
by All Things Neonatal | Aug 5, 2016 | Uncategorized
There may be nothing that is harder in medicine. We are trained to respond to changes in patients condition with a response that more often than not suggests a new treatment or change in management. Sometimes the best thing for the patient is in fact to do nothing or at least resist a dramatic response to the issue in front of you. This may be the most common issue facing the new trainee who is undoubtedly biased towards doing something. Take for instance the situation in which the trainee who is new to the service finding out that their 26 week infant has a PDA. Their mind races as they digest this information from morning signover. There is less than 2 hours until they come face to face with their attending who no doubt will ask them the dreaded question. “What are you going to do about it?”. When having to choose a path, if they state “I want to sit tight and watch” they fear the thought of the attending thinking they don’t know what to do. Conversely they could stick their neck out and choose to treat with a variety of approaches but then might they be seen as too aggressive?! The likely path is suggesting treatment but in fact the more I think about it the option of benign neglect may be the best approach or at least one in which if you treat and it doesn’t work the first time you just shrug your shoulders and say “I’ll deal with it till it closes on it’s own”.
This post really is a follow-up to a previous one entitled The Pesky PDA. A Puzzle After All These Years. What triggered this writing was another before and after comparison of two periods in which the management of PDAs for a unit took a 180 degree turn.
Know When to Hold Em And No When to Fold Em
This is the essence of the issue for one unit. Sung SI et al published a paper this month entitled Mandatory Closure Versus Nonintervention for Patent Ductus Arteriosus in Very Preterm Infants. They describe a before and after comparison of 81 infants from 2009-11 and 97 infants from 2012-14. All babies were born between 23-26 weeks gestational age. In the first time period their unit had a mandatory PDA closure policy. That is they gave one course of indomethacin and if possible a second course followed by surgical ligation. A significant PDA was defined as one that had a left to right shunt and was at least 2 mm in diameter and the patient had to be ventilated. Any patient who had been extubated regardless of need for CPAP did not have to have their PDA closed. In the second time period the group attempted to avoid indomethacin and ligation at all costs and in fact in this cohort none received either.
So What Happened?
In the first time period 52 (64%) received indomethacin but only 29% responded and a full 37/52 (71%) went on to receive surgical ligation. Of the 29 that did not receive indomethacin due to contraindications they underwent primary ligation for a total of 82% receiving surgical ligation. The average day of closure for period 1 was 12.9 days.
In period 2 a number of interesting findings occurred. The average day of closure was at 44.2 days. Five infants were discharged with a PDA with 3 experiencing spontaneous closure after discharge and the remaining infants undergoing transcatheter occlusion. In period 2 there were more diuretics and fluid restriction employed. Comparing the two periods for a number of other outcomes reveals some other intriguing findings.
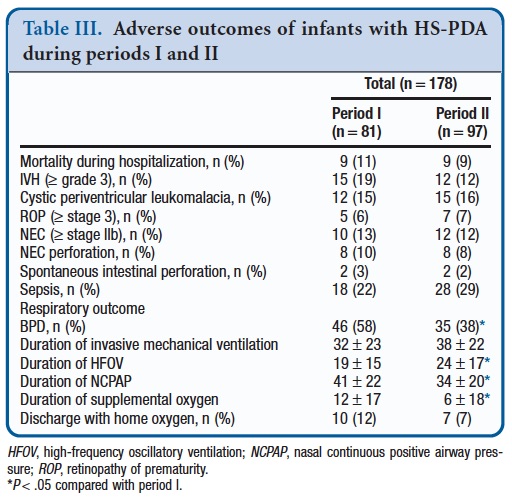
Even with such differing approaches there is no difference in mortality, severe IVH, ROP, PVL, NEC or sepsis. What is different though is the diagnosis of BPD yet there is no difference in total ventilation. In period 2 there is a shift towards more of this ventilation being HFOV less CPAP use at the same time.
What Might It All Mean?
It is retrospective and therefore we cannot be certain that there are not other variables that are not affecting the results that would have had a better chance of being evened out in an RCT. Having said that it is intriguing that having a PDA has been associated with BPD in the past but in this study having a PDA for a longer time is associated with a reduction in BPD. We know that longer periods of invasive mechanical ventilation increase the risk of developing BPD so it is intriguing that that there is no difference in mechanical ventilation yet there is more BPD when you are aggressive with the PDA. You might postulate that the need for surgery leads to greater need for ventilatory support and therefore damages the lungs but the needs for HFOV was higher in the second phase which at least hints that in terms of aggressiveness, Period 2 infants had a tougher go.
