I couldn’t think of a better topic for World Prematurity Day 2021 than what constitutes the edge of viability. Thinking back over my career, when I was a resident and fellow infants born at 25 and 26 weeks were deemed about as low as “we should” go but we certainly resuscitated infants at 24 weeks but this was considered heroic. Jump ahead to the last decade and we began caring for infants at birth at 23 weeks so commonly that the thought of offering comfort care only to infants at 24 weeks became almost unthinkable for many health care providers. Before I get jumped on, let me say that I am not saying I agree or disagree with that sentiment but it is something that is felt by many.
The Shared Decision Model
In the last few years a rethink again has occurred whereby the concept of the treating team knowing best has been replaced by the “shared decision model”. In this line of thinking, it is not up to us as health care providers to “tell the parents” what to do but rather come to a shared decision based on an assessment of the wishes and values of the parents in conjunction with hearing about both short and long term problems their infants may face if resuscitated. This concept was central to the statement by the Canadian Pediatric Society that I am proud to have been part of with respect to its development. The statement for those that are interested is Counselling and management for anticipated extremely preterm birth
What’s next? Going below 22 weeks?
The challenge of the shared decision model is that there comes a point where the answer is simply “no”. If for example a family at 19 weeks gestation demanded an attempt at resuscitation I would have to inform them that survival is not possible (assuming ultrasound confirmed anthropometric measurements consistent with that age). The question though becomes a little more difficult to answer at 21 weeks and was the subject of a recent article in the New York Times about a survivor at 21 weeks gestation.
Even with the best gestational age dating the estimate can be off by up to 5 days so it’s possible that the infant in this story was closer to 22 weeks or even midpoint between 22 and 23 weeks in reality. Regardless it does raise the question about what to do at 21 weeks and I suspect we will begin to see more stories about this now that the glass ceiling of 22 weeks has been breached. What about below 21 weeks? Sounds impossible I know but with research that remains at the stage of animal studies this may become possible. Maybe not in the next 5-10 years but it could happen in my lifetime in this chosen field.
The Artificial Placenta
This made headlines a few years ago with the news that the Children’s Hospital of Philadelphia had successfully kept a lamb alive for a period of 4 weeks using an artificial placenta and amniotic fluid.
You might think that this was a one-off experiment that will never see the light of day but similar work is being done in Toronto, Canada where they have been able to do similar work with preterm piglets in their paper Achieving sustained extrauterine life: Challenges of an artificial placenta in fetal pigs as a model of the preterm human fetus. Incidentally as my colleague Dr. Ayman Sheta worked on this project while in Toronto I am particularly pleased to share this research. Similar to the experience in CHOP the team in Toronto has been able to keep piglets alive for progressively longer durations. My understanding is that despite the best efforts infectious complications over arise limiting how long one can sustain such animals.
This leads me to my final thoughts on where we might be able to go. I see a future where we apply such technology to humans but not in the way that people might have thought. Keeping a fetus after delivery at 21 or 20 weeks on an artificial placenta for many weeks is not likely a realistic goal. What if we could get 1 or 2 weeks though and allow the fetus to be oxygenated without using positive pressure on their developing lungs and transition them at 23 or 24 weeks gestation? We may in this way be able to allow for postnatal maturation in a artificial uterine environment and give babies a chance who would otherwise never had the opportunity for a shared decision with medical staff.
Sound like science fiction? Well the beauty of the internet as my friend told me today is that once it’s out there it out there for good. Let’s see how this post stands the test of time and to all the babies out there in NICUs and to their families I wish you all a good and uneventful World Prematurity Day wherever you may be!
