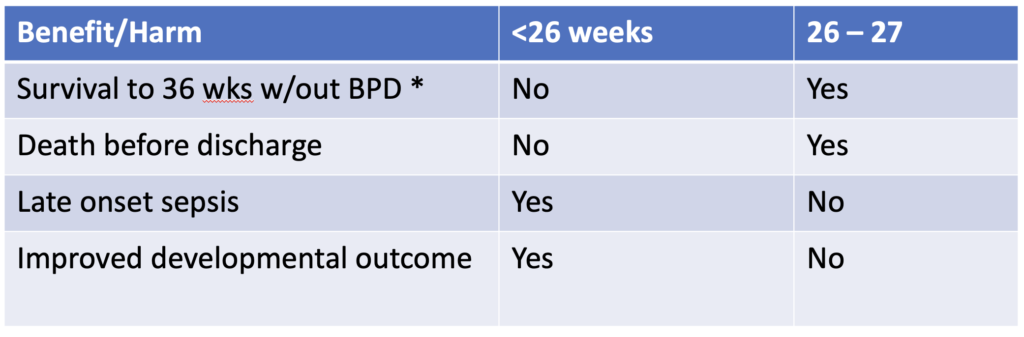
Precision medicine is a growing field in which genetic factors, environment, metabolism and even lifestyle are taken into account when deciding who should receive a treatment or not. When it comes to bronchopulmonary dysplasia I believe anyone who works in Neonatal care can attest it is a mystery why some infants go on to develop BPD while others don’t. We do know that certain treatment strategies may increase risk such as using excessive volumes or pressure to ventilate and in the last 25 years the notion that your level of cortisol in the blood may make a difference as well. I have written about prophylactic hydrocortisone use before in Hydrocortisone after birth may benefit the smallest preemies the most! When looking at the literature thus far and taking into account the results of the individual patient meta-analysis the following table can be generated highlighting a summary of benefits.
The question thus becomes if there is benefit for some infants under 26 weeks and then for some that are 26 and 27 weeks but there is also risk of harm, is there a way to select out those who are most likely to benefit with the least risk of harm.
A baby’s initial cortisol level may be the answer
The PREMILOC study was a double-blond multicentred trial of 523 infants randomly assigned to either prophylactic hydrocortisone in the first 24 hours of life or placebo. All infants were under 28 weeks at birth and received 1 mg/kg/d of hydrocortisone 1 mg/kg/d for 7 days followed by 3 days of 0.5 mg/kg/d for three days. In a pre-planned study coming out of the PREMILOC study, researchers looked at the role of baseline cortisol in predicting response to treatment or risk of adverse outcomes.
What they found in examining baseline levels for both treatment and placebo groups was that a relationship exists between the baseline level and such outcomes.
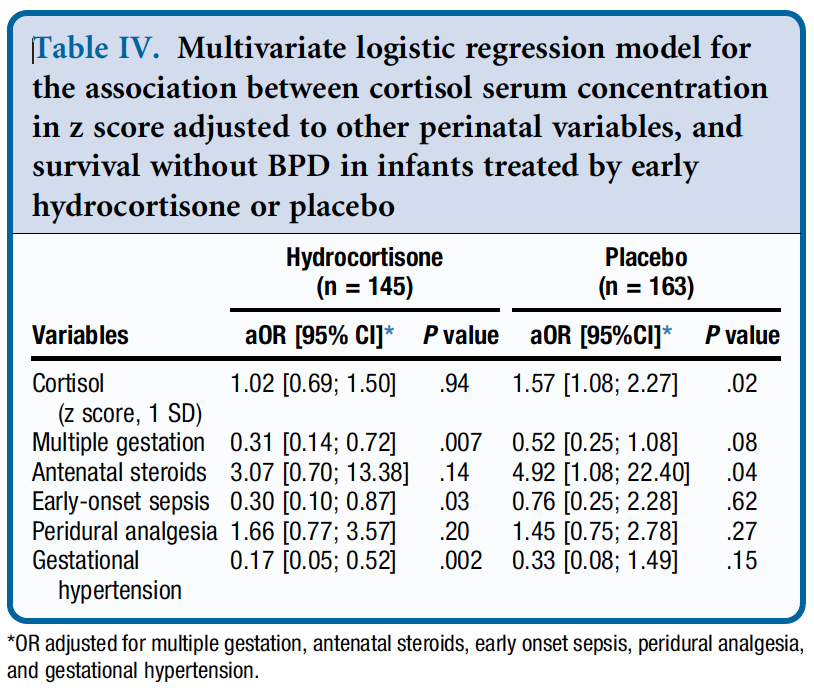
From Table 4 they found a relationship between survival without BPD and a higher initial level of cortisol but found no such relationship in the treatment arm. The threshold of what was considered high was 880 nmol/L although the mean cortisol was in the 400-500 nmol/L range. in other words, if having adequate physiologic levels of cortisol is the goal and a baby already has that, giving more non-antiinflammatory dosing of hydrocortisone doesn’t yield benefit.
