by All Things Neonatal | Jun 12, 2015 | Neonatology, nutrition
The picture looks ridiculous. Why does this seem so unnatural yet we feed babies this same product around the world. Granted they don’t drink it from the source as this man is but the liquid is in essence the same. As the saying goes, “Cow’s milk is for baby cows”. When you put it that way it helps put in context the question posed as the title of this post. Should we be surprised that the consumption of a milk meant for another species might have some side effects at a population level if fed to enough infants; especially those with fragile bowel due to prematurity or other high risk condition compromising blood flow to the gut.
The following piece was written by Kari Bonnar with contributions from Sharla Fast both Registered Dieticians in our NICUs. It has been recognized for some time now that the use of donor milk in our highest risk premature infants is associated with less NEC and based on a previous review of the evidence we have been using DBM for the past several years. What this post explores though is the potential for further benefit by taking the next step. That is to ask the question; what additional benefit may be gained by replacing all sources of Cow’s Milk protein in this population. I am delighted to present their review of the literature here as I am sure you will find it as informative and thought provoking as I have.
The health benefits of human milk for all infants, including those born extremely premature, have been increasingly recognized and published.1 The American Academy of Pediatrics policy statement on breastfeeding and the use of human milk recommends that all preterm infants receive human milk including donor human milk if mother’s own milk is unavailable.2 When compared with a diet of preterm formula, premature infants have improved feeding tolerance and a lower incidence of late onset sepsis and necrotizing enterocolitis (NEC) when fed their mothers’ own milk.3 For mothers of extremely premature infants, providing sufficient milk to meet their infant’s needs is a common challenge. Pasteurized donor human milk has been made available to this population in WRHA since 2011 as it has been found to be well tolerated and is also associated with a significantly lower incidence of NEC.4
However, as the sole nutritive substance, human milk does not meet the macronutrient and micronutrient requirements of preterm infants. Multi-nutrient fortifiers are required to provide additional protein, minerals and vitamins to ensure optimal nutrient intake and neurodevelopmental growth.5 Prolacta Bioscience has recently launched in Canada with their human milk-based fortifiers, which are gaining popularity due to the ongoing research and success with these products in the United States, Austria, and now Canada.6 It is a new and novel approach that is proving to be most beneficial in reducing neonatal morbidity and mortality rates.7
In infants fed an exclusive human milk diet, Sullivan et al. found a reduction in medical NEC of 50% and surgical NEC of almost 90% compared to a diet containing cow’s milk-based products.7 To date, there is no other intervention that has had such a marked effect on the incidence of NEC.8 Abrams et al. found that for every 10% increase in intake of anything other than an exclusive human milk diet, the risk of NEC increases by 11.8% and the risk of surgical NEC increases by 21%, both with a 95% confidence interval.9
Patel et al. found that for every dose increase of 10ml/kg/day of human milk over the first 28 days post birth, the odds of sepsis decreased by 19%.10 Further to this, they found that overall NICU costs were lowest in very low birth weight (VLBW) infants who received the highest daily dose of human milk. Similarly, Abrams et al. reported that for each 10% increase in the intake of other than exclusive human milk diet, there was an 18% increase in risk for sepsis.9 In addition to predisposing the infant to other morbidities in the preterm population, and subsequent neurodevelopmental disability, sepsis significantly increases NICU costs by 31%. This translates into higher societal and educational costs for VLBW infants who survive sepsis with neurodevelopmental disability.10 ,11
A reduction in the number of days on total parenteral nutrition (TPN) was found by Cristofalo at al. with the use of an exclusive human milk based diet, in addition to reduction in sepsis and NEC.12 These same findings have been documented by Ghandehari et al. which reflect that an exclusive human milk diet leads to improved feeding tolerance and therefore, a decrease in total TPN days.13 Given that TPN is often the cause of late onset sepsis, the reduction of TPN days is imperative and almost always translates into decreased length of stay.14 Abrams et al. found that duration of TPN was 8 days less in infants receiving a diet containing <10% cow’s milk-based protein versus ≥ 10%, another recognizable dose related finding.9
It is well documented that increased growth leads to a decreased incidence of cerebral palsy and poor neurodevelopmental scores at 18-22 months corrected age, therefore adequate growth (weight, head circumference and length) is crucial in this population.15 The study by Hair et al. followed a standardized feeding protocol with early and rapid advancement of fortification with donor human milk derived fortifier and found that growth standards were being met and resulted in a marked decrease in extrauterine growth restriction.14 Cristofalo et al. study also compared growth rates, which were found to be slightly slower in the human milk fortified versus cow’s milk fortified arm of this study. However, it was mentioned that the small differences could be prevented with further adjustments in fortifier to improve rates of growth, as shown by Hair et al.12, 14 Abrams et al. confirms in their findings that growth rates were similar among human milk-based and cow’s milk-based fortification.9 This is a popular area of ongoing research with many abstracts also showing adequate growth rates with use of human milk-based fortifiers.
