular haemorrhage (RR 0.54, 95% CI 0.43 to 0.69, 13 studies, 2872 infants), necrotising enterocolitis (RR 0.46, 95% CI 0.29 to 0.74, eight studies, 1675 infants), respiratory support, intensive care admissions (RR 0.80, 95% CI 0.65 to 0.99, two studies, 277 infants) and systemic infections in the first 48 hours of life (RR 0.56, 95% CI 0.38 to 0.85, five studies, 1319 infants).
While it is clear that corticosteroid administration prior to 37 weeks has great benefit, the question is whether these benefits might actually extend to 37 and 38 weeks. It has been known for some time that having an elective c-section before 39 weeks exposes the infant to an increased risk of pulmonary morbidity and NICU admission. In 2009 Tita At et al studied 24077 repeat elective c-sections at term finding that 36% were performed prior to 39 weeks. The findings conclusively demonstrated that delivery at 37 and 38 weeks increased the likelihood of a composite outcome of death or respiratory complications, treated hypoglycemia, newborn sepsis and admission to the NICU. Interestingly one can also see that after 40 weeks these complications rose again. Post term deliveries are not without their consequences either.
Broken down by outcome, it is also clear that each component has an increased risk at both 37 and 38 weeks compared to delivery at 39 or 40 weeks.
With such increased risk this practice has been discouraged by many obstetrical organizations including the American College of Obstetricians and Gynecologists.
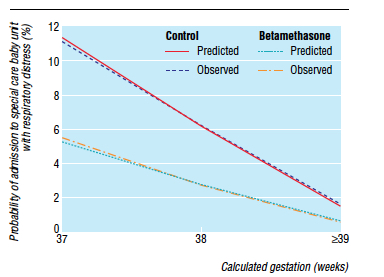
Knowing that there is clear benefit to providing corticosteroids before 37 weeks, it was only a matter of time before someone would test the hypothesis that treatment of women having an elective c-section in would reduce the incidence of respiratory complications such as TTN and RDS. Surprisingly there is really only one relevant study on this subject performed by P. Stutchfield et al in 2005 entitled Antenatal Betamethasone and Incidence of Neonatal Respiratory Distress After Elective Caesarean Section: A Pragmatic Trial. The trial provided betamethasone as a single course of two doses 24 hours apart starting 48 hours before a planned c-section with 998 participants in total.
The primary outcome in this trial was admission to NICU with respiratory distress. While the study was unblinded, the results were impressive and shown in the figure to the right indicating that below 39 weeks there was a significant difference in likelihood of admission for respiratory distress if women were treated with betamethasone prior to elective delivery via c-section. In terms of effectiveness this translates to the need to treat 37 women at 37-38 weeks with betamethasone to prevent one admission for respiratory distress to NICU. Eighty percent of the newborns in the control group had TTN versus RDS so I would expect you would need to treat about 200 women to prevent one case of RDS at this gestational age. Is it worth it? I suspect if you told parents that you could prevent hospital admission of their newborn at all many would choose to do so. There is another side to this though that one must consider and that side is the impact on neurodevelopment.
Corticosteroids work by overcoming the maternal capacity to break down cortisol by a placental enzyme 11β-hydroxysteroid dehydrogenase type 2 (11β-HDS-2). Furthermore the corticosteroids used (betamethasone and dexamethasone) are resistant to degradation by this enzyme. In the brain this enzyme exists as well and has increased activity such that levels of active cortisol in the brain are at a minimum. In animal models, high levels of glucocorticoids cause decreased brain differentiation with reduced neurogenesis. These processes are likely to be similar in humans given the presence of the same enzyme which has little effect in inactivating these synthetic medications.
