In NICU we are always vigilant for infections. Bacterial sepsis is not uncommon and in fact in the latest 2020 Canadian Neonatal Network annual report, 9.4% of all babies across Canada born at < 33 weeks gestation experienced an infection after 3 days of age. Looking at the rate of infections in those with central lines (Central Line Bloodstream Infection or CLABSI the rate was 2.9/1000 line days. Infections in NICU are not surprising given that these infants often have need for vascular access and needle pokes breaking the skin and have a somewhat fragile immune system associated with premature birth. There are many strategies to reduce infection risk in the NICU but one in particular that has been around a long time is cleansing of the skin before any skin breaking procedures are performed such as for blood draws. Options exist for cleaning in terms of solution and whether it contains alcohol or not. A common skin antiseptic used is chlorhexidine which comes available as a 2% or 1% solution and with or without alcohol. The babies in particular who are our smallest may be sensitive to the alcohol and may be left with skin burns so for the smallest of infants we often clean without the alcohol containing solutions. What we are going to talk about today though is the use of 2% vs 1% and whether one is any different than the other in terms of effectiveness.
The Study
The study was done in India by Sharma A et al and entitled Aqueous chlorhexidine 1% versus 2% for neonatal skin antisepsis: a randomised non-inferiority trial. The authors set out to determine a number of things. The primary outcome was the percentage of negative skin swabs after application of both but they also looked for evidence of harm in terms of skin rashes and chlorhexidine blood levels. The strategy employed was for the investigator to identify a 4cm2 skin area to obtain the pre-antisepsis skin swab from one of the following sites: cubital fossa, dorsum hand or dorsum foot. Each patient could be enrolled again after a 96 hour period of time had elapsed. An alternate site was selected at the time of repeat enrolment. Each patient had a swab of this area done in a specific and repeated way in terms of strokes of the skin and then in a randomized fashion each patient received either the 1% or 2% solution on a swab. The solution was tested by a pharmacist throughout the study to validate the concentration of chlorhexidine (swab was dipped in the tested solution) and then applied in a consistent manner to the skin area. The area was left to dry for 60 seconds and then a second swab taken to determine whether the skin had been cleared of the bacteria that would have been picked up by the swab pre-chlorhexidine. The study set a target of a 5% non-inferiority limit comparing the two concentrations with an expected efficacy of about 90% for a 2% chlorhexidine solution to sterilize an area. This meant that if the efficacy of the 1% solution fell below a 5% difference it would be deemed to not be equivalent to the 2%.
What did they find?
First of all the groups were comparable in baseline characteristics. The babies enrolled in the study ranged from 26 0/7 to 42 6/7 weeks at delivery. As planned the groups; 341 to 1% and 344 to 2% were stratified for analysis into 26 0/7 to 27 6/7, 28 0/7 to 34 6/7 and 35 0/7 to 42 6/7 groups. The means GA and BW for each overall group however were 2018 vs 2029 and 34 vs 35 weeks for 1 and 2% groups.
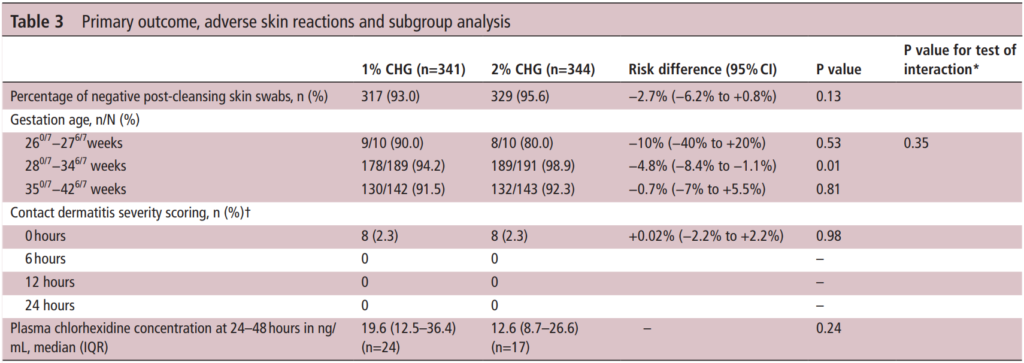
The table above has all the relevant information from the outcomes of interest. The efficacy of the antiseptics was a bit better than anticipated at 93% for the 1% vs 95.6% for the 2% group. On the surface you might be tempted to jump up and say “ah ha! They are equal”. However when you look at the 95% CI around the estimates you get a risk difference of -2.7% but the lower CI limit is -6.2% so as the authors concluded they are in fact not equal. Looking at the subgroups the number show some differences but only the middle group reached a statistical difference.