In closing, the review of current evidence clearly indicates that a diet of exclusive human milk is associated with lower mortality and morbidity in extremely premature infants without compromising growth and should be considered as an approach to nutritional care for these infants. Further research is needed to fully capture the extent to which using exclusive human milk diets actually reduce overall healthcare costs via improving the short and long term outcomes of extremely premature infants. Research to date only explores the financial impact for the first few years of life; therefore the true costs of these major morbidities are vastly underestimated and underreported. There are many unpublished trials and abstracts that are currently in process that will only strengthen the shift toward exclusive human milk-based diets, ideally making this common practice among Canadian centres in the very near future.
1 American Academy of Pediatrics. Section on Breastfeeding. Breastfeeding and the use of human milk. Pediatrics 2005; 115:496-506
2 American Academy of Pediatrics. Section on Breastfeeding. Breastfeeding and the use of human milk. Pediatrics 2012; 129:3;e827-41
3 Schanler RJ, Shulman RJ, Lau C. Feeding strategies for premature infants: Beneficial outcomes of feeding fortified human milk vs preterm formula. Pediatrics 1999;103:1150-7
4 Boyd CA, Quigley MA, Brocklehurst P, Donor Breast milk versus infant formula for preterm infants: a systematic review and meta-analysis. Arch Dis Child Fetal Neonatal Ed 2007;92:F169-75
5 Agostini C et al. Enteral nutrition supply for preterm infants: commentary from the European society for pediatric gastroenterology, hepatology, and nutrition committee on nutrition. JPGN 2010;50:1:85-91
6 Prolacta Bioscience, Industry, California: product description. http://www.prolacta.com/human-milk-fortifier