Even with this knowledge, we as health care providers freely recommend antenatal steroids to women at risk of preterm birth for all the benefits outlined at the start of this post. Preterm infants are at significant risk of IVH, PVL, NEC, PDA and many other conditions which in and of themselves have been linked with adverse neurodevelopment. It is the avoidance of these outcomes which likely explains why corticosteroid administration with it’s known effect on the developing brain leads to improved neurodevelopmental outcome. The challenge here is that can we extrapolate this to the 38 and 39 week fetus? I would suggest that this is not the case as the risks of the conditions leading to neurodevelopmental impairment are magnitudes less. We are then exposing these fetuses to the potential harm or glucocorticoids without the benefit of reducing the conditions that matter to outcome. On the other side of the scale is a reduction in TTN/RDS and admission to the NICU but is it worth treating 37 mothers to avoid this with the heavy weight on the other side?
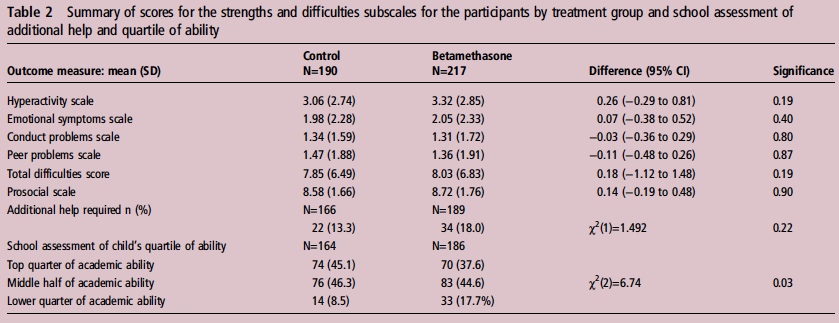
If you believe I am making some unfair assumptions it is worth seeing what happened to the patients in the 2005 study by Stuchfield when they were followed up between 8 – 15 years of age. The study used a questionnaire to address a number of outcomes related to education, atopy and behaviour. The response rate for the study was only 51% of the original cohort so any conclusions must be taken with a grain of salt. That being said the authors state that there were no differences in outcome or difference in rates of asthma and atopy. In their conclusion they affirm that based on the lack of differences in long-term outcomes but with improved short-term respiratory status at birth steroids should be provided before elective c-sections. Curiously though the authors do not address an interesting finding shown in table 2 from the article.
Looking at the bottom section pertaining to the school’s assessment of a child’s academic ability, less children in the steroid group performed at the top quarter of the class and twice as many children were in the lower quarter of the class. To me at least it seems disingenuous to claim no differences were seen when clearly here is a difference based on a third-party (the teacher) that is significant. The academic purists will be quick to point out that this is a secondary analysis and not the primary outcome specifically of the study and that the numbers are small. Additionally one can also argue that at a 51% response rate we are missing a great deal of outcomes. Furthermore it may well be that when it comes to surveys, those who have concerns about their participation in the study may be more apt to complete it skewing the results.
I will allow all these arguments as it really helps to support my conclusion on all of this. There is very little data out there on the benefit of providing antenatal steroids at term before elective c-section. The data out there for long-term effects does show a concern regarding school performance and the exposure in this case is to medication which is known to have effects on the developing brain. That data though is suspect as well given the issues raised in the above paragraphGiven the number of women that need to be treated to avoid one admission for respiratory distress and with the above mentioned concerns I believe more studies are needed to determine whether this is worth instituting as standard practice. Finally, any future studies will need to address in a prospective manner using a large number of patients whether there is indeed any impact on development in the long-term from such practice.
Go to any NICU these days and you will no doubt hear about the toxicity of oxygen. Oxygen as we say is a drug and like any such product has both good and bad effects. On the good side is the ability to increase the fraction of inspired oxygen to deal with transient changes in observed saturations. In extreme cases where the patient is desaturating into the 20’s and 30’s with accompanying bradycardia this can be life saving. On the other hand the “bad” is related to toxicity from oxygen free radicals which can increase rates of ROP, BPD and in the case of resuscitation with O2 vs room air may increase the chances of death.
It is for this reason that NICU teams pay particular attention to saturation targeting. The optimal goal remains elusive as oxygen restriction to 85-89% has been linked to higher mortality as in the Support Trial (full article) while higher saturations may increase the rate of ROP and BPD. Many units are falling somewhere in the middle such as goals of 90-95% or as in our units 88-93%. If during your visit to an NICU you were to observe the nurses at the bedside you would see them or the Respiratory Therapists tweaking the oxygen up and down many times a day as they strive to keep the saturations within these ranges. As a Neonatologist I greatly appreciate the efforts of everyone on the team who try to keep maintain these goals but in the end how do they really do?