The culprit may be the heart. In period 1 there was a significantly increased rate of myocardial dysfunction and need for inotropes following ligation. It could well be that left ventricular dysfunction led to pulmonary edema such that in the 24-28 hours after the surgery ventilator requirements were increased and damaged the lung. The lack of a difference in overall ventilation days supports this possibility. Looking at the other common risk factors for BPD such as chorioamnionitis and lack of antenatal steroids these are no different between groups. Although not statistically significant there are more male infants in period 2 which would usually tip the scales towards worse outcome as well. It does need to be stressed as well that the rate of surgical ligation is higher than any study I have come across so the contribution of the surgery itself to the disparate outcome needs to be seriously considered.
What would I do?
Despite this study and some others that have preceded it I am not at the point of saying we shouldn’t treat at all. Our own approach is to give prophylactic indomethacin to such babies and then for the most part if a PDA remains treat one more time but at all costs try and avoid ligation. An RCT sounds like it is in the works though comparing the two approaches so that will certainly be interesting to see. It is tough to say what the future holds but to any young trainees who are reading this, the next time you are asked what to do about a PDA you are well within your rights to suggest “Maybe we should do nothing”!

by All Things Neonatal | Jun 30, 2016 | nutrition, Uncategorized
Breast milk has many benefits and seems to be in the health care news feeds almost daily. As the evidence mounts for long term effects of the infant microbiome, more and more centres are insisting on providing human milk to their smallest infants. Such provision significantly reduces the incidence of NEC, mortality and length of stay. There is a trade-off though in that donor milk after processing loses some of it’s benefits in terms of nutritional density. One such study demonstrated nutritional insufficiencies with 79% having a fat content < 4 g/dL, 56% having protein content< 1.5 g/dL, and 67% having an energy density < 67 kcal/dL (< 20 Kcal/oz). It is for this reason that at least in our unit many infants on donor milk ultimately receive a combination of high fluid volumes, added beneprotein or cow’s milk powders to achieve adequate caloric intake. Without such additions, growth failure ensues. Such growth failure is not without consequence and will be the topic of a future post. One significant concern however is that failure of our VLBW infants to grow will no doubt impact the timing of discharge as at least in our unit, babies less than 1700g are unlikely to be discharged. With the seemingly endless stream of babies banging on the doors of the NICU to occupy a bed, any practice that leads to increasing lengths of stay will no doubt slow discharge and cause a swelling daily patient census.
What if increasing volume was not an option?
Such might be the case with a baby diagnosed with BPD. Medical teams are often reluctant to increase volumes in these patients due to concerns of water retention increasing respiratory support and severity of the condition. While diuretics have not been shown to be of long term benefit to BPD they continue to be used at times perhaps due to old habits or anecdotal experiences by team members of a baby who seemed to benefit. Such use though is not without it’s complications as the need to monitor electrolytes means more needle sticks for these infants subjecting them to painful procedures that they truly don’t need. Alternatively, another approach is to restrict fluids but this may lead to hunger or create little room to add enough nutrition again potentially compromising the long term health of such infants.
Amy Hair and colleagues recently published the following study which takes a different approach to the problem Premature Infants 750–1,250 g Birth Weight Supplemented with a Novel Human Milk-Derived Cream Are Discharged Sooner
This paper is essentially a study within a study. Infants taking part in an RCT of Prolacta cream (Prolacta being the subject of a previous post) were randomized as well to a cream supplement vs no cream. The cream had a caloric density of 2.5 Kcal/mL and was added to donor milk or mother’s own milk when the measured caloric density was less than 19 Kcal/oz. The study was small (75 patients; control 37, cream 38) which should be stated upfront and as it was a secondary analysis of the parent study was not powered to detect a difference in length of stay but that was what was reported here. The results for the groups overall were demonstrated an impact in length of stay and discharge with the results shown below.
|
Control (N=37) |
Cream (N=38) |
p |
| PDA ligation % |
8.1 |
2.6 |
0.36 |
| PDA treated medically % |
27 |
29 |
0.85 |
| Sepsis % |
5.4 |
7.9 |
1 |
| NEC% |
0 |
0 |
– |
| BPD% |
32.4 |
23.7 |
0.4 |
| Death % |
0 |
0 |
– |
| Length of stay, days |
86+/-39 |
74+/-22 |
0.05 |
| PMA at discharge, weeks |
39.9+/-4.8 |
38.2+/-2.7 |
0.03 |
What about those with sensitivity to fluid?