7 Sillivan S, et al. An Exclusively Human Milk-Based Diet is Associated with a Lower Rate of necrotizing Enterocolitis than a Diet of Human Milk and Bovine Milk-Based Products. J Pediatr 2010:156;562-7
8 Bell EF. Preventing necrotizing enterocolitis: what works and how safe? Pediatrics 2005:115;173-4
9 Abrams SA, Schanler RJ, Lee ML, Rechtman DJ. Greater Mortality and Morbidity in Extremely Preterm Infants fed a diet containing cow milk protein products. Breastfeed Med. 2014:9;1-8
10 Patel AL, Johnson TJ, Engstrom JL, Fogg LF, Jegier BJ et al. Impact of early human milk on sepsis and health-care costs in very low birth weight infants. J Perinatology 2013:33:514-19
11 Ganapathy V, Hay JW, Kim JH. Cost of necrotizing enterocolitis and cost-effectiveness of exclusively human milk-based products in feeding extremely premature infants. Breastfeed Med. 2012:7;29-37
12 Cristofalo EA, Schanler RJ, Blanco CL, Sullivan S, Trawoeger R, et al. Randomized trial of exclusive human milk versus preterm formula diets in extremely premature infants. J Pediatr. 2013;1-4
13 Ghandehari H, Lee ML, Rechtman DJ. An exclusive human milk based diet in extremely premature infants reduces the probability of remaining on total parenteral nutrition: a reanalysis of the data. BMC. 2012:5;188
14 Hair AB, Hawthorne KM, Chetta KE, Abrams, SA. Human milk feeding supports adequate growth in infants ≤1250 grams birth weight. BMC. 2013:6;459
15 Ehrankranz RA, Dusiuk AM, Vohr BR, Wright LL, Wrage LA, et al. Growth in the neonatal intensive care unit influences neurodevelopmental and growth outcomes of extremely low birth weight infants. Pediatrics. 2006.117:4; 1253-61
by All Things Neonatal | Jun 6, 2015 | Breastfeeding, Breastmilk, newborn
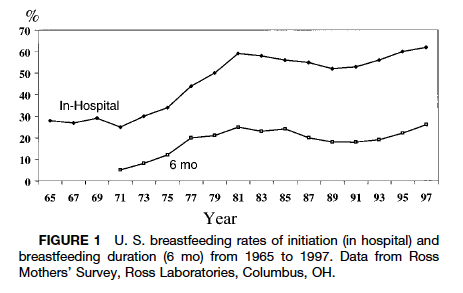