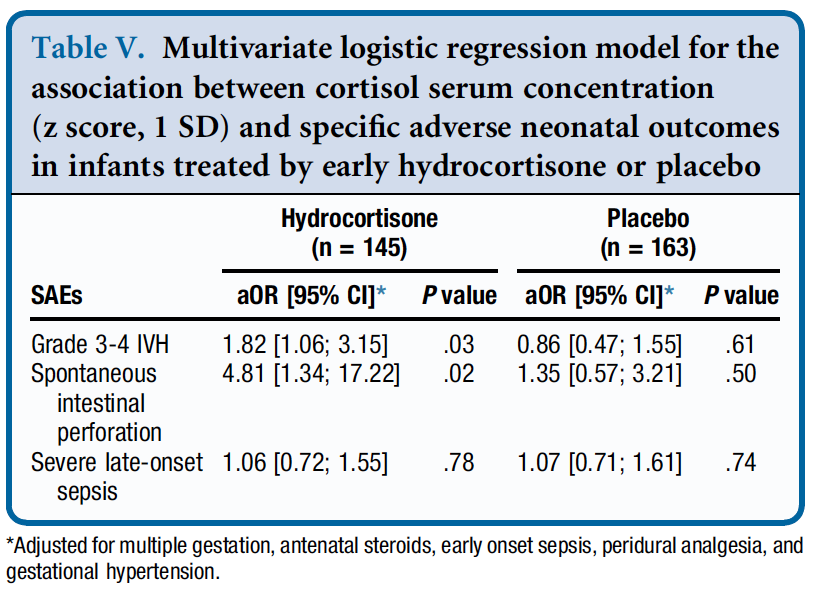
Similarly, when looking at side effects a positive correlation was found between higher baseline levels of cortisol and risk of grade III/IV IVH and spontaneous intestinal perforation. It would seem therefore that if a baby has the level of cortisol that they would normally have from a physiologic perspective they are no different than a placebo arm patient when given hydrocortisone as you bring them to where they need to be. When you double the dose however that they should have, side effects begin to rear their ugly head.
How can you use this information?
From personal conversations I know that many centres are struggling with what to do about giving hydrocortisone. On the one hand there isn’t much benefit (if at all) for BPD in the 24 and 25 week infants but they do better from a neurodevelopmental standpoint. On the other hand there is a benefit in the 26 and 27 week infants but you may predispose them to side effects as well.
This is where precision medicine comes in. One option for centers unsure of who to provide this to (if at all) could be to use a threshold of 880 nmol/L and if the initial level is above this you would not treat but if below offer treatment. This level while found in the study to be predictive of side effects in particular if high does seem very high to me. I would think most babies would qualify which is not necessarily a bad thing but in our center we have typically used levels above 400 or 500 as an adequate stress response. Regardless of the level picked one would be using physiologic data to determine who to give hydrocortisone to as a way to try and maximize benefit and minimize harm for the individual patient.
Make no mistake. Regardless of whether you decide to try this for your patients I don’t believe this is a magic bullet. The best chances for our patients come from having bundles of evidence based based practices and applying them to the patient population if we hope to reduce BPD and minimize risk from any side effects of our treatments. The question is whether prophylactic hydrocortisone should be part of this bundle.