In NICU we are always vigilant for infections. Bacterial sepsis is not uncommon and in fact in the latest 2020 Canadian Neonatal Network annual report, 9.4% of all babies across Canada born at < 33 weeks gestation experienced an infection after 3 days of age. Looking at the rate of infections in those with central lines (Central Line Bloodstream Infection or CLABSI the rate was 2.9/1000 line days. Infections in NICU are not surprising given that these infants often have need for vascular access and needle pokes breaking the skin and have a somewhat fragile immune system associated with premature birth. There are many strategies to reduce infection risk in the NICU but one in particular that has been around a long time is cleansing of the skin before any skin breaking procedures are performed such as for blood draws. Options exist for cleaning in terms of solution and whether it contains alcohol or not. A common skin antiseptic used is chlorhexidine which comes available as a 2% or 1% solution and with or without alcohol. The babies in particular who are our smallest may be sensitive to the alcohol and may be left with skin burns so for the smallest of infants we often clean without the alcohol containing solutions. What we are going to talk about today though is the use of 2% vs 1% and whether one is any different than the other in terms of effectiveness.
The Study
The study was done in India by Sharma A et al and entitled Aqueous chlorhexidine 1% versus 2% for neonatal skin antisepsis: a randomised non-inferiority trial. The authors set out to determine a number of things. The primary outcome was the percentage of negative skin swabs after application of both but they also looked for evidence of harm in terms of skin rashes and chlorhexidine blood levels. The strategy employed was for the investigator to identify a 4cm2 skin area to obtain the pre-antisepsis skin swab from one of the following sites: cubital fossa, dorsum hand or dorsum foot. Each patient could be enrolled again after a 96 hour period of time had elapsed. An alternate site was selected at the time of repeat enrolment. Each patient had a swab of this area done in a specific and repeated way in terms of strokes of the skin and then in a randomized fashion each patient received either the 1% or 2% solution on a swab. The solution was tested by a pharmacist throughout the study to validate the concentration of chlorhexidine (swab was dipped in the tested solution) and then applied in a consistent manner to the skin area. The area was left to dry for 60 seconds and then a second swab taken to determine whether the skin had been cleared of the bacteria that would have been picked up by the swab pre-chlorhexidine. The study set a target of a 5% non-inferiority limit comparing the two concentrations with an expected efficacy of about 90% for a 2% chlorhexidine solution to sterilize an area. This meant that if the efficacy of the 1% solution fell below a 5% difference it would be deemed to not be equivalent to the 2%.
What did they find?
First of all the groups were comparable in baseline characteristics. The babies enrolled in the study ranged from 26 0/7 to 42 6/7 weeks at delivery. As planned the groups; 341 to 1% and 344 to 2% were stratified for analysis into 26 0/7 to 27 6/7, 28 0/7 to 34 6/7 and 35 0/7 to 42 6/7 groups. The means GA and BW for each overall group however were 2018 vs 2029 and 34 vs 35 weeks for 1 and 2% groups.
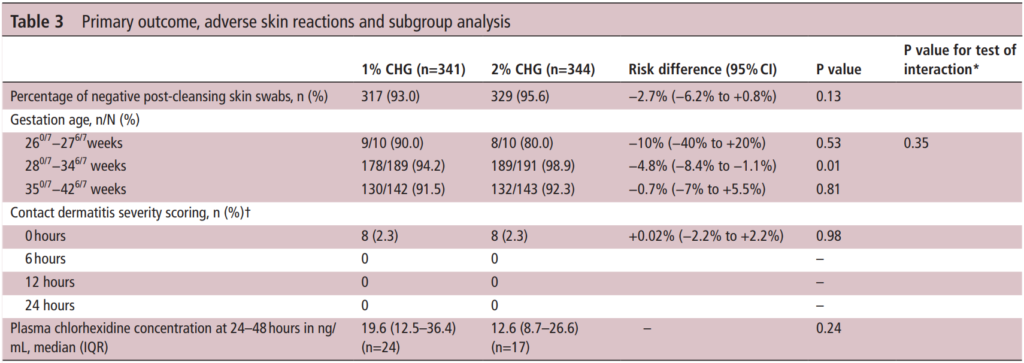
The table above has all the relevant information from the outcomes of interest. The efficacy of the antiseptics was a bit better than anticipated at 93% for the 1% vs 95.6% for the 2% group. On the surface you might be tempted to jump up and say “ah ha! They are equal”. However when you look at the 95% CI around the estimates you get a risk difference of -2.7% but the lower CI limit is -6.2% so as the authors concluded they are in fact not equal. Looking at the subgroups the number show some differences but only the middle group reached a statistical difference.