Nineteen seventy two was notable for many things aside from the year of my birth. Canada defeated the Soviets in the summer series, the Watergate scandal took down a Presidency, The GodFather was released and for the purposes of this post breastfeeding rates in the US reached an all time low of 22%. For an excellent review of the history of breastfeeding the article by AL Wright is excellent.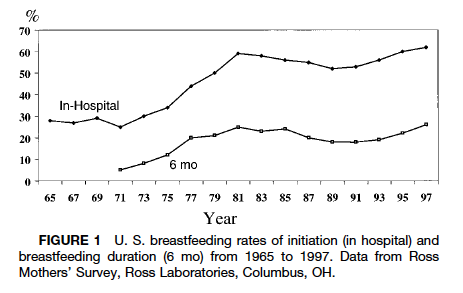
Rates of breastfeeding began a steady decline in the 1960s as more and more women entered the workforce and seemingly had to choose between employment and breastfeeding. This was a time when it was not seen as being acceptable to breastfeed in public (although that is not the case in many places still to this day) and the workplace was not as conducive to supporting women as in current times (think onsite daycares). Add to this that the 1970s also saw a backlash of sorts in the appeal of breastfeeding due to science “perfecting” a better source of nutrition in formula and we had the low rates that we did. In fact through discussions with parents from that generation, mother’s who chose to breastfeed may have been viewed by some as being silly for not using something like formula that could let the whole family in on the experience. Mom, Dad, kids and grandparents could all take part in the wonderful act of feeding. Why be so selfish?
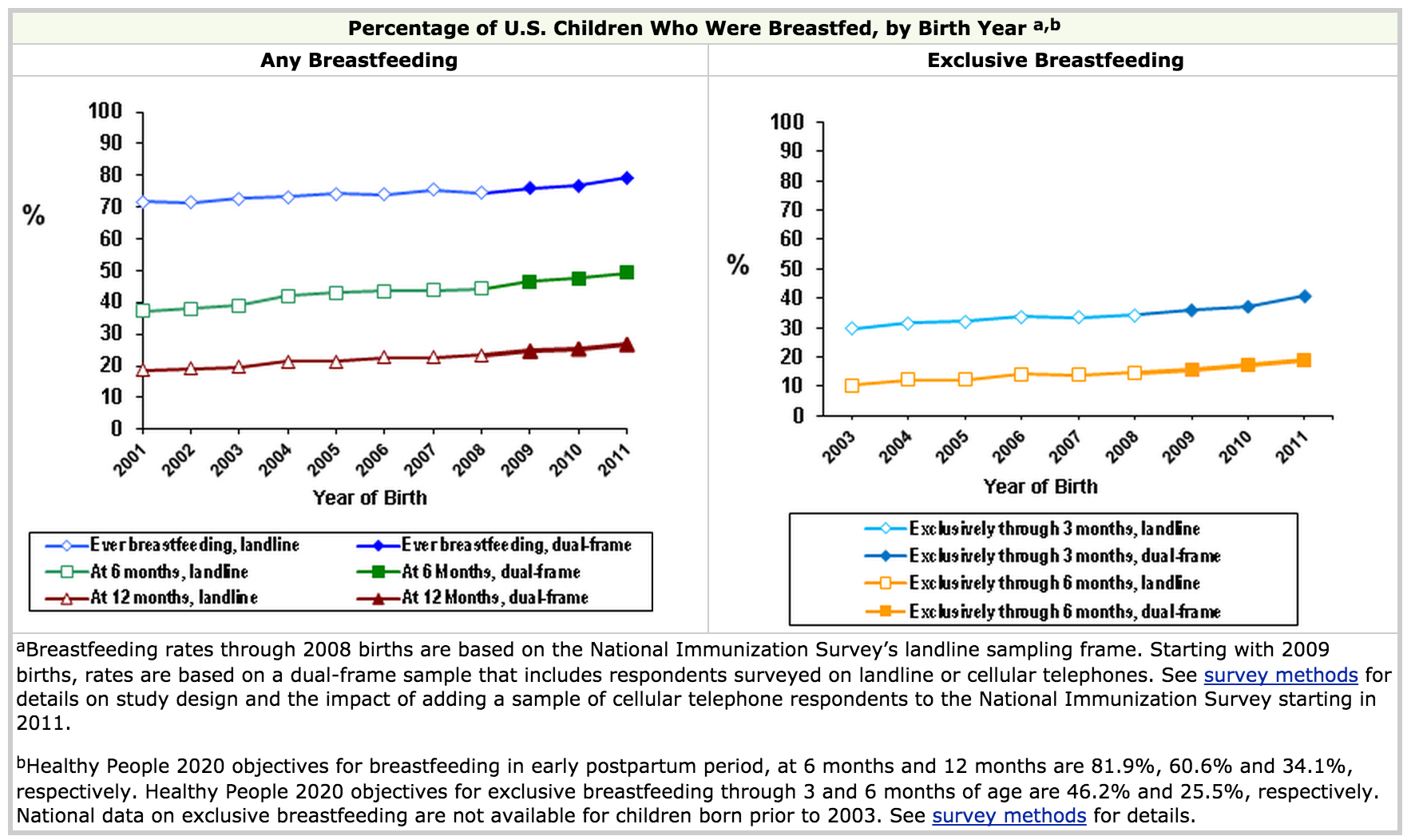
Following this period as research began to demonstrate improved outcomes with breastfeeding including reductions in atopic disease, less hospital admissions and more recently positive impacts on intelligence and your microbiome the trend reversed. In fact, as the above graph demonstrates, rates approximating 70% were reached by the late 1990s. Since that time the CDC has shown that initiation rates have continued to rise and currently are at the highest documented levels in history.
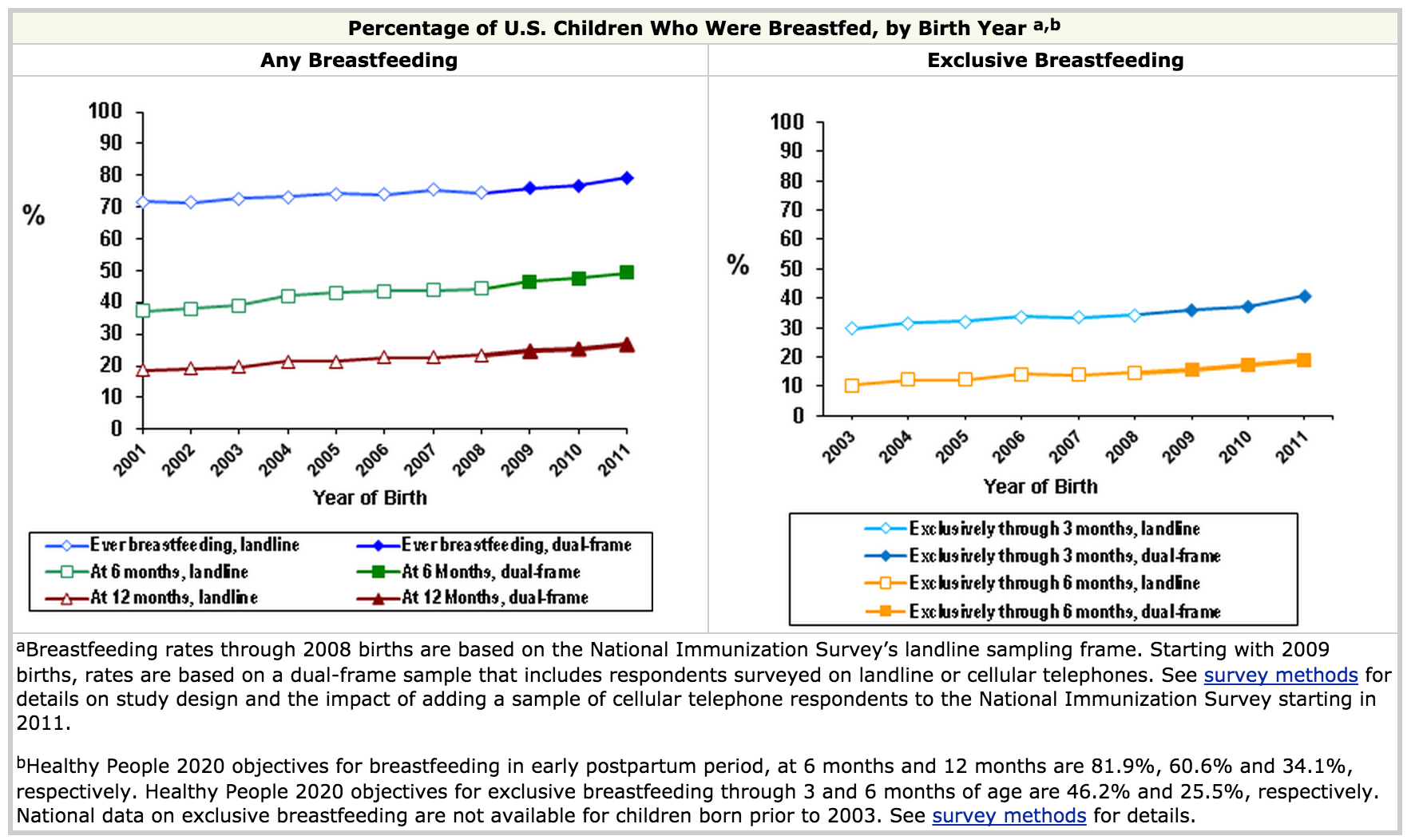
