
by All Things Neonatal | Jun 20, 2019 | resuscitation
This post has the potential to be polarizing as sustained inflations while common as an approach after delivery in Europe has not been widely adopted in Canada and the United States. Some time ago I wrote about sustained inflations and a reader commented that I should wait for the results of the The Sustained Aeration for Infant Lungs (SAIL) trial before forming a final opinion on whether this is a good strategy or not. The previous blog post on this topic was Is It Time To Use Sustained Lung Inflation in NRP? and was followed by Is expired CO2 the key to making sustained inflation a standard in resuscitation? The first post concluded that there was a concerning trend towards more IVH in those who received sustained inflations (SI) while the second showed both a reduction in BPD and duration of mechanical ventilation with this approach. I suggested that maybe we were really onto something here and then I was asked to wait before coming to a conclusion until the SAIL trial was done. Well that day has come.
The SAIL trial
This trial led by Dr. H. Kirpalani and involving 18 NICUs in 9 countries was a big endeavour. The paper was just published and is entitled Effect of Sustained Inflations vs Intermittent Positive Pressure Ventilation on Bronchopulmonary Dysplasia or Death Among Extremely Preterm Infants The SAIL Randomized Clinical Trial. The trial compared SI of 15 seconds at a peak pressure of 20 cmH2O, followed if needed by a second SI of 15 seconds
at a peak of 25 cmH2O to traditional PPV for infants who after initial 30 seconds of CPAP required further intervention to establish breathing. These were provided via facemask or nasopharyngeal tune attached to a t-piece resuscitator. In both groups after the initial intervention standard resuscitation steps were carried out. The primary outcome was death or BPD at 36 weeks PMA. A data safety monitoring board (DSMB) was formed as well and it is this group that became very important to the conclusions of the study and led to its early termination. All infants were 23 weeks 0 days’ to 26 weeks 6 days’ GA. Before the study was terminated the final totals were 215 patients in the SI arm and 211 in the traditional PPV group.
The trial was stopped after the DSMB identified an excessive number of early deaths within 48 hours in the SI group. The findings were “11 of 16 early deaths in the sustained inflation group vs 1 of 3 in the standard
resuscitation group were considered possibly related to allocation group”. A number of these deaths occurred in the highest risk group of those born at 23-24 weeks but it was enough to stop recruitment.
With respect to the primary outcome the results showed no difference between the two approaches. In saying this however, if the study did not recruit enough patients as planned to demonstrate a difference one has to question whether the study had enough power to find a benefit.

To answer this question the authors performed a Bayesian Analysis to determine the probability that adding more patients would have led to a different conclusion. That is to determine if they would have found a difference favouring SI. In the end they found that their conclusions would not have changed. Sustained inflations in infants from 23 weeks 0 days’ to 26 weeks 6 days’ GA do not confer a benefit and may be associated with a higher likelihood of death within 48 hours of birth.
What do we do with these results?
I think this is it. I can’t see a research ethics board allowing another study at this point. This by neonatal standards was a big study given the relative scarcity of infants at these gestational ages. The fact that no difference was found in rates of death or survival with BPD for those at highest risk of these outcomes suggests to me that looking at older GA at birth will not produce different results. Sustained inflation to establish FRC and initiate respiration was a good concept backed by animal research. Moreover, clinical work out of Edmonton in recent years suggested potential benefits but with the publication of this study I suspect we will need as a neonatal community to look at other strategies to decrease rates of BPD. Concerns over increased risk of death in my opinion mean this ship has SAILed,

by All Things Neonatal | Jun 5, 2019 | resuscitation
Just about all of our preterm infants born at <29 weeks start life out the same in terms of neurological injury. There are of course some infants who may have suffered ischemic injury in utero or an IVH but most are born with their story yet to be told. I think intuitively we have known for some time that the way we resuscitate matters. Establishing an FRC by inflating the lungs of these infants after delivery is a must but as the saying goes the devil is in the details.