This was the subject of a 2006 paper by Hagadorn et al. Eighty four infants from 14 centres all less than 28 weeks were enrolled in this study looking at how successful staff were at keeping infants within a desired range. The findings were somewhat discouraging in that 16-64% of the time saturations were in range, while 20-73% of the time they were above range depending on the centre studied. In a different study by Laptook et al published in the same year, the results were not much better with saturations higher than goal about 15% of the time and lower by nearly 26% of the time. What impact might swings in oxygen saturation have on the brain when the saturations are low and similarly on rates of BPD and ROP when the tendency is to overshoot the goals? There is no doubt that everyone is trying to do a good job but how deflating is it to nursing and other staff members when despite their best efforts they are only in range about 60% of the time?
Fortunately I believe change is coming. With improvements in technology it is now possible to have a closed loop system in which a patient who is receiving oxygen has their saturation measured and the information via a feedback loop triggers an automated response. This response either raises or lowers the FiO2 in an automatic way which eliminates the need for health care staff to make such changes. Such technology is actually not that new as it was tested in 2001 by Claure et al and was found to be at least as effective as manual changes by a dedicated nurse. Several other small studies followed, all demonstrating an improved accuracy in maintaining target saturations. This July the same group published the following article Automated versus Manual Oxygen Control with Different Saturation Targets and Modes of Respiratory Support in Preterm Infants. This study compared the accuracy in maintaining saturations using a target of 91-95% and another of 89-93% with 80 patients participating. Patients in this study received both invasive and non-invasive ventilation. When comparing the two target ranges the automatic adjustments showed greater benefit with the results being 62 +/- 17% vs 54 +/- 16% for the 91-95% range and 62 +/-17% vs 58 +/-15% in the lower range. Both of these results were statistically different with p values of <0.001. When looking at episodes of significant hypoxemia as defined by a saturation < 80% the findings were interesting showing in the high range 13 vs 4 and in the low range 15 vs 4 favouring the use of autosaturations. The authors were surprised at the lack of large disparity in the accuracy between manual and auto adjustment of FiO2 but this may be related to the Hawthorne effect. Since the nurses in this study were not blinded to the intervention they may have changed their behaviour in essence to try and prove that they were just as good. How this would translate into a real world situation when a study is not being performed I suspect would favour the automated system more.
Perhaps the most interesting part of the study though was the number of Manual FiO2 adjustments per 24 hours between the two groups. For the 89%-93% SpO2 target range this was 1 [0-3] vs 102 [73-173], P < .001 and for the 91%-95% SpO2 target range 1 [0-3] vs 109 [79-156], P < .001. For me this is the crux of the discussion. In a twenty four hour period there is a reduction of about 100 interventions using the saturation range similar to our own. Take note as well that some patients required over 150 interventions in 24 hours as 100 was the mean! While the targeting is improved somewhat with the use of the auto FiO2 adjustment this is where the biggest benefit to the patient lies as I see it. Nurse and respiratory therapists are very busy on any given shift. One hundred adjustments a day translates into 4 changes in FiO2 per hour on average. Although not measured I can’t help but wonder what impact these interruptions have on the rest of the care for a given patient. What is the “ripple effect” of such interruptions in a person’s train of thought. Could this translate into a med error or delay care for another patient to whom the nurse is responsible for as well? If one didn’t have to pay as much attention to the FiO2, what other goals could their attention be put towards? Might this provide them with more time to educate parents, do skin care, or a host of other responsibilities which in the current state get interrupted every time an alarm goes off.
As this technology is improved I see this being a welcome addition to the NICU. As with anything though that promises a hands free environment it will be essential to have an override built in. Furthermore we can never take our eyes off the patient as no matter how safe these systems may be there is always the chance that a computer will freeze as we all know. The impact of such a “glitch” in the algorithm that these systems use could be catastrophic to outcome so as good as these may be we will always need the human presence to ensure that what we think we are getting from the system is actually there.