Choosing to provide postnatal systemic steroids to preterm infants for treatment of evolving BPD has given many to pause before choosing to administer them. Ever since K Barrington published his systematic review The adverse neuro-developmental effects of postnatal steroids in the preterm infant: a systematic review of RCTs. and found a 186% increase in risk of CP among those who received these treatments, efforts have been made to minimize risk when these are given. Such efforts have included shortening the exposure from the length 42 day courses and also decreasing the cumulative dose of dexamethasone. Fortunately these efforts have led to findings that these two approaches have not been associated with adverse neurodevelopmental outcomes. Having said that, I doubt there is a Neonatologist that still doesn’t at least think about long term outcome when deciding to give dexamethasone. The systemic application certainly will have effects on the lung but the circulating steroid in the brain is what occupies our thoughts.
What About Applying it Directly to the Lung
If you wanted to prevent BPD the way to do it would be to minimize the time infants are exposed to positive pressure ventilation. Rather than giving steroids after a week or two maybe it would be best to give them early. Recent evidence supports this for systemic steroids and has been written about recently. Hydrocortisone after birth may benefit the smallest preemies the most! This still involves providing steroid systemically. Over the years, inhaled steroids have been tried as have intratracheal instillation of steroid with and without surfactant as a vehicle for distribution to the lung. This month colleagues of mine anchored by Dr. G. t’Jong (a founding member of the “Tall Men of Pediatrics #TMOP) published a systematic review and meta-analysis of all such RCTs in their paper Efficacy and safety of pulmonary application of corticosteroids in preterm infants with respiratory distress syndrome: a systematic review and metaanalysis. The results of the study suggest that there may well be a role for this approach.
All of the included studies used a prophylactic approach of giving between the first 4 hours and the 14th day of postnatal age doses of pulmonary steroids with the goal of preventing death or BPD. The GA of enrolled infants ranged from 26 to 34 weeks, and the birth weight ranged from 801 to 1591 g. Out of 870 possible articles only 12 made the cut and compromised the data for the analysis.
Routes of steroid were by inhalation, liquid instillation though the endotracheal tube or by mixing in surfactant and administering through the ETT.
What Did They Find?
Using 36 weeks corrected age as a time point for BPD or death, the forrest plot demonstrated the following. A reduction in risk of BPD or death of 15% with a range of 24% to only a 4% reduction.
Looking at the method of administration though is where I find things get particularly interesting.
What this demonstrates is that how you give the steroids matters. If you use the inhalational or intratracheal instillation (without a vehicle to distribute the steroids) there is no benefit in reduction of BPD or death. If however you use a vehicle (in both Yeh studies it was surfactant) you find a significant reduction in this outcome. In fact if you just look at the studies by Yeh the reduction is 36% (CI 34 – 47%). In terms of reduction of risk these are big numbers. So big one needs to question if the numbers are real in the long run.
Why might this work though?
In the larger study by Yeh, budesonide was mixed with surfactant and delivered to intubated infants every 8 hours until FiO2 was less than 30%, they were extubated or a maximum of 6 doses were reached. We know that surfactant spreads throughout the lung very nicely so it stands to reason that the budesonide could have been delivered evenly throughout the lung. Compare this with inhalational steroid that most likely winds up on the plastic tubing or proximal airway. The anti-inflammatory nature of steroids should decrease damage in the distal airways offsetting the effects of positive pressure ventilation.
Future Directions
I am excited by these findings (if you couldn’t tell). What we don’t know though is whether the belief that the steroid stays in the lung is true. Are we just making ourselves feel better by believing that the steroid won’t be absorbed and move systemically. This needs to be tested and I believe results of such testing will be along in the near future.
Secondly, we need a bigger study or at least another to add to the body of research being done. Such a study will also need long term follow-up to determine if this strategy does at least have equal neurodevelopmental outcomes to the children who don’t receive steroid. The meta-analysis above does show in a handful of studies that long term outcome was no different but given the history of steroids here I suspect we will need exceptionally strong evidence to see this practice go mainstream.
What I do believe is whether you choose to use steroids prophylactically using hydrocortisone or using intratracheal surfactant delivered budesonide, we will see one or both of these strategies eventually utilized in NICUs before long.
This must be one of my favourite topics as I have been following the story of early hydrocortisone to reduce BPD for quite some time. It becomes even more enticing when I have met the authors of the studies previously and can see how passionate they are about the possibilities. The PREMILOC study was covered on my site twice now, with the first post being A Shocking Change in Position. Postnatal steroids for ALL microprems? and the second reviewing the 22 month outcome afterwards /2017/05/07/early-hydrocortisone-short-term-gain-without-long-term-pain/.