Before we go into that let me state clearly that this group comparison is REALLY SMALL (control with BPD=12 vs cream with BPD=9). The results though are interesting.
|
BPD control (N=12) |
BPD cream N=9 |
p |
| Length of stay, days |
121 +/-49 |
104+/-23 |
0.08 |
| PMA at discharge, weeks |
44.2+/-6.1 |
41.3+/-2.7 |
0.08 |
So they did not reach statistical significance yet one can’t help but wonder what would have happened if the study had been larger or better yet the study was a prospective RCT examining the use of cream as a main outcome. That of course is what no doubt will come with time. I can’t help but think though that the results have biologic plausibility. Providing better nutrition should lead to better growth, enhanced tissue repair and with it earlier readiness for discharge.
One interesting point here is that the method that was used to calculate the caloric density of milk was found to overestimate the density by an average of 1.2 Kcal/oz when the method was compared to a gold standard. Given that fortification with cream was only to be used if the caloric density of the milk fell below 19 Kcal/oz where average milk caloric density is 20 Kcal/oz there is the distinct possibility that the eligible infants for cream were underestimated. Could some of the BPD be attributable to infants being significantly undernourished in the control group as they actually were receiving <19 Kcal/oz but not fortified? Could the added fortification have led to faster recovery from BPD?
Interesting question’s in need of answers. I look forward to seeing where this goes. I suspect that donor milk is not enough, adding a little cream may be needed for some infants especially those who have trouble tolerating cow’s milk fortification.

by All Things Neonatal | Nov 12, 2015 | Neonatal
In 2018 where do we stand on this question? Upcoming retrospective trials and work by EPIQ-4 may help to resolve this issue. In the meantime what does the existing evidence say?
The decision to extubate an extremely low birthweight infant is one of the most common sources of disagreement and anxiety in the NICU. As a resident, I recall an unwritten rule that “no baby under 750g will have a trial of extubation as they will most certainly fail”. As time went on however, studies suggested that not only is this a false statement but also that the duration of intubation was directly correlated with risk of BPD. As Danan described, for infants less than a 1000g, delaying extubation when they had reached minimal settings did not result in lower rates of BPD. Moreover 60 – 70% of infants who have such extubation attempts are not reintubated within a week, so it is possible to have success.
The detractors however express concern about the 30-40% who do require reintubation and worry that harm will be caused by such acts. Frequent concerns are voiced with respect to potential trauma to the airway leading to subglottic stenosis; potentially increasing the risk of BPD and finally the belief that attempts are futile so why put parents through the stress in the midst of perceived near certain failure. The problem with these perceptions however is that they are mostly the culmination of confirmation bias. Patients that have multiple failed extubations are remembered especially when they develop significant complications, while the ones who extubate successfully are quickly forgotten. This is not intentional in any way but simply a human tendency to follow the pattern of “the squeaky wheel getting the grease”. The preemies who do poorly are front and centre as they take up a great deal of our time & attention while the ones who do very well while celebrated, are not as easily remembered for the success they demonstrated when extubated.
Being someone who believes in extubating as soon as possible though I was surprised several months ago to find a paucity of data demonstrating that there was in fact support for the practice in terms of better outcomes being associated with early extubation. While small studies certainly pointed in that direction the real question was about to be answered in the study that follows.
Is it better to fail multiple times or be intubated once for the duration of ventilation.