Looking at the CDC data though reveals some very important information. While the rates of any breastfeeding reach 80%, the rates at 6 months hover around 50%. This means that a significant portion of US women are using some formula when they come home and from the graph on the right about 35% by three months are exclusively breastfeeding. This number is far short of the goal the WHO has set to encourage exclusive breastfeeding for the first 6 months however it is a remarkable achievement for infant health.
http://www.who.int/topics/breastfeeding/en/
A recent trend on social media and print media has been the Brelfie. As you may know, this involves taking a picture of yourself breastfeeding your baby and posting it in one forum or another. This has been popularized by many celebrities and made it’s way onto the cover of Elle magazine this month.
 So called Lactavists have been overjoyed to see such public acceptance and promotion of breastfeeding. As a Neonatologist I am delighted to see such high rates of breastfeeding and with it the beneficial effects that it brings.
So called Lactavists have been overjoyed to see such public acceptance and promotion of breastfeeding. As a Neonatologist I am delighted to see such high rates of breastfeeding and with it the beneficial effects that it brings.
Curiously, though all of this attention and promotion of breastfeeding has created a culture that is now being called bressure. This is defined as pressure to breastfeed and was the subject of a recent survey by Channel Mum in the UK. The highlights of the survey that went out to 2,075 mums showed:
– 16 per cent of bottle-feeding mums have been on the receiving end of cruel comments from other mothers they know
– one in 20 being attacked on social media
– 69 per cent of bottle-feeding mums said they had been judged negatively
– 41 per cent made to feel they have ‘failed as a mum and failed their child’ by not breastfeeding
– 15 per cent of mums have even lied to cover up their bottle-feeding and appear to be ‘better’ mums.