The intervention here was that within 24 hours of birth babies born between 24-27 weeks gestational age were randomized to receive placebo or hydrocortisone 1 mg/kg/d divided q12h for one week followed by 0.5 mg/kg/d for three days. The primary outcome was rate of survival without BPD at 36 weeks PMA. The finding was a positive one with a 9% reduction in this outcome with the use of this strategy. Following these results were the two year follow-up which reported no evidence of harm but the planned analysis by gestational age groupings of 24-25 and 26-27 weeks was not reported at that time but it has just been released this month.
Is there a benefit?
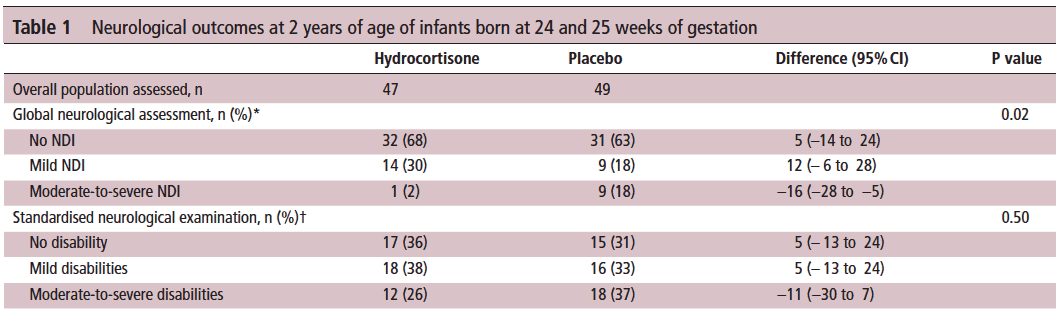
Of the original cohort the authors are to be commended here as they were able to follow-up 93% of all infants studied at a mean age of 22 months. The methods of assessing their neurological status have been discussed previously but essentially comprised standardized questionnaires for parents, assessment tools and physical examinations.
Let’s start off with what they didn’t find. There was no difference between those who received placebo vs hydrocortisone in the 26-27 week group but where it perhaps matters most there was. The infants born at 24-25 weeks are certainly some of our highest risk infants in the NICU. It is in this group that the use of hydrocortisone translated into a statistically significant reduction in the rate of neurodevelopmental impairment. The Global Neurological Assessement scores demonstrated a significant improvement in the hydrocortisone group with a p value of 0.02. Specifically moderate to severe disability was noted in 18% compared to 2% in the group receiving hydrocortisone.They did not find a difference in the neurological exam but that may reflect the lack of physical abnormalities with cognitive deficit remaining. It could also be explained perhaps by the physical examination not being sensitive enough to capture subtle differences.
Why might this be?
Adding an anti-inflammatory agent into the early phase of a preemies life might spare the brain from white matter damage. Inflammation is well known to inflict injury upon the developing brain and other organs (think BPD, ROP) so dampening these factors in the first ten days of life could bring about such results via a mechanism such as that. When you look at the original findings of the study though, a couple other factors also pop up that likely contribute to these findings as well. Infants in the hydrocortisone group had a statistical reduction in the rate of BPD and PDA ligations. Both of these outcomes have been independently linked to adverse neurodevelopmental outcome so it stands to reason that reducing each of these outcomes in the most vulnerable infants could have a benefit.
In fact when you add everything up, is there much reason not to try this approach? Ten days of hydrocortisone has now been shown to reduce BPD, decrease PDA ligations and importantly in the most vulnerable of our infants improve their developmental outcome. I think with this information at our fingertips it becomes increasingly difficult to ignore this approach. Do I think this will become adopted widely? I suspect there will be those who take the Cochrane approach to this and will ask for more well designed RCTs to be done in order to replicate these results or at least confirm a direction of effect which can then be studied as part of a systematic review. There will be those early adopters though who may well take this on. It will be interesting to see as these centres in turn report their before and after comparisons in the literature what the real world impact of this approach might be.
Stay tuned as I am sure this is not the last we will hear on this topic!


 (a founding member of the “Tall Men of Pediatrics #TMOP) published a systematic review and meta-analysis of all such RCTs in their paper
(a founding member of the “Tall Men of Pediatrics #TMOP) published a systematic review and meta-analysis of all such RCTs in their paper