Living in Canada we are privileged to have a universal health care system. Privileged in the sense that all citizens are entitled to the same level of care regardless of economic circumstance although the monetary costs to the tax payer is another story and forms the basis of most arguments in the US against adopting such a system down south. My goal of this post though is not to enter into a debate about which system is superior but rather speak of the dollars and cents attributable to being born too early or too small.
In the US such measurements are simpler as costs are more easily measured in a private health care system but each health care region in Canada can measure to a certain degree the costs associated with a hospital stay. Certainly the story of Raquena Thomas made this clear to me. In 2007 she was born in Edmonton after her mother left Jamaica for a visit with family in Edmonton. After delivering she was found to have hypoplastic left heart syndrome (HLHS) and went on to have the first stage of the Norwood procedure. What followed was a bill to the mother for $162576 and for commentary on the discussion that ensued about who should pay the bill see the article here. As I was working at the Stollery Children’s Hospital at the time and cared for this infant it was clear to me after this experience that the hospital indeed has a clear method to calculate costs even if we the taxpayer are blind to such calculations.
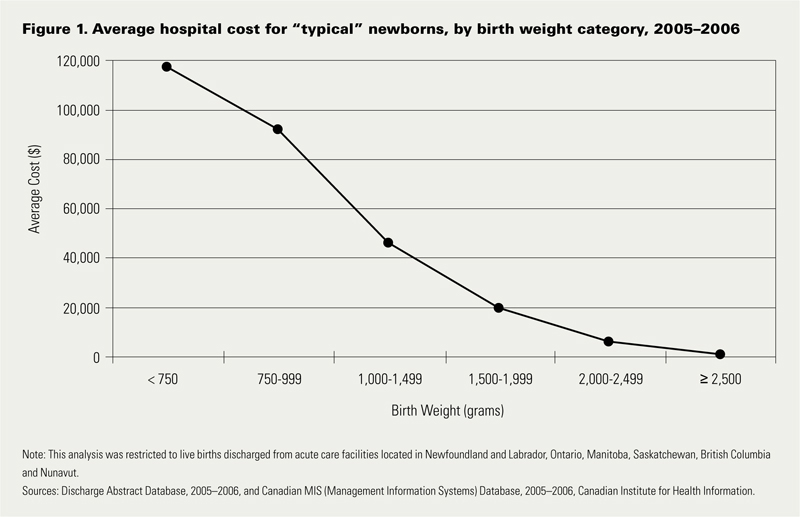
Now HLHS is a condition that affects very few infants a year in any given province but what about low birth weight and preterm birth? This as we say in Neonatology is our bread and butter. In 2009 Lim et al published data on the Canadian population in attempt to ascertain the health care costs for these groups of patients (CIHI survey: Hospital costs for preterm and small-for-gestational age babies in Canada)
In this period 1 in 7 babies was born either preterm or small for gestational age. If specifically looking at infants < 2500g defined as low birth weight this represented 6% of all babies born. When you factor in that there were 350000 babies born in that year in Canada we are looking at about 21000 babies nationally. Looking at the costs for these infants one sees a direct relationship between decreasing birth weight and increasing costs in the hospital. This should not be surprising to anyone. It should be noted though that the paper provides average costs only without standard deviation or ranges. As you would expect, the costs for a patient with severe HIE or NEC would be higher than the 26 week infant who has a very smooth course and does not have a symptomatic PDA, severe IVH or any other significant disability during their course.
The data looking at such costs is scare with respect to the Canadian landscape and even more difficult to determine has been lifetime costs or at least incremental costs after leaving the hospital environment. I was delighted to see that former colleagues of mine in Edmonton have published a new paper examining both the extent of health service utilization (HSU) attributable costs in the year following discharge of both LBW and normal birth weight peers in Alberta (abstract here). Not surprisingly, smaller babies have more medical needs. In this study LBW patients had an average of 5.9 outpatient services and 1.1 visits to the ER in the first year of life compared to 2 and 0.9 in the normal birth weight peers. Physician services were double with 22.7 office visits compared to 11.9 in the NBW group. The costs to the Health Care system overall are represented in the table below which demonstrates that the LBW infants make up 37% of the total health care costs of newborns yet represent only 6% of the population. In terms of risk factors for LBW they were high prepregnancy weight, aboriginal women and low socioeconomic status. Efforts to lessen the incidence of the first and third factor in our pregnant population would be a good target for public health efforts. Bear in mind that the costs outlined below are in addition to the costs in the hospital.