Importantly contact dermatitis which was scored by nursing using a standardized approach showed no difference at any time points. As expected some absorption did occur from application of the swabs but there was no difference between the two concentrations of significance although interestingly the higher concentration solution trended lower.
The authors do point out in this study that they did not get the 355 patients they wanted in each group although I have to say it was so close that I don’t believe adding a small percentage more of patients to the study would have been likely to change the conclusions.
Lesson from this study?
I suppose the first thing I take is that I am relieved that since our unit uses the 2% solution I don’t see any need for change. The second thing is that the rate of dermatitis from either solution is limited to about 1/10 babies after application but by 6 hours it is gone. Both have very high rates of successful skin antisepsis but if there is really no contraindication in terms of either skin irritation or high levels of drug in the blood my bias would be to grab onto the extra few percent successes at clearing the skin of bacteria. Even if it only a 3% gain, if we can maximize the cleaning of the skin before we poke a needle through it I think that is the way to go. If there are centres out there using the 1% though and plan on sticking to it I would be curious as to why?
I spend a bit of time on social media and when I do I come across the argument that vaccines aren’t needed in pregnancy if you have already had COVID. The concept from the vaccine hesitant is based on the notion of trying to avoid any perceived risk of vaccination when the body is already making antibodies against the virus. The literature has been fairly scant on newborns in terms of protective antibodies and limited to case reports/series that I have shared from time to time on either twitter or facebook. As you might expect something might have changed as I am writing a piece on this topic again. The change is related to a recent paper entitled Titers of SARS CoV-2 antibodies in cord blood of neonates whose mothers contracted SARS CoV-2 (COVID-19) during pregnancy and in those whose mothers were vaccinated with mRNA to SARS CoV-2 during pregnancy by Kashani-Legumsky et al in J Perinatol.
Setting The Stage
Before getting in to what they did it is important to understand how the mRNA vaccines work as the antibodies that one can look at in mothers and babies are of two types. The mRNA vaccines instruct the body to make anti-bodies against the spike protein (S antibodies) which forms the basis of how the vaccine helps our bodies identify the virus and then destroy it. For those who have actually been exposed to the virus and are not vaccinated, they develop a second antibody to the nucelocapsid protein (N antibody) which is within the viral core so this type will only be present in people who have been infected with the virus and their immune systems have dealt with it on their own. This is an important distinction as it allows you to create pure samples of people who have had the virus as a true infection and those who have been vaccinated and finally those who are neither.
Comparing Three Groups
So the authors here decided to compare three groups of women. Eighty three cord blood samples were divided into three groups (from the paper quoted) based on IgG antibody titres.
Group 1 included 29 samples (37%) from women who were infected with SARS-CoV-2 during pregnancy. Twelve had RT-PCR confirmed Covid-19 infection: three were infected in the first trimester, three in the second trimester and six in the third trimester. The other 17 had no clinical signs of SARS-CoV-2 infection during pregnancy and had a positive serologic test on admission. None of the 17 women had active SARS-CoV-2 infection at the time of delivery. Group 2 included 29 samples (37%) from women who were vaccinated against SARS-CoV-2 in the 3rd trimester.
Group 3 included 21 women (34%) and served as controls.
Looking at antibody levels in Group 1&2, 100% were positive for S antibodies. Interestingly, in group 1, 4 women did not test positive for the N antibody (3 were asymptomatic and one infected in the 1st trimester). In group 3 none of the women tested positive for any antibodies confirming they were neither vaccinated or had the infection previously.