Importantly contact dermatitis which was scored by nursing using a standardized approach showed no difference at any time points. As expected some absorption did occur from application of the swabs but there was no difference between the two concentrations of significance although interestingly the higher concentration solution trended lower.
The authors do point out in this study that they did not get the 355 patients they wanted in each group although I have to say it was so close that I don’t believe adding a small percentage more of patients to the study would have been likely to change the conclusions.
Lesson from this study?
I suppose the first thing I take is that I am relieved that since our unit uses the 2% solution I don’t see any need for change. The second thing is that the rate of dermatitis from either solution is limited to about 1/10 babies after application but by 6 hours it is gone. Both have very high rates of successful skin antisepsis but if there is really no contraindication in terms of either skin irritation or high levels of drug in the blood my bias would be to grab onto the extra few percent successes at clearing the skin of bacteria. Even if it only a 3% gain, if we can maximize the cleaning of the skin before we poke a needle through it I think that is the way to go. If there are centres out there using the 1% though and plan on sticking to it I would be curious as to why?
If you work in the NICU then you have seen your fair share of septic workups for late onset sepsis. Sepsis is such a common diagnosis that if I had to guess I would say that at least 50% of all discharge summaries would include this in a list of final diagnoses for any VLBW infant. If you were to look through the chart though you would find that while workups are common, the recovery of a pathogenic bacterium is not as much. This is in part due to the low threshold that many people have for doing such workups. A little bit of temperature instability, a few more apneic events than normal or a rise in O2 requirements may all trigger such investigations. When they come back negative we all feel good that we looked but we also are then quick to blame the etiology on something else. Mild fluctuations in temperature are written off as overbundling, apnea due to outgrowth of caffeine and a rise in FiO2 to evolving CLD. Maybe though the explanation at least in some cases is that there was a pathogen but we didn’t test for it.
Viruses are everywhere
Tis the season so to speak so everyone is on high alert for viruses in our homes, schools, malls etc but many of us consider the NICU to be mostly free of such pathogens. The truth is we mostly are provided that we all wash our hands well, keep sick contacts from visiting and put on a mask when our coughing starts. Alas, if you have done a handwashing audit as we have you would know that when looking at technique and duration of handwashing, we don’t always hit 100%. These audits are for health care practitioners but I have often wondered what sort of results we would see were we to do the same for parents and visitors. When we know the viruses are out there such as during outbreaks of RSV and influenza we can’t help but send off our samples for respiratory viruses more frequently but what if we did this with intention for every late onset septic workup?
Lucky For Us Someone Did Just That!
Back in 2014 the following study was published. Viral respiratory tract infections in the neonatal intensive care unit: the VIRIoN-I study. This was a simple prospective and elegant study in which any infant in the NICU who had never been home and was greater than 72 hours had respiratory samples sent for viral panels within 72 hours of starting antibiotics for presumed late onset sepsis. The findings were certainly interesting in that 6% of 135 sepsis evaluations tested positive for a virus. In the analysis, the infants had the following characteristics:
tended to be older (41 vs 11 days; P = .007)
exposed to individuals with respiratory tract viral symptoms (37% vs 2%; P = .003)
lower total neutrophil counts (P = .02)
best predictor of viral infection was the caregivers’ clinical suspicion of viral infection (P = .006)
What interests me about these results are a couple things. The first is that as I was once told, the sensitivity of asking if someone has been around sick people is low during peaks in viral outbreaks as who hasn’t? Perhaps what this study tells us is that within the NICU environment we actually do a reasonable job of keeping such contacts away but when they slip through infections happen. The second point worth mentioning is that a low neutrophil count is associated which is interesting given how often neutropenia is pointed to as a reason to start antibiotics. These viruses are troublesome creatures indeed!
Further Evidence Arrives
At the end of last year a similar study was published by the same group Viral Respiratory Infections in Preterm Infants during and after Hospitalization. They took a different approach this time out and took nasopharyngeal samples from 189 infants in the NICU (96 term and 93 preterm) within 7 days of birth and then sent samples weekly while in hospital followed by monthly for four months after discharge. In this collection of infants a mere 4 patients tested positive in NICU and all of them under 28 weeks of age at birth! How do we account for the remarkable reduction in risk while in hospital? To answer that you can read through the NICU environment in the full article if you have access. In short, they had a very rigorous infection control set of precautions set up. Interestingly only one of the infections was with RSV and the unit did not provide prophylaxis for infants in hospital. Perhaps with precautions like theirs they felt it was unnecessary. Once discharged a little over a third of patients acquired a viral infection in the first four months at home. Given the potential risk for readmission and with that to a PICU this rate of viral infection is concerning.