This so called bressure has led to a public campaign to increase awareness of the harassment that some mothers feel which involves taking selfies with cards having one word describing what breastfeeding meant for them. A video from Channel Mum can be seen here
Channel Mum Video Response to Brelfies
While I am all for breastfeeding, I find it peculiar that the experience that breastfeeding mothers (all 22% of them) had in 1972 is now being felt by a larger percentage in 2015 who are bottle feeding. It is unfortunate that assumptions are being made of many of these women who put a bottle in the mouths of their infants. How many times does one conclude that the mother simply chose not to breastfeed because they were worried about the way their breasts would be affected cosmetically or that they simply chose to go back to work and breastfeeding would just get in the way. I suspect in most cases the truth is much different. Many of these mothers have tried to breastfeed but couldn’t produce enough. Others may have suffered from cracked nipples, mastitis, abscesses or due to prior surgery were unable to produce milk. Many such mothers have agonized over their “failure” to do something that they hear “everyone can do”. While they are told it takes some work for many that is a huge understatement. Is it not bad enough that these women have suffered the feeling of failure? To be looked at or spoken to in a disapproving way does nothing to support them. Add to this that by 3 months of age at least in the US 65% of mothers are providing some formula and it seems silly to take the “high and mighty” approach in the first couple of months and assume the worst of these women. Many of the “breastfeeders” will soon enough join the ranks of those using some formula.
Maybe the better option is to try and help. Many of the above problems whether it be producing enough quantity or pain related to breastfeeding can be addressed through tips on technique. While I am not an expert in this, hospitals would do well to increase staffing of on site lactation consultants to help mothers who wish to breastfeed get off on the right foot so to speak. A larger working force of midwives in North America in particular could certainly provide help in this regard. What I can say is that if a woman suffers a bad experience with breastfeeding in their first pregnancy the likelihood they will try again the next time is lower especially if we as a society make them feel like a failure.
Yes we need to promote breastfeeding and we should do what we can to follow the WHO recommendations and minimize the use of formula when possible. While bressure may have been intended to yield something good we need to be sensitive. Perhaps a better strategy next time a friend says they are going to use formula is to ask if they are having trouble with breastfeeding and if they need some help. Not having the discussion will ensure that nothing changes and a chance to do something will be lost due to misdirected bressure.
by All Things Neonatal | Mar 17, 2015 | Breastfeeding, Breastmilk, Infection, Pregnancy
Its hard not to hear about probiotics these days. They are in our grocery stores as supplements to yoghurt and other foods and can be purchased in health food stores or at your local pharmacy. They appear to be everywhere as word spreads about the importance of your microbiome in maintaining good overall health.
It didn’t take long for clinician scientists to turn their attention to the neonate who is at risk of necrotizing enterocolits (NEC). It has been known for some time that formula feeding versus breast milk plays a role in the development of NEC as premature infants fed formula repeatedly were found across studies to have a higher incidence of NEC. The evidence is so strong in fact that the Cochrane review on the subject states “Enteral supplementation of probiotics prevents severe NEC and all cause mortality in preterm infants. Our updated review of available evidence strongly supports a change in practice.“ If you have read such reviews you know that they rarely come out this strong in their support of something! Furthermore, infants fed formula may have a different preponderance of more pathogenic bacteria in the colon and less lactobacillus and bifidobacterium species. The idea behind providing probiotics to neonates would therefore be to repopulate the intestine of these vulnerable infants with good bacteria and potentially reduce the incidence of a devastating condition like NEC.
If only it were that easy though
The issue of using Probiotics in preterm infants is a contentious one to say the least. While the evidence appears to indicate an overall benefit in terms of reducing rates of NEC there remain concerns regarding the safety of providing bacteria to this population even though the bacteria are thought to be beneficial. The people who urge caution in the use of probiotics say so due to a few reports of sepsis after the introduction of probiotics with the organism that the patient was provided or with a different species that was could be traced to a contaminated product. As noted in an article on CBC recently these products fall under the category of a nutritional product rather than a medication with Health Canada and therefore are not subject to the same rigorous quality control standards as other comparable medications would be.
Others while recognizing the potential for contamination and sepsis would argue that the risk is low compared to the benefit provided to the infants overall and therefore claim benefits outweigh risks.
Manipulating Breastmilk in a Double Bling RCT
Given the above concerns regarding administration of these products to neonates I was excited to see the randomized double blinded study by Benor S et al; Probiotic supplementation in mothers of very low birth weight infants. This study enrolled mother and infant pairs within 72 hours after birth to commence on maternal treatment with Lactobacillus acidodphilus and Bifidobatera lactis versus placebo until discharge. The rationale for giving probiotics to lactating mothers was based on a previous study showing less atopic dermatitis in the offspring of mothers who took such treatment while breastfeeding and in a study of breast milk demonstrating lower levels of the inflammatory cytokine transforming growth factor beta (TNF-B). Less inflammation might equate to less NEC.