BW Category
Cost per patient
Patients
Cost to System (millions)
NBW
$3,942
43207
182
LBW <2500
$33,096
3123
108
1500 – 2499g (MLBW)
$20,467
2571
53
1000 – 1499g (VLBW)
$83,895
278
23
< 1000g (ELBW)
$117,546
274
32
The analysis provided in this paper does not specify out the costs by certain conditions such as NEC or BPD so all we have to go on are averages for HSU and cost. It does however raise a point which I believe is crucial to any discussions with respect to expanding programs within the hospital. We need to refocus administration at both the hospital level and at the funding source (our provincial governments) as to the true costs of the conditions that we are trying to prevent. It is only through looking at the costs of both the hospitalization and after discharge that we can truly come to understand the cost effectiveness of expanded programs or new treatment modalities.
Donor breast milk is one that I believe serves as a good example of a program that is in need of expansion in many places in the country but is hampered by the perception of high up front costs. The average cost of this milk is about $4 per ounce. I will simplify the math a little as there would be a phase of escalating the volume per day and a wean at the end but let’s say we have a 1.5 kg infant that we want to treat with DBM for a period of 4 weeks. The cost to do this assuming a TFI of 150 mL/kg/d would be a little over $800 per patient so with the increasing phase, wean and adjusting for some weight gain let’s say $1000 per patient. If there were 200 such patients in your hospital each year the annual cost would be $200000 which on the surface seems like a lot of money. From the most recent cochrane review though comparing formula to donor milk the risk ratio to develop NEC is 2.77 meaning that a preterm baby who receives formula is nearly three times as likely to develop NEC. Ignoring differing rates of NEC by hospital let’s just use the concept that we could prevent one case of NEC a year with such a strategy. The cost of medical NEC is somewhere between 100-140K while surgical is 200 – 240K. The in-hospital costs of preventing just one case nearly pay for or exceed the cost of the entire years supply of DBM. If you add to this the cost of the following years of physician visits, consultants, testing, special diets and investigations and procedures these patients receive the costs are more than covered from just one patient.
Health care budgets are no doubt a difficult thing to balance but the point of all of this is that when determining whether to spend our precious health care dollars we must look at not only the impact during the hospitalization but for years after if we truly modify future risks as well.
This is a lengthier piece than normal but the message at the end is critical to disseminate so I would encourage you to share this if you wish with others to prevent misinformation from being propagated in the media by the sensationalism of a claim by a group of Pediatricians.
My Facebook page became awash in rainbow overlaid posts on Friday. Very quickly I realized as did most of the developed world, that the US Supreme Court ruled in favour of same-sex marriage and just so no one thinks that this will turn into a homophobic piece, I celebrated the change along with many friends and fellow Social Media colleagues.
After the initial excitement began to wane I came across a press release that I found a little shocking given that I belong to the group of people (as a Pediatrician not a member of the organization) that released the statement shown below. The statement is from the American College of Pediatricians
Dr. Michelle Cretella, President of the American College of Pediatricians in response to the SCOTUS decision today stated, “[T]his is a tragic day for America’s children. The SCOTUS has just undermined the single greatest pro-child institution in the history of mankind: the natural family. Just as it did in the joint Roe v Wade and Doe v Bolton decisions, the SCOTUS has elevated and enshrined the wants of adults over the needs of children.“
Although it is disappointing only 4 of the 9 justices heeded the scientific findings in the College Brief, the College will continue to proclaim the important unique contributions of both mothers and fathers to the optimal nurturing of all children.
