It’s World Prematurity Day today and if you are a parent or are caring for a baby who has just entered this world before 37 weeks GA you are now part of a membership that counts 15 million new babies each year according to the WHO’s data. As I tell most new parents who have a baby admitted to our unit “It’s ok to take some time to adjust to this. You didn’t plan on being here”. That is true for most who go into spontaneous labour but of course those who are electively delivered due to maternal or fetal indications that have been followed closely often have time to prepare for the journey to the NICU. Many of these parents will have had the opportunity to visit the NICU or even connect with other parents before the anticipated birth of their child to at least get a glimpse into what life is like in the NICU. Much has been written about parental stress and methods to reduce it and I find that a piece that appeared in the Huffington Post offers some good pointers to helping parents manage the transition from pregnancy to NICU. The piece is entitled 5 Things Never To Say To Parents Of Preemies (And What To Say Instead).It is well worth a read but the one thing that stuck out in my mind is one very important thing to say.
Congratulations on the birth of your baby
There is no doubt that the family who gives birth to a preterm infant is experiencing stress. What may be lost in the first few days of surfactant, central lines and looking for sepsis among other things is that a new member of the 15 million strong has entered this world. They have a new child and just like anyone else should receive a congratulations. No one needs to tell them to be worried. They already are and likely view many of the possibilities more pessimistically than you do. Taking a moment to say congratulations though may go a long way to reminding them that amidst all this stress there is something to rejoice in and look to the future. If we aren’t supportive then I have no doubt the subconscious message is that they shouldn’t have hope either. I am not suggesting that we sugarcoat what is really going on but one can be honest about likely outcomes and still celebrate the arrival of a new baby. Much has also been written recently about a number of strategies to reduce stress in the NICU such as skin to skin care, integration of families more closely into the patient care team and forming parent support groups just to name a few. What else can be done to improve the quality of life for parents going through this journey?
Enrol Your Baby In A Research Study
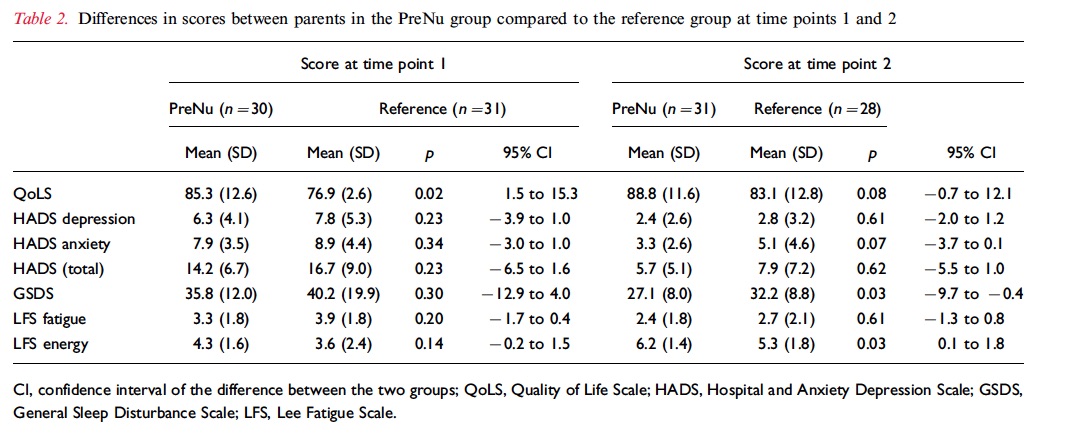
I work in an academic centre and given the volume of research projects at any given time there is a need to approach families and sometimes quite soon after delivery. interestingly, I have heard from time to time that individuals have been hesitant to approach families due to a feeling that they are overwhelmed and won’t be receptive to being approached in this fragile state. I am guilty of the same thoughts from time to time but maybe it is time I reconsider. Nordheim T et al just published an interesting study on this topic entitled Quality of life in parents of preterm infants in a randomized nutritional intervention trial. This study was actually a study of parents within a study that called the PreNu trial that involved an intervention of a energy and protein supplemental strategy to enhance weight at discharge. The trial was an RCT and unfortunately although well intentioned was stopped when the intervention group was found to have an unexpected increase in sepsis rates. Although this study did not ultimately find a positive outcome there were additional analyses performed of quality of life and parental stress at two time points the first being during the hospital stay and the second at 3.5 years of age. The patients were all treated the same aside from the nutritional intake and in the end 30 intervention parents and 31 single parents not enrolled in a study (many in couples) participated in the study. In followup a little less than 70% completed the stress measures at 3.5 years. The results are found below.