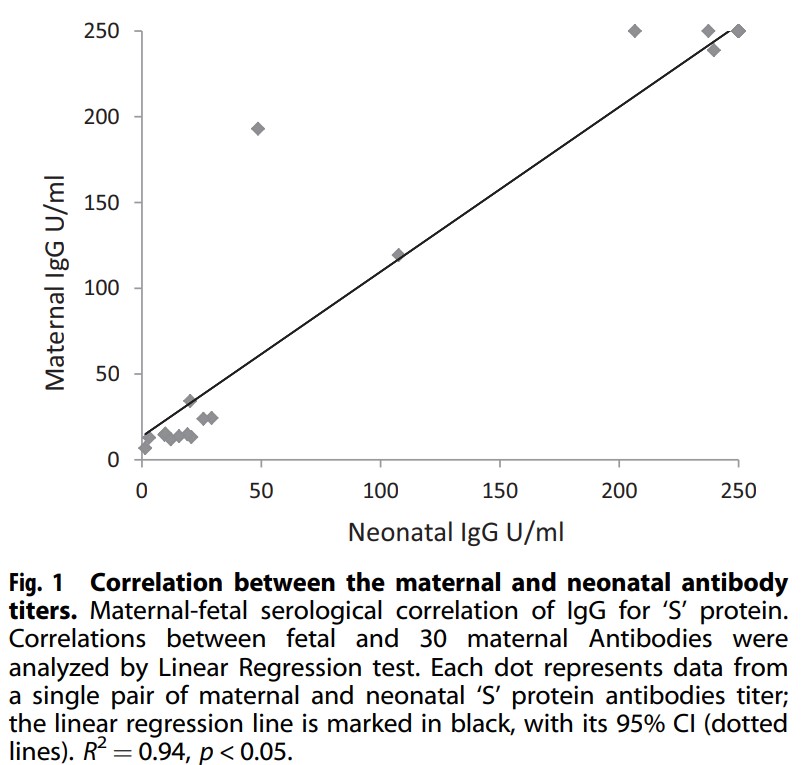
Looking at mean antibody S titres there was a significant difference found in that Group 1 had a mean of 83.7 U/mL vs 225.5 U/mL for the newborns whose mothers were vaccinated. Also notable was the relationship (not surprisingly between antibody levels in the mother at the time of delivery and newborn cord blood titres.
There was a linear correlation between the level in the mother and the level found in the newborn with higher levels presumably better for protecting the infant. Having said that, no infants in this study had neonatal COVID infection. Detractors would be quick to point out that this indicates it doesn’t matter if you get the vaccine since all babies were ok but remember although this may be the biggest study looking at antibodies in cord blood it remains a very small sample and neonatal infection although reported, remains a very rare occurrence.
The Other Side
If you have followed my coverage of the COVID saga from the start you would know that I am in favour of vaccination and in pregnancy as well. The results of this study are encouraging but we need to compare apples to apples. This study compared women who were vaccinated in the 3rd trimester to women who were infected at earlier time points and may have been sick or asymptomatic. The lower antibody levels found in group 1 could represent declining titres as the infection becomes more remote. What we also don’t know is what they antibody levels would have looked like in group 2 if the mothers were vaccinated in the 1st or 2nd trimester as this is now happening. Would the levels be similar? They just might be as the antibody levels do decline with time. We rely on memory cells to reactivate our antibody producing cells if the virus comes along again.
I am not saying this study is meaningless but be prepared if you quote this study for vaccine hesitant to point out that you are comparing recent vaccination to potentially mild cases or remote infections. What is clear and hopeful though is that your newborn is protected by antibodies you make in pregnancy from vaccination at very good levels and until we can vaccinate babies this is the greatest protection we can offer.
When I began my career in Neonatology we initially ventilated primarily with pressure limited time cycled modes of ventilation and only supported some of the breaths as in SIMV modes. With time and emerging research a movement to using set volumes came about and in many centres supporting every breath using an assist control mode or similar version. Although I don’t have access to it in my centre, ventilators such as the Avea also allow for automated FiO2 control in addition to having a choice of two different volume targeting modes. The difference between the modes is the subject of a study entitled Comparison of volume guarantee and volume-controlled ventilation both using closed loop inspired oxygen in preterm infants: a randomised crossover study (CLIO-VG study). I suppose it shouldn’t be a big surprise that as technology advances and we fine tune practice, different modes for volume targeting would arise.