The primary outcome was Bell Stage II NEC and the investigators required 90 mothers in each arm to show a difference in the incidence of NEC based on previous work in their centre. All included pairs needed to be providing >50% EBM in order to minimize any effect from formula. The overall incidence of NEC at the completion of the study was 27% in the placebo group vs 12% probiotic group and for NEC II 18% vs 4% in those treated with probiotics. The rates of NEC were quite high compared to what we typically see and the authors noted that even for their site (for uncertain reasons) there was a higher rate than they expected. Neither of the rates of NEC were statistically different (both reached p=0.15 levels) but there was a significant issue with this study.
The total recruitment was 25 in the probiotic and 33 in the control arm. This was a far cry from the estimated 90 needed per side. The reason for this goes back to the start of this blog entry. The study needed to be stopped due to poor enrolment. Why so low? The majority of mothers approached for this study did not want to risk not getting probiotics so they opted to simply take them due to the perceived health benefits that as adults they already believe exist. Sadly I think this problem would resurface in many places if the study was replicated. This loss of equipoise by the families will make obtaining consent for such studies very difficult and we may not get a satisfactory answer.
Interestingly the authors of this study also measured TNF-B and found a strong trend towards lower levels in the breast milk of the probiotic supplemented group matching the trend towards less NEC.
I sincerely hope that another study such as this can be done without such issues in recruitment as the strategy would address the issue of not providing the bacteria directly to the neonate while still potentially reaping the benefits of less NEC. For now we will have to wait and see.
by All Things Neonatal | Mar 12, 2015 | General Comments

I would like to thank each and every one of you for your words of encouragement over the last three weeks since the inception of this blog. Today marked a significant event by surpassing 100 followers who receive an email with each blog post. As of tonight, there have also been almost 2000 viewings of these posts from at least 20 countries worldwide. I find these metrics informative as I really have no idea how many views happen on Facebook or Twitter but with the blog data I get a sense of how many of you are out there!
I have thoroughly enjoyed writing these pieces and really appreciate the feedback on each topic. The last few weeks have included correspondence with someone from another country who was unaware that Propranolol could be used for hemangiomas and a practical suggestion for starting children on propranolol in a day clinic type of environment. I look forward to the opening of such a clinic in our hospital in the next year or so. There is no doubt that the topic that garnered the most attention was the use of breast milk by body builders. Although this was a more playful topic it did raise awareness of the use of donor breast milk and who knows whether or not a unit somewhere may look into this through the communication that the post generated. The Sympathetic Note to the Anti-Vaxxers caused an explosion on Twitter that left me exhausted after 3 days of exchanges with people opposed to vaccination. I have to say that although it was tiring, the amount of websites, articles and information from that side of the argument that I was provided is worthy of a post in and of itself! I learned a lot from individuals on the other side of the promoting health coin and I feel as if I am a better doctor for it as I now have better insight into the basis for many of their arguments.
I have to say the pinnacle of this experience however was an exchange with someone who attributed their child’s autism to the MMR vaccine. After a bit of a lengthy exchange I was sent a picture of her beautiful daughter with a thank you for having given them some relief after reading the post on MMR. Their daughter was lovely as was the knowledge that I had helped someone who I would have otherwise never met if it weren’t for this medium.
Your support has kept my enthusiasm for writing up and on a local front I also want to thank the doctors, nurses, dieticians, RRTs and others who have encouraged this medium for education. I have really enjoyed being stopped in the NICU, IMCN or hallways to chat further about this post or that. It means a lot!
Moving forward I look forward to many more opportunities to share with you. I would like to add that I have created a twitter feed at @NICU_musings to talk about these and other topics not on the blog for those of you who are more bent on Twitter. There is also now a Facebook page at https://www.facebook.com/allthingsneonatal where discussion can also take place if you are more of a Facebook fan.