How Do We Interpret This
The parents in this study who were part of the intervention group were about 3 years older so perhaps with more life experience may have developed some better coping strategies but during the hospital stay those who participated in research had better measures of quality of life and at three years better reports of sleep and energy levels. The study is quite small so we need to take all of this with a grain of salt with respect to the 3.5 year outcomes as there are so many variables that could happen along the way to explain this difference but I think it may be fair to acknowledge the quality of life measure during the stay. Why might parents report these findings? The finding of better quality of life is especially interesting given that more patients in this study had sepsis which one would think would make for a worse result. Here are a few thoughts.
Involvement in research may have increased their knowledge base as they learned about nutrition and expected weight gain in the NICU.
Frequent interaction with researchers may have given them more attention and with it more education.
Some parents may have simply felt better about knowing they were helping others who would come after them. I have heard this comment myself many times and suspect that it would be attributable at least to a certain extent.
A better understanding of the issues facing their infants through education may have reduced stress levels due to avoiding “fear of the unknown”.
Regardless of the exact reason behind the findings what stands out in my mind is that participation in research likely provides comfort for parents who are in the midst of tremendous stress. Is it the altruistic desire to help others or being able to find something good in the face of a guarded outlook? I don’t know but I do believe that what this study tells us is that we shouldn’t be afraid to approach families.
After first congratulating them give them a little time to absorb their new reality and then offer them the chance to improve the care for the next 15 million that will come this time next year for World Prematurity Day 2017.
I have probably received more requests for our glucose gel protocol than any other question since I started writing on this blog. Dextrose gel has been used more and more often for treatment of hypoglycemia such that it is now a key strategy in the management of low blood sugar in ours and many other institutions. If you are interested in the past analyses of the supporting trials they can be found in these posts; Glucose gel For Managing Hypoglycemia. Can We Afford Not To Use It? and Dextrose gel for hypoglycemia: Safe in the long run? As you can tell from these posts I am a fan of dextrose gel and eagerly await our own analysis of the impact of using gel on NICU admission rates for one!
But What If You Could Prevent Hypoglycemia Rather Than Treating It?
This is the question that the same group who has conducted the other trials sought to answer in their dose finding study entitled Prophylactic Oral Dextrose Gel for Newborn Babies at Risk of Neonatal Hypoglycaemia: A Randomised Controlled Dose-Finding Trial (the Pre-hPOD Study). I suppose it was only a matter of time that someone asked the question; “What if we prophylactically gave at risk babies dextrose gel? Could we prevent them from becoming hypoglycemic and reduce admissions and improve breastfeeding rates as has been seen with treatment of established hypoglycemia?” That is what they went out and did. The group selected at risk patients such as those born to mothers with any type of diabetes, late preterm infants, SGA and others typically classified as being at risk but who did not require NICU admission at 1 hour of age when treatment was provided. The primary outcome was hypoglcyemia (<2.6 mmol/L) in the first 48 hours. Secondary outcomes included NICU admissions, breastfeeding rates in hospital and after discharge as well as formula intake at various time points.
The study sought really to serve as a pilot whose goal was to determine when compared to placebo whether several different regimens could prevent development of hypoglycemia. The groups were (with the first dose in each case given at 1 hour of age):
Single dose of 40% dextrose gel – 0.5 mL/kg
Single dose of 40% dextrose gel – 1 ml/kg
Four doses of 0.5 mL/kg given every three hours with breastfeeding
A single dose of 1 mL/kg then 3 X 0.5 mL/kg given q3h before each breastfeed.