This is the central question that I believe has been answered as good as it will ever be by EA Jensen et al in JAMA this past month “Effects of Multiple Ventilation Courses and Duration of Mechanical Ventilation on Respiratory Outcomes in Extremely Low-Birth-Weight Infants.” This retrospective review included 3343 infants below 1000g and examined the primary outcome of BPD and secondary outcomes of death, continued supplemental oxygen use at the time of discharge, and tracheostomy among survivors. As you might expect, regardless of whether one compared duration of ventilation or number of reintubations, variables such as need for surfactant, postnatal dexamethasone, PDA treatment and NEC became more common as exposure to either outcome increased. 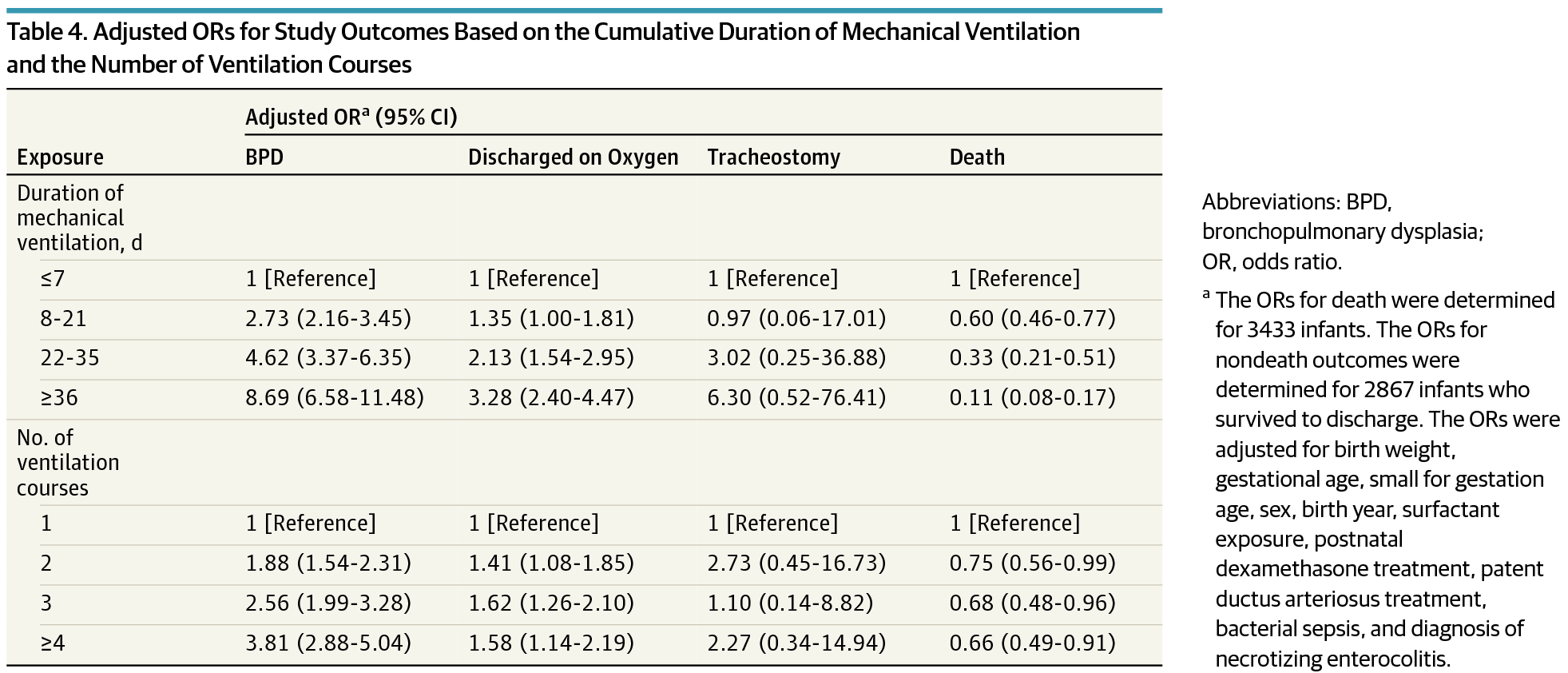 When a logistic regression model was applied though it became evident that the odds ratio for BPD increased to a much greater degree with increasing duration of ventilation than the number of attempts.
When a logistic regression model was applied though it became evident that the odds ratio for BPD increased to a much greater degree with increasing duration of ventilation than the number of attempts.
To quote the authors:
“After adjustment for the cumulative duration of mechanical ventilation, a greater number of ventilation courses was not associated with an increase in the risk-adjusted odds of supplemental oxygen use at discharge. The number of ventilation courses remained associated with increased risk of BPD only among infants exposed to 4 or more courses.”
The Needs of The Many Outweigh The Needs of The Few
In other words, for an infant to have an increased risk of BPD they would need to have failed extubation four or more times! It is not easy to predict with certainty who these children will be but if we take these findings as accurate (since I believe we will not see an RCT of this magnitude anytime soon) is it ethical to keep a child intubated due to the belief that they might fail? On the contrary, how can we not try when failure is not associated with adverse outcome? In fact none of the secondary outcomes were found to be increased either. Importantly, there was no difference in the need for a tracheostomy in this population which may serve as a proxy for lack significant airway injury from multiple intubations. The goal of this post is to provide all of us who care for these preemies with the reassurance that if they fail extubation, once, twice and even three times that is still a good thing. For the ones that fail more than that, if only we had a crystal ball we might have spared them that risk but given that we live in a world without this ability, we owe it to our patients to try. Moreover, we owe it to the parents of these children to educate them that failure can still be a good thing.
May I never have a near 100% success at extubating my patients on the first try. If I truly care for them I will embrace my failures and know that I have done the right thing.