As I went to their website and read about this organization it became clear that this group is mixing Church and State so to speak. Their mission statement states:
Mission of the College
The Mission of the American College of Pediatricians is to enable all children to reach their optimal physical and emotional health and well-being. To this end, we recognize the basic father-mother family unit, within the context of marriage, to be the optimal setting for childhood development, but pledge our support to all children, regardless of their circumstances.
Who are these people and why are they speaking out in such contrast to the American Academy of Pediatrics who in 2013 published their technical report in support of same-sex couple raising children. The AAP which has about 64000 members dwarfs the membership of possibly 200 Pediatricians that comprise the American College of Pediatricians. The smaller group was formed when a group of Pediatricians became upset in 2002 of the AAPs position that endorsed same-sex couples adopting children. The trouble of course with an organization such as this is that their name implies some degree of credibility but in looking at their track record on this issue they have little to none. They are a group that seems to ignore the literature discussed below in favour of quasi-scientific religious literature suggesting harm from such family units. The support of the AAP, the dominant organization in the field was made clear June 26th with this statement. I particularly like the quote from the president of the AAP.
“Every child needs stable, nurturing relationships to thrive, and marriage is one way to support and recognize those relationships,” said Sandra G. Hassink, MD, FAAP, AAP president. “Today’s historic decision by the U.S. Supreme Court supports children in families with same-gender parents. If a child has two loving and capable parents who choose to create a permanent bond, it’s in the best interest of their children that legal institutions allow them to do so.”
Putting aside my natural suspicion of the American College of Pediatricians, it did lead me to ask an important question. Are kids truly better off being raised in a heterosexual marriage? Perhaps there is evidence to show that indeed this is something that we as Pediatricians should be promoting. Looking at the evidence though would suggest otherwise or at least that there is no difference. In 2014 the largest study to date was published by Australian researcher Crouch et al involving 315 parents representing 500 children from same-sex marriages (complete study here). The study involved a questionnaire that would then be compared against population data to see if differences exist between parental units. A little over two-thirds of the parental units were Lesbian. The results demonstrated that in virtually all measures of child health the parental units were equivalent. Curiously, sense of stronger family cohesion was present with the same-sex groups. Possible reasons for this may be related to the way in which children are brought into this world in the two parental unit types. Given that people of the same-sex must plan (there are exceptions no doubt) to procreate there is little chance of the unexpected pregnancy occurring. These are almost all “wanted or chosen” children as opposed to the situation encountered in many pregnancies that are not planned. That is not to say that these children can’t or won’t be loved but the likelihood seems much lower in a LGBT parenting situation due to the planning that is generally required. While the research did not go on to elaborate on why the cohesion might be enhanced this is just my speculation.
Adding to this piece of evidence that these children are likely to have equivalent health to the traditional family rearing model is a well-timed report that surfaced the same week as the Supreme Court Ruling. The report from the Huffington Post challenges that after reviewing 19000 studies on same-sex parenting there can be no conclusion that the children of such families are worse off in any measure of health. Where the above group derives their mission statement from then is certainly not based on science but rather perception.
Back to the American College of Pediatricians (ACOP). I mentioned earlier that I was suspicious of the ACOP and what they portray as advocating for a child’s best health. As a writer of a blog I firmly believe that the buck stops at me with respect to content. If I have a guest writer I am responsible for their content as well as my own. I took the liberty of reviewing a recent piece from their blog and what I saw both shocked me and left me with the certainty that this group is not so much advocating for the health of children as condemning those lifestyles that they do not believe fit the mother-father mold. On June 5th the group released the following piece entitled “P” is for Pedophile. Please click on the link if you have the stomach for it but to give you a taste of what they are talking about here is the quote from the first line of the entry.
“Driving in this morning I began to wonder. Why isn’t the movement of LGBT not the PGBT movement: “P” for pedophile?”
If this group had any credibility by having a professional sounding name, my hope is that this post will spread wide and far to help discredit this organization. The evidence suggests that members of the LGBT community raise just as healthy kids as any of us and any attempts to smear people simply for who they happen to bond with for life amounts to hate and there should be no room in Pediatrics or any other field of medicine for that.