Vision for the future!
Taken together we can state that viruses do make their way into the NICU but fortunately not as commonly as one might think. What the last study in particular does remind us though is that we need to ensure that as part of discharge teaching parents take home many of the practices that we have used in the hospital with respect to hand hygiene, limiting visitors and not being afraid to holster some hand sanitizer for those times when soap and water are not so easy to come by. To be sure viruses are out there but at least for the first few months after discharge for our most vulnerable babies a little paranoia about viruses could go a long way.
I came across an article from the BBC about a company in Israel that has developed a kit which can determine the presence of bacteria or virus in the blood of a patient within a two-hour window. More than that the kit has a point of care device as shown below.
Imagine for a moment the impact of being able to determine the presence or absence of sepsis within a two-hour window. Infants who have respiratory distress with a plan to assess in four-hours to determine need for antibiotics would never receive a dose. Other infants who were given one dose of ampicillin and gentamicin at birth would not need any further doses if the test indicated no bacteria or viruses present. Now you might say what is the harm in providing 48 hours of antibiotics or even 5 days if you are unsure of the presence of sepsis? There probably is little harm in a couple of days but the practice of prolonging antibiotics for fear that a patient has suspected sepsis is quite common in Neonatal circles. A recent article by Greenwood C et al (http://1.usa.gov/1Ex4qlH) examined stools at 1, 2 and 3 weeks of premature infants exposed to either short 1-4 day or longer 5-7 day courses of antibiotics. The results were quite striking in that the neonates exposed to the longer duration experienced less bacterial diversity than the other group and a preponderance of Enterobacter. Curiously levels of Lactobacillus and Bifidobacteria were low in all groups which might suggest a role for probiotics or explain why they might have been shown to reduce NEC. In fact in this study higher rates of NEC, sepsis and death were noted in the group receiving prolonged courses!
I have written other posts in which I have commented on Probiotics so to be clear I am not advocating that we use them routinely but one does have to wonder if it would be worthwhile repopulating the intestine of an infant who legitimately needed a 7 day course for a proven infection. Perhaps this post will stimulate someone to do that very study.
Aside from the perturbed microbiome leading to NEC, sepsis and death we also now have evidence of many long-term effects from antibiotics. The one creating the most alarm in press is no doubt the emergence of “superbugs” but more recently evidence has started to mount that repeated courses of antibiotics in infancy may lead to adult obesity (http://bit.ly/18JIIj7) and childhood allergy (http://bit.ly/1LwBmBc).
Getting back to this new technology it would still seem to be in the early stages. Looking through the company’s website they are allowing people to apply to be an early adopter. Additionally the links to their publications are really presentations at this time. A Pubmed search failed to come up with any specific articles regarding these products to I would have to say we are still in this products infancy. That being said it is certainly exciting to speculate about the impact that this innovation could have especially the point of care device pictured above which would bring the diagnosis to the bedside! I would encourage you to look at MeMeds website as it has a lot of very good information and if you check in from time to time who knows, you might be the first to hear that the two-hour test for sepsis is ready for use in your unit somewhere.



 . They took a different approach this time out and took nasopharyngeal samples from 189 infants in the NICU (96 term and 93 preterm) within 7 days of birth and then sent samples weekly while in hospital followed by monthly for four months after discharge. In this collection of infants a mere 4 patients tested positive in NICU and all of them under 28 weeks of age at birth! How do we account for the remarkable reduction in risk while in hospital? To answer that you can read through the NICU environment in the full article if you have access. In short, they had a very rigorous infection control set of precautions set up. Interestingly only one of the infections was with RSV and the unit did not provide prophylaxis for infants in hospital. Perhaps with precautions like theirs they felt it was unnecessary. Once discharged a little over a third of patients acquired a viral infection in the first four months at home. Given the potential risk for readmission and with that to a PICU this rate of viral infection is concerning.
. They took a different approach this time out and took nasopharyngeal samples from 189 infants in the NICU (96 term and 93 preterm) within 7 days of birth and then sent samples weekly while in hospital followed by monthly for four months after discharge. In this collection of infants a mere 4 patients tested positive in NICU and all of them under 28 weeks of age at birth! How do we account for the remarkable reduction in risk while in hospital? To answer that you can read through the NICU environment in the full article if you have access. In short, they had a very rigorous infection control set of precautions set up. Interestingly only one of the infections was with RSV and the unit did not provide prophylaxis for infants in hospital. Perhaps with precautions like theirs they felt it was unnecessary. Once discharged a little over a third of patients acquired a viral infection in the first four months at home. Given the potential risk for readmission and with that to a PICU this rate of viral infection is concerning.