by All Things Neonatal | Oct 8, 2015 | antibiotics
The literature over the last few years has ballooned with reports of adverse outcomes related to antibiotic overuse. The most common adverse outcome noted on the worldwide stage is that of antimicrobial resistance and the so-called “superbugs” but in the NICU a whole host of other outcomes have been noted. Prolonging antibiotics beyond the first couple days of life has led to changes in the microbiome towards more pathogenic bacteria in the NICU. This shift has been accompanied by a rise in the rate of necrotizing enterocolitis in such units as well as many outcomes including some which affect us as adults such as asthma, which has been discussed on my Facebook page before.
New Consequences of Prolonging Antibiotics Beyond 48 hours
This month a colleague with a particular interest in this story forwarded our team the following paper. Prolonged Early Antibiotic Use and Bronchopulmonary Dysplasia in Very Low Birth Weight Infants by Novitsky et al. What this retrospective study demonstrated (comparing 747 infants treated for less than 48 hours to 159 treated beyond) was that the prolongation of antibiotics beyond the first 48 hours was associated with increased propensity to develop BPD. This finding remained true even when factoring in other risks for such outcomes including gestational age, maternal antibiotics, inborn status, clinical chorioamnionitis, prolonged rupture of membranes, preeclampsia, cesarean delivery, Apgar at 5 minutes, SNAP score, and mechanical ventilation. Curiously it is not just the initial course that is of concern but ongoing exposure as well. “After adding total cumulative hospital course antibiotic days, the odds of BPD remained increased with > 48 hours of antibiotic coverage in the 1st week. Furthermore, for every additional day of antibiotic coverage after the 1st week of life, there was an increased odds of developing BPD (OR, 1.16 per antibiotic day, 95% CI, 1.11–1.2). “
Prolonging antibiotics has another downstream consequence of increasing the rates of endotracheal tube colonization with bacteria to the tune of 38 vs. 16%. Additionally there was a shift in endotracheal tube culture patterns towards the emergence of resistant gram negative organisms (7% vs. 2%) if prolonged treatment up to 7 days was chosen. As has been shown in other studies rates of NEC were increased as well which should be no surprise based on previous similar work.
Wanting To Be Safe And Do The Right Thing
Once bitten twice shy as the saying goes. Any clinician who has missed an episode of sepsis in a newborn after not starting antibiotics is no doubt scarred to some degree. I have no doubt that all of us wish to do the right thing and protect the infants in our care when risk factors for sepsis indicate to us that there is a higher likelihood of sepsis being present. Looking at this study one can see the following risks were indeed more prevalent in the group treated beyond 48 hours.
| Risk |
Antibiotics < 48 hours in 1st week |
Antibiotics > 48 hours in 1st week |
P value |
| Birth weight |
1053 +/- 296 |
944 +/- 274 |
<0.01 |
| SNAP score |
13 +/- 9.2 |
17.8 +/-7.1 |
<0.01 |
| Clinical Chorio % |
5 |
18 |
<0.01 |
| Prolonged ROM |
14 |
26 |
<0.01 |
From the table I think we can agree that these infants were smaller and potentially sicker which likely motivated those clinicians to try and “do the right thing” even if cultures were negative. In this paper they defined sepsis as a positive culture and the presence of signs suggestive of sepsis, which avoids any confusion, related to such subjective classification as “possible or probable” sepsis where the clinical picture is suggestive but the culture negative. Despite a perceived increase in risk of sepsis after birth how accurate were clinicians? Early and Late Onset Sepsis Rates 14% in the < 48 hr and 16% in the > 48 hour group. Not significant at all.
The Cost of Fear
What is significant is the consequence of fear that motivates such decisions in the face of negative blood cultures. There is no difference in our ability to predict, yet doing so increases the risk of recovering bacteria from the endotracheal tube and more so resistant ones. The likelihood of obtaining bacterial growth in the endotracheal tube is more than doubled; NEC increased 2.5 times, gram-negative resistance tripled and the odds of developing BPD approximately doubled with an increasing tendency to this outcome simply by prolonging antibiotics. The cost of fear is that we trade our poor ability to truly predict sepsis with significant adverse risk that impacts the infant not only during their stay but long after they leave the NICU.
It is human nature to wish to do no harm. In order to truly achieve this we have to quell our need to “feel good” by knowing we have covered for sepsis and replace this with the fear of causing serious harm from such action. The decision to prolong the antibiotic course is the easy route as we go home comfortable that the baby is “covered” in case we are wrong. It makes us feel better but at significant cost. Only by changing our perspective of what constitutes harm will we ever move forward in this fight to change practice. Are you prepared to do it?