The following piece is by guest writer Nicole Sneath NNP at the University of Manitoba. I am delighted to have her write on the use of simulation in the NICU and encourage you to watch the video she made for a recent charitable luncheon for the Children’s Hospital Foundation of Manitoba.
Practice makes perfect. This is something we’ve all heard at one point or another. Whether it was when we were learning how to ride a bike without training wheels, or print our name, or pitch that perfect strike. It seems a basic lesson, common sense, but do we practice what we preach?
In health care we deal with stressful situations, complex syntheses of information and multiple unique interactions. For the most part, we work in interprofessional teams, each one responsible for some part of care to our patients and each one dependant on the other whether we like to admit it or not. Our groups are varied, ranging from hands on direct care providers, to consultants, support staff, administrators and maintenance workers. Each one plays a unique role complementing the other. Sounds like the perfect set up. In practice however, do we really complement each other? Do we communicate effectively? How often do things fall through the cracks? Do we use our skills and strengths to everyone’s advantage? Is this diverse system a well-oiled machine working together and collaborating to provide optimal patient care? I would guess if you looked at your organization critically you may not be happy with all the answers.
Most of us trained and practiced with members of our own profession, doctors with doctors, nurses with nurses and so on. We were hired into our jobs and again did our orientation and continuing education within our own groups. In the everyday workplace however we are all blended together, modeling those that have practiced before us. Sometimes we work together well, seamlessly collaborating for a common goal. When we don’t, who pays the price? Perhaps it’s the patient with an untoward outcome, perhaps its the administrator with a complaint on their desk, perhaps its the consultant frustrated by the miscommunications or perhaps it’s the staff member not satisfied or content with their work.
Training programs have started to recognize that collaboration needs to start at the beginning. Waiting to introduce these concepts until arrival into the workplace is too late. Interprofessional learning is defined as learning with, from and about each other and this should happen at all levels of education and training. Teams function well not only by practicing together, but by creating environments where teams can get to know each other. Creating a relationship, no matter how small, can go a long way when stress increases and trust is needed.
It’s been shown that errors are often caused by breakdowns in communication. Maybe the nurse that administered the wrong dose of medication just didn’t know the dosing for that particular medication? Solving the problem could be teaching the proper dose and voila, problem solved. Or was the problem that they didn’t know where to find the information, weren’t comfortable asking for help, or didn’t want to question the doctor that ordered it? When the surgeon amputates the wrong leg is it because that one surgeon just isn’t that bright? Or could it be that no one else in the operating room double-checked, no one spoke up when they thought-wait, was it the left or the right, each one assumed that someone else must know best? Speculations abound for what goes on in critical incidents such as these. A common thread in preventing many critical incidents is the need for improved communication. Closed-loop communication, a shared mental model, role identification and clear leadership are integral to good communication in stressful situations. These concepts are best taught through experience rather than didactic lectures alone. So how do we go about teaching these skills?
Practice. Practice in an environment that is like the real thing, but lacks the risk to patients. Gone is the see one, do one, teach one mantra but it is replaced by see many, simulate even more, then do. Simulation allows us to breakdown specific skills and practice them over and over until we master them. We can practice individually or to harvest the greater benefit we can bring our interprofessional groups together and practice the skills that can’t be taught by reading a book. We can video record the sessions and debrief them afterwards. Instead of debriefing by giving a reassuring pat on the back or a not helpful shaming, perhaps we should try the “debriefing with good judgement” method and gain insight into the frames that guide individuals behaviour and actions. We can stop asking “dirty questions”-you know, the questions that we ask when we already know the answer, the “guess what I’m thinking” questions. Instead we can develop true curiosity into what individuals are thinking and then be able to change behaviour and facilitate critical thinking and problem solving.
We all come to work and want to do a good job. We want to be told that we made a difference, that something we did during the day has made a positive contribution to someone’s life. If this doesn’t resonate then perhaps a change in occupation is in order. If we critically examine our own practice, we would find areas that we could improve, skills we wish were a little more precise, or areas of specialty that we wish we knew a little more about. Traditional responses would be to dust off an old textbook or perform a literature search and get the information we need. Is this manner of learning effective? Does this address all the skills and knowledge we are seeking? Do we really know our areas of weakness? Do we want to?