What’s the difference?
Volume Controlled Ventilation (VCV) – flow based on a set volume and measurement of the PIP every 2 ms. Next breath is given the greater of PEEP+2 cm H2O or PIP-2 cmH2O. The ventilator at the end of each breath is able to determine if the baby is still demanding flow and continues providing flow but stops when inspiratory flow is <25% of peak set flow. There is constant inspiratory flow and peak volumes.
Volume Guarantee (VG)- inspiratory pressure is adjusted breath to breath. These breaths have a decelerating flow instead of a fixed flow as in VCV.
The Study
Using automated FiO2 control for both groups the study design was a crossover one. The concept was that better ventilation would help to keep O2 saturations more reliably in a target range of 90-95% and that one of these modes might be superior than the other in doing so. Infants in the study were born at 23+0 – 36+6 weeks and had to be intubated and on >21% FiO2 to be part of the study. Each group spent 12 hours in each arm with the starting mode randomly chosen before switching over to the other mode.
Based on a power calculation in which the authors selected looking for a 5% difference they determined they needed 19 patients in the study overall. The median GA of the infants was 25 weeks (IQR 24-28) with a BW of 685g.
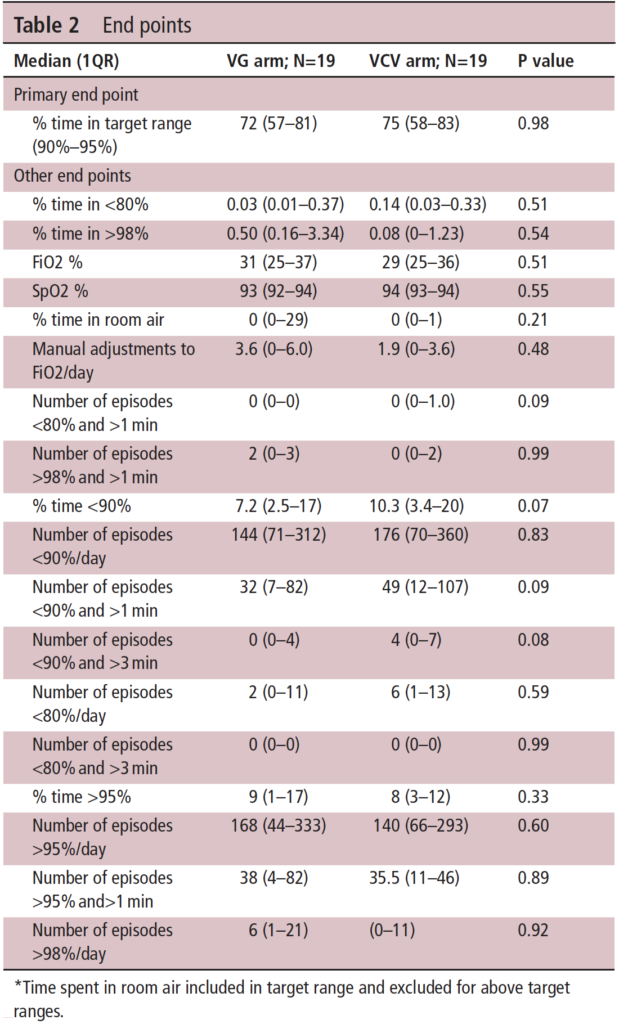
The results demonstrate at the top of Table 2 that the primary outcome was no different at all. Basically whichever mode you choose will work just fine when used with automated FiO2 control to keep the saturations in the target range. If there is anything that the study suggests though is that the percentage of time below 90% may be worse with VCV than VG. You get this from looking at the table and looking at the secondary outcomes. A word of warning though that since the study is small (very small) it is really difficult to take too much stock in the secondary outcomes as the study wasn’t powered to detect such differences. One can’t help but wonder though if that trend might have become a one of significance if the numbers in the study were greater. Is there biological plausibility for this? Looking at the two modes, it would appear that VG by adjusting each breath based on the last expired tidal volume may be more agile. If you believe the hypothesis that tighter control of alveolar ventilation by delivering better ventilation is key to reducing time outside the target ranges then it makes some sense that this mode would be better.