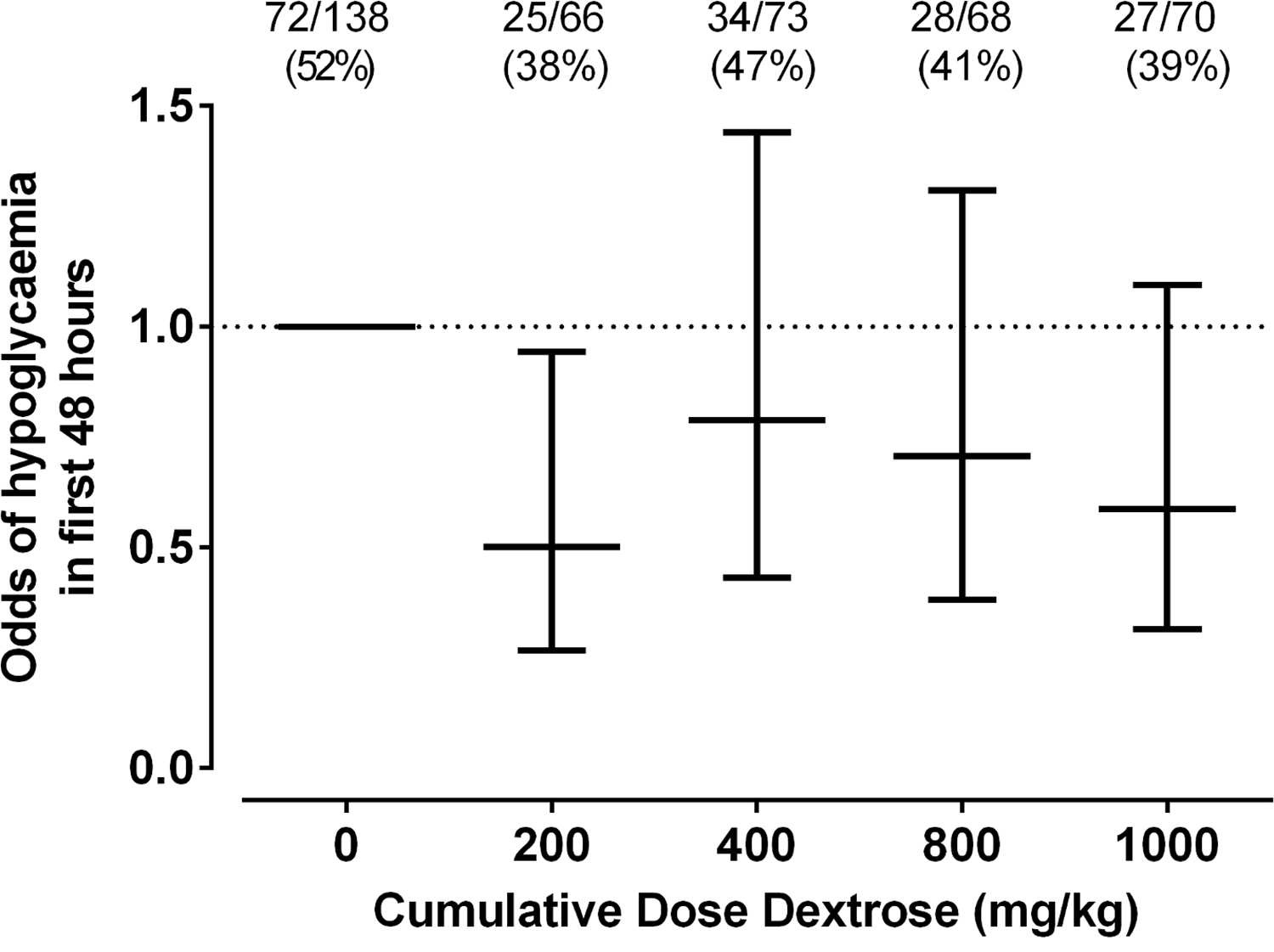
In total 412 patients were randomized into 8 different groups (4 treatment and 4 placebo).
As The Saying Goes, Less Is More
The only dose of dextrose that reduced the risk of hypoglycemia in the first 48 hours was 0.5 mL/kg which provides 200 mg/kg of dextrose which is the same as a bolus of IV dextrose when giving 2 mL/kg of D10W. Curiously using a higher dose or using multiple doses had no effect on reducing the risk. Based on a difference of 14% between placebo and this group you would need to treat roughly 7 patients with dextrose gel once to prevent one episode of hypoglycemia. Also worth noting is that admission to NICU was no different but if one restricted the reason for admission to hypoglycemia the difference was significant (13% vs 2% risk; p = 0.04). What was not seen here was a difference in rates of breastfeeding and much effect on use of formula.
Why Might These Results Have Occurred?