I will leave you with this news story I read tonight which reminded me of the power of community generosity that many of you know we have been blessed with here. Charitable giving is a very special and important thing and this story seemed right to finish off on a high note.
http://www.yourerie.com/news/news-article/d/story/pay-it-forward-check-helps-neonatal-intensive-care/16215/VCOYMz8je0631nC0dShYQQ

by All Things Neonatal | Feb 28, 2015 | Breastmilk
I wrote this post almost a year ago and could not believe such practice was going on. Here we are this week and the following was published in Men’s Health magazine indicating breast milk consumption by body builders has not gone away quietly.
For my own thought on this including updates to the original post please read below.
It may seem like I am making a joke but sadly it is the real deal as you can see from the USA Today video released in the past couple weeks. The benefits of drinking breast milk to add muscle mass has spread quickly among that community. That is not to say that the majority are using it but there definitely is a following. Taking a look at the website “Only The Breast“ reveals the sad truth. There are currently 6368 classifieds for women selling breast milk with 804 of these women specifically targeting men who wish to buy (Update: As of February 23, 2016 the number of offerings has risen to 10135 with 1294 offering to men so the problem is getting worse not better!). Contrast this with only 113 women willing to donate their milk. This is only one site as women are also resorting to Craigslist and Kijiji to just name a couple of alternatives. There is money in selling breast milk and sadly those who most need it may not be getting it.
The amount of evidence supporting the benefits of an exclusive breast milk diet for preterm infants in particular has exploded in the past few years. There is no question in my mind that breast milk should be distributed to babies whose mothers are unable to provide enough milk for them while in the hospital. The proven reductions In necrotizing enterocolitis; a major cause of morbidity and death in the NICU are reason enough to exclude formula from a low birth weight preterm infant. See Formula versus donor breast milk for feeding preterm or low birth weight infants.
If each case of necrotizing enterocolitis costs the US Health care system approximately $150000 imagine how much money could be saved when estimates from other studies such as the one by Sullivan et al target the reduction in NEC at about 70%. In our own centre with approximately seven cases per year we would expect to see 5 less babies affected by this per year.
Aside from the above concerns about using breast milk in a population that has no likely benefit there is substantial risk to purchasing milk online. As mentioned in the USA today video the FDA has spoken out against such practice due to high likelihood of contamination by bacteria secondary to non standardized methods of storage. The article cited in the video can be found here.
Where is the harm?
The rate of contamination at 74% is frightening and in turn puzzling that people so focused on treating their bodies like a temple would consider ingesting it. A search on Pubmed using a combination of different search criteria combined with a broader search using google failed to come up with one article showing any evidence supporting the consumption of breast milk by those wishing to build muscle mass. Given the lack of evidence and the potential for harm this is a practice that needs to be eliminated as soon as possible. The selling of excess supply from mothers to males who have no potential to benefit is tragic. Each ounce that is sold in such a way is a waste of liquid gold and in essence is “stolen” away from the pool of milk that could be sent to a Human Milk Banking Association of North America approved Milk Bank. All Milk Banks that follow their standards provide breast milk which has is safe to consume as opposed to those sourced from online sites. Furthermore newer organizations such as the Mother’s Milk Coop pay for such milk as an alternative for mothers seeking income through the selling of their excess supply. There are of course possible issues that arise from paying mothers for their milk but if they are looking to profit then perhaps the coop is the preferred option. Selling milk and giving formula to their infants is not something I condone but if they are going to do it anyway the online route is the worse of the two options.
It is my hope that this post serves to educate even one mother that while their efforts to earn some income are understood there are better and safer ways to do so than an unregulated site such as “Only The Breast” or others. If you come across anyone who even hints at selling their milk through the means mentioned above, direct them to the closest breast milk bank or to the Coop mentioned above (recognizing that this too is not ideal)!
Finally, with the significant impact exclusive breast milk diets can have on outcomes for premature neonates hospitals worldwide would be wise to follow the lead of the University Hospital of Limerick who was just honoured for their initiative to ensure near 100% use of breast milk in their hospital through the use of donor milk.
Encourage your local hospitals to acquire donor breast milk if they don’t have a program to do so already. If they already have a program work with your health region to expand it.
Money very well spent I say.