On a personal note, I use only VG in my centre so I am pleased to see there is really no difference in the primary outcome but the trend in the secondary outcomes at least puts a slight smile on my face as well!
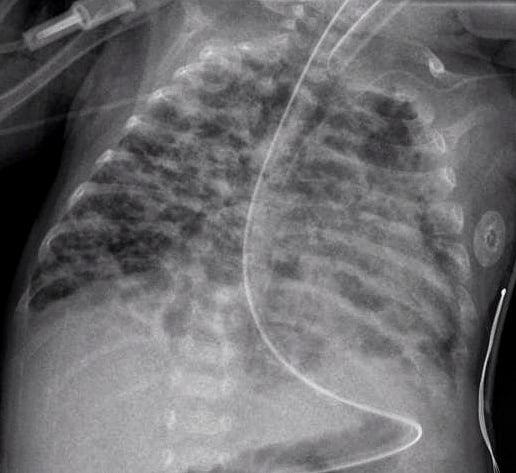
I have written a lot over the years on the topic of BPD. It isn’t by chance as it is a condition that Neonatologists have put a lot of weight on. In many ways it is a benchmark that is often the go to condition when comparing one unit to another. When two Neonatologists get together their first question isn’t what’s your rate of ROP or severe developmental delay but more often comparing rates of BPD. We like to compare this as a metric as it’s something we can see as compared to say rates of late onset sepsis. You can see a patient on a ventilator or on CPAP at 36 weeks but you can’t see bacteria coursing through veins.
Not all BPD is the same though. in 2000 the NIH produced a new consensus definition of BPD as shown below.
What stands out for the babies <32 weeks is how severe BPD is defined. Babies who are ventilated are classified in the same severity group as those who are on CPAP. Somehow that doesn’t seem quite right intuitively but alas that is what they decided at the time.
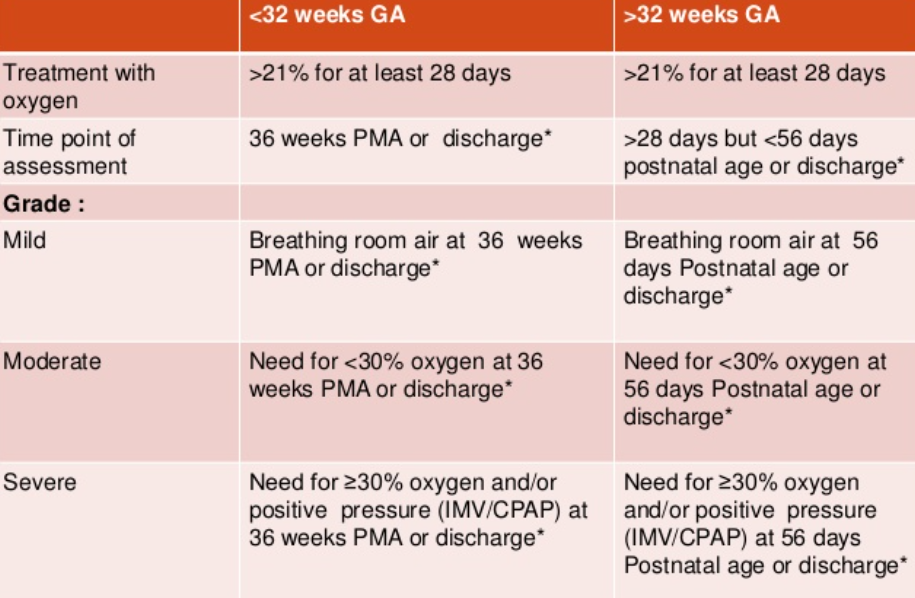
Type 1 sBPD: patients on nasal cannula or noninvasive positive pressure support (i.e., high flow nasal cannula (HFNC), nasal continuous positive airway pressure (nCPAP), noninvasive intermittent positive pressure ventilation (nIPPV)) Type 2 sBPD: infants receiving iMV
The authors then looked at a sample of 564 patients from 2015-2019 in the BPD collaborative registry and subdivided them into 429 (76%) Type 1 vs 135 (24%) Type 2 sBPD and compared outcomes between the two. The differences between the two types of BPD are quite significant and shown in Table I. Babies who went on to develop sBPD as Type 2 were younger and smaller than those with Type 1. Medication use within the NICU and after discharge was markedly different as were the total ventilator days which is likely not surprising since by definition they were still intubated at 36 weeks. Importantly if you were still intubated at 36 weeks PMA almost one quarter of the patients went on to receive a tracheostomy.