Insulin levels were not measured in this study but I truly wonder if the reason for hypoglycemia in the other groups may have been transient hyperinsulinemia from essentially receiving either a very large load of glucose (1 mL/kg groups) or effectively 4 boluses of glucose in the first 12 hours of feeding. Rebound hypoglycemia from IV boluses is a known phenomenon as insulin levels surge to deal with the large dextrose load and I can’t help but wonder if that is the reason that all but the single dose regimen had an effect. It is also worth commenting that with so many secondary outcomes in this study the p values needed to reach significance are likely much smaller than 0.05 so I would take the reduction in NICU admissions for hypoglycemia with a grain of salt although at least the trend is encouraging.
I wouldn’t change my practice yet and the authors do acknowledge in the article that a much larger study is now being done using the single dose of 0.5 mL/kg to look at outcomes and until that is published I don’t think a practice change is in order. What this study does reinforce though is that providing multiple doses of dextrose gel may yield diminishing returns. While the goal here was prophylaxis, I can’t help but think about the patients who are symptomatic and receive two or three gels and still wind up with an IV. Could it be the same rebound hypoglycemia at play?
We also have to acknowledge that even if this is an effective preventative strategy, is it in the best interests of the babies to all receive such treatment when at least in 6 babies they wouldn’t have needed any? Could such treatment simply be reserved as has been done for those who develop hypoglycemia? Those who question the safety of the ingredients such as dyes that are found in the product may want some long term safety data before this becomes routine in at risk babies but it won’t surprise me if such strategies become commonplace pending the results of the larger trial on the way.
In April of this year the ALPS trial results were published in the New England Journal of Medicine (Antenatal Betamethasone for Women at Risk for Late Preterm Delivery) and I took the time to review the paper at the time Antenatal Steroids After 34 weeks. Believe the hype? In the analysis I focused on an issue which was relevant at the time, being a shortage of betamethasone. In a situation when the drug of choice is in short supply I argued that while the benefits of giving steroid to women at risk of delivery between 34 0/7 to 36 6/7 weeks was there, if I had to choose (as I did at the time) I would save the doses for those at highest risk of adverse outcome. Since the blog post though a couple of things have come out in the literature that I believe are worth sharing as it could truly influence practice.
The American College of Obstetricians and Gynecologists, moved by the results of the ALPS trial issued the following recommendations (shortened in places).
Betamethasone may be considered in women with a singleton pregnancy between 34 0/7 and 36 6/7 weeks gestation at imminent risk of preterm birth within 7 days.
Monitoring of late preterms for hypoglycemia (already being done)
Do not give in the setting of chorioamnionitis.
Tocolysis or delayed delivery for maternal indications should not be done in order to to allow for administration of late preterm antenatal corticosteroids.
Do not provide if the pregnancy was already exposed to antenatal corticosteroids.
The exclusions above such as twins and triplets, diabetic pregnancies and previous receipt of steroids were included since the study had not included these patients. As the ACOG states in the summary, they will be reviewing such indications in the future and providing recommendations. I would imagine that if I were in a US based practice then this post might seem like old news since many centres would have started doing this. Given that the readers of this blog are based in many different countries around the globe and at least in Canada this has not become commonplace I thought it would be worth the update!
I posted the abstract for this review on my Facebook page the other day and it certainly garnered a lot of interest. Some of my readers indicated the practice is already underway. I was curious what a systematic review would reveal about the topic since the ACOG was so moved by the ALPS study in particular. Perusing through the Society of Obstetricians and Gynecologists of Canada (SOGC) I can’t find any commentary on this topic and certainly there are no new clinical practice guidelines since the ALPS study landed on my desktop.
Here are the pooled results from 6 trials:
Lower risk of RDS (relative risk 0.74, 95% confidence interval 0.61 to 0.91)
Mild RDS (0.67, 0.46 to 0.96)
Moderate RDS (0.39, 0.18 to 0.89)
Severe RDS (0.55, 0.33 to 0.91)
Transient tachypnea of the newborn (0.56, 0.37 to 0.86)
Shorter stay on a neonatal intensive care unit (−7.64 days, −7.65 to −7.64)
So across the board patients who receive antenatal steroids after 34 weeks still continue to see a benefit but looked at a different way the real benefit of the intervention is easier to see and that is through looking at the number needed to treat (NNT). For those of you who are not familiar with this analysis, this looks at how many patients one would need to treat in order to avoid the outcome in 1 patient.