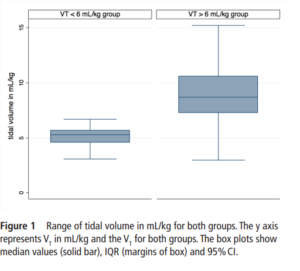
The Edmonton group led by Dr. Schmolzer has had several papers examined in these blogs and on this occasion I am reviewing an important paper that really is a follow-up study to a previous one looking at the impact of high tidal volume delivery after birth. I have written on this previous paper before in It’s possibile! Resuscitation with volume ventilation after delivery. On this occasion the authors have published the following paper; Impact of delivered tidal volume on the occurrence of intraventricular haemorrhage in preterm infants during positive pressure ventilation in the delivery room.This observational study had a simple enough premise. Will the use of Vt > 6 mL/kg in infants given PPV for at least two minutes lead to worse rates of IVH? All infants were < 29 weeks and if they had chest compressions or epinephrine were excluded. All infants were treated equally in terms of delayed cord clamping and antenatal steroid provision. Ventilation was done with a t-piece resuscitator and Vt measured with an NM3 monitor connected to the face mask. First ultrasounds were done for all at 3 days of age.
What did the authors find?
One hundred and sixty five infants comprised this cohort. Overall, 124 (75%) infants were in the high volume group compared to 41 (25%) with a mean VT<6 mL/kg. Median Vt were 5.3 (4.6-5.7) ml/kg for the low group and 8.7
(7.3-10.6) mL/kg which were significantly different.
 When looking at the rates of IVH and the severity of those affected the results are striking.
When looking at the rates of IVH and the severity of those affected the results are striking.
IVH in the high VT group was diagnosed in 63 (51%) infants compared with 5 (13%) infants in the normal VT group (P=0.008).Severe IVH (grade III or IV) developed in 33/124 (27%) infants in the high VT group and 2/41 (6%) in the normal VT group (P=0.01)
Hydrocephalus, following IVH developed in 7/49 (14%) and 2/16 (13%) in the >6 mL/kg and <6 mL/kg VT groups. Looking at other factors that could affect the outcome of interest the authors noted the following physiologic findings. Oxygen saturations were lower in the low volume group at 6, 13 and 14 min after birth while tissue oxygenation as measured by NIRS was similarly lower at 7,8 and 25 min after birth (P<0.001). Conversely, heart rate was significantly lower in the VT>6 mL/kg group at 5, 20 and 25 min after birth (P<0.001). Fraction of inspired oxygen was similar in both groups within the first 30 min. Systolic, diastolic and mean blood pressure was similar between the groups. What these results say to me is that despite having lower oxygen saturations and cerebral oxygen saturation at various time points in the first 25 minutes of life the infants seem to be better off given that HR was lower in those given higher volumes despite similar FiO2. Rates of volume support after admission were slightly higher in the high volume group but inotrope usage appears to be not significantly different. Prophylactic indomethacin was used equally in the two cohorts.
Thoughts for the future
Once a preterm infant is admitted to the NICU we start volume targeted ventilation from the start. In the delivery room we may think that we do the same by putting such infants on a volume guarantee mode after intubation but the period prior to that is generally done with a bag and mask. Whether you use a t-piece resuscitator or an anesthesia bag or even a self inflating bag, you are using a pressure and hoping not to overdistend the alveoli. What I think this study demonstrates similar to the previous work by this group is that there is another way. If we are so concerned about volutrauma in the NICU then why should we feel any differently about the first few minutes of life. Impairment of venous return from the head is likely to account for a higher risk of IVH and while a larger study may be wished for, the results here are fairly dramatic. Turning the question around, one could ask if there is harm in using a volume targeted strategy in the delivery room? I think we would be hard pressed to say that keeping the volumes under 6 mL/kg is a bad idea. The challenge as I see it now is whether we rig up devices to accomplish this or do the large medical equipment providers develop an all in one system to accomplish this? I think the time has come to do so and will be first in line to try it out if there is a possibility to do a trial.