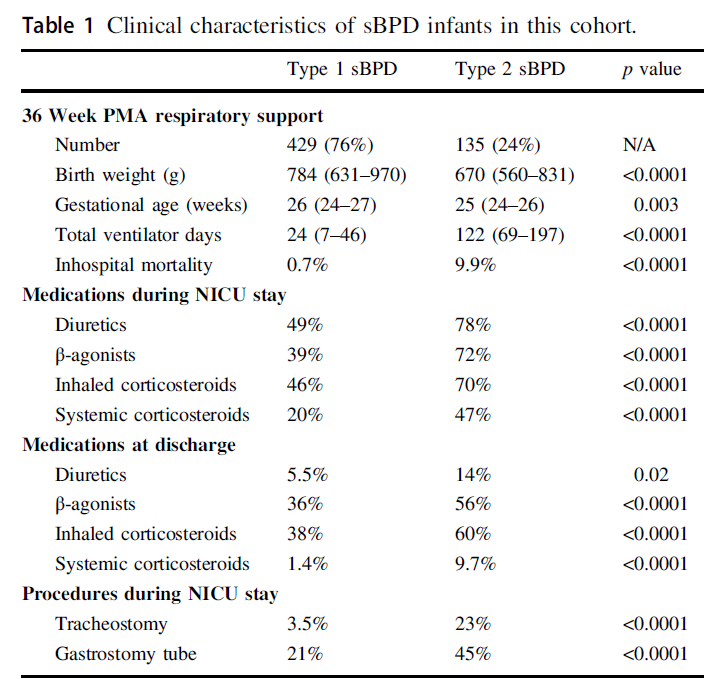
Looking at it another way using relative risks the signifance of having Type 2 sBPD is impactful.
Taking Meaning From This
You might be quick to say, Michael this is absolutely no surprise. On the other hand if you have read this blog for some time you may remember this piece The New BPD That Matters. This study looked at what gestational age really mattered when looking at long term pulmonary outcomes in a Canadian cohort. When you take all comers it was 40 weeks and not 36 weeks that really mattered. The likely differernce here though is that by selecting out only the severe patients in this current study it is indeed the 36 week mark that still has relevance. I actually think the two papers together are not contradictory but rather additive.
What I think one takes away from the current study is that failure to extubate by 36 weeks does in fact carry with it significant long term risk to the patient. It would be easy enough to say that these babies should be extubated but as you see from table I it isn’t that they didn’t try. From a medication standpoint it would appear that they ” threw the kitchen sink” at these babies. The only thing I find a little surprising is that only 47% of babies in the collaborative with type 2 sBPD received systemic steroids. If they were that sick I would have expected it to be higher although that also may just be a reflection of my own practice.
One thing that I think will be a hot topic moving forward is the use of higher levels of CPAP than what many units are accustomed to. This has also been recently discussed in High CPAP vs NIPPV. Is there a winner? There may be a reluctance by some units to use CPAP levels in the +9-12 cm H2O range but when looking at these downstream complications for patients who remain ventilated at 36 weeks I think people need to seriously consider their biases and whether they are based on science or what they were taught. I can’t help but think of the oft used expression absence of evidence is not evidence of absence and think that if we can all be a little humble who knows what we may discover that can help this population.