References
1. There’s no such thing as “nonjudgemental” debriefing: a theory and method for debriefing with good judgement. http://www.ncbi.nlm.nih.gov/pubmed/19088574
2. Debriefing with good judgement: combining rigorous feedback with genuine inquiry.


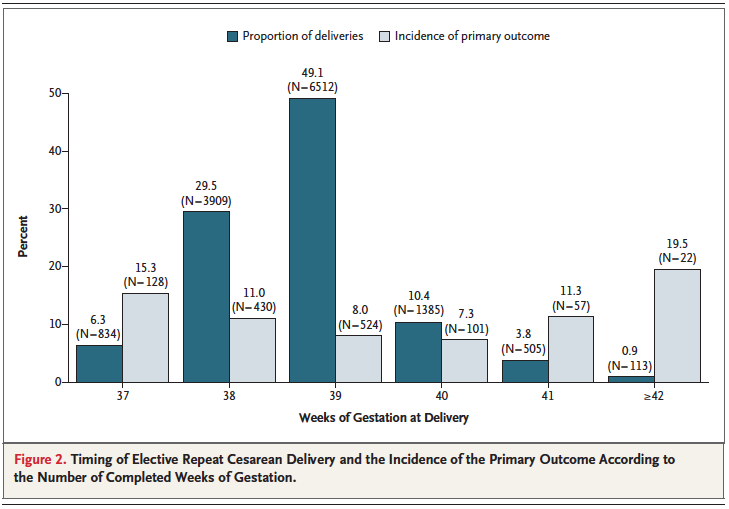 Interestingly one can also see that after 40 weeks these complications rose again. Post term deliveries are not without their consequences either.
Interestingly one can also see that after 40 weeks these complications rose again. Post term deliveries are not without their consequences either.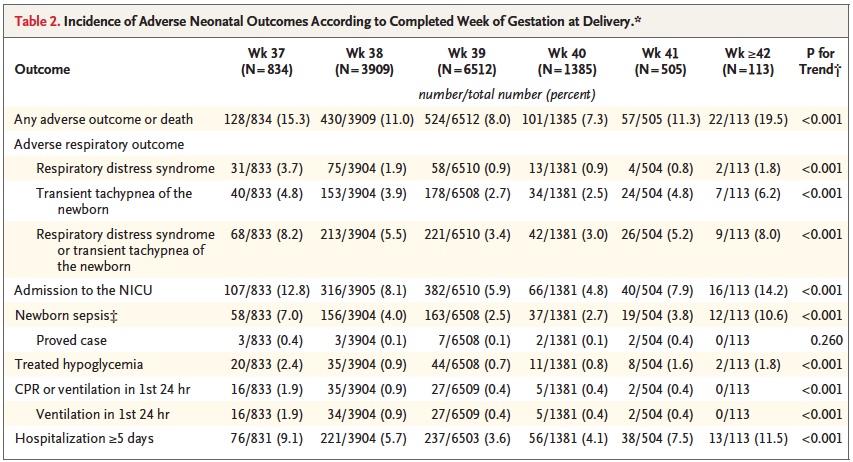


 Looking at the costs for these infants one sees a direct relationship between decreasing birth weight and increasing costs in the hospital. This should not be surprising to anyone. It should be noted though that the paper provides average costs only without standard deviation or ranges. As you would expect, the costs for a patient with severe HIE or NEC would be higher than the 26 week infant who has a very smooth course and does not have a symptomatic PDA, severe IVH or any other significant disability during their course.
Looking at the costs for these infants one sees a direct relationship between decreasing birth weight and increasing costs in the hospital. This should not be surprising to anyone. It should be noted though that the paper provides average costs only without standard deviation or ranges. As you would expect, the costs for a patient with severe HIE or NEC would be higher than the 26 week infant who has a very smooth course and does not have a symptomatic PDA, severe IVH or any other significant disability during their course.