For the outcomes above as an example the NNT for RDS overall is about 59 while for TTN 31 patients. Severe RDS which is less common after 34 weeks you might expect to require more patients to treat to help 1 avoid the outcome and you would be correct. That number is 118 patients. It is interesting to look at the impact of steroids in pregnancies below 34 weeks (taken from the Cochrane review on the subject) as the NNT there is 23! If you were to break these benefits down from 23-27 weeks though where the risk of RDS is quite high the NNT would be even lower. Steroids help, no question to reduce neonatal complications but as you can see even when there is a reduction in risk for various outcomes, the number of women you need to treat to get one good outcome is quite different.
Some Discussion With Obstetrics Is Needed Here
As you read through this post you may find yourself saying “Who cares? if there is a benefit at all most moms would say give me the steroids!” The issue here has to do with long term outcome. To put it simply, we don’t know for this type of patient. We know clearly that for patients at high risk of adverse outcomes eg. 24 week infant, the reduction in risks of infection, NEC, PDA, BPD etc from receiving antenatal steroids translates into many long term benefits. What about the patient who say is 35 weeks and would have none of those risks? Yes we are avoiding some short term outcomes that let’s be honest can be scary for a new parent but what are we trading this benefit for. The concern comes from what we know about steroids impact on the developing brain. Steroids lead to a developmental arrest but in very preterm infants there is no doubt that the protective effect on all of these other outcomes more than offsets whatever impact there is there. Incidentally I wrote about this once before and the section of interest appears at the end of the relevant post Not just for preemies anymore? Antenatal steroids for elective c-sections at term. In the absence of these other conditions could there be a long term impact in babies 34 – 36 6/7? My suspicion is that the answer is no but discussion is needed here especially in the absence of an endorsement by our Canadian SOGC. Having said all that I expect the future will indeed see an expansion of the program but then I do hope that someone takes the time to follow such children up so we have the answer once and for all.
As a young resident I have a vivid memory of a baby with CDH having saturations of 60 – 65% despite HFOV, paralysis and alkalinization (yes we used to do that). It was at that time that I pretty much threw my hands in the air and declared there was really nothing left that we could do. One of my mentors, a very wise Neonatologist Dr. Henrique Rigatto looked at me and said “why don’t we try inhaled nitric oxide?” Being the resident immersed in the burgeoning field of evidence based medicine I questioned him on this stating “But the evidence shows no benefit of iNO in CDH in any trials”. He looked back at me and asked “Are you prepared to let this baby die without even trying it?”. When put that way I answered shyly that I would order the iNO and… it worked. Whether it was coincidence or not I cannot say but I felt he had a point which I have shared many times with students over the years. A drug may not show a benefit in a clinical RCT so at a population level it should not be our ” go to” drug of choice but on an individual level as a last resort sometimes these medications for an individual patient may make a difference. Looking at it from a different standpoint one might say it falls into the “can’t hurt but might help” category of therapy.
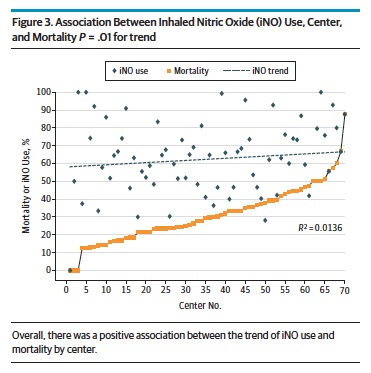
The study looked at 2047 patients treated with iNO most of whom received 20 ppm of iNO. Interestingly about 15% of the patients treated with iNO did not have pulonary hypertension on ECHO. The study found a positive association between centres using iNO and mortality. Moreover as the number of centres increased over time that used iNO so did the overall mortality in the study cohort. Beyond just looking at the trend in mortality with increasing use the authors took this one step further and used the statistical technique of propensity scoring to determine the attributable risk to mortality of using iNO in patients with CDH.
Propensity scoring is an interesting technique that one can use to estimate risk when it is unlikely that a randomized controlled trial will be available and this is one of those cases. The technique uses an approach which strives to balance the variables that determined why different patients received a treatment so when comparing the outcomes of the two groups you manage to isolate the effect to just the treatment that is being studied. In this case the technique indicates that the estimate of harm is estimated to be 15% meaning that there is an estimated 15% increase in mortality for patients with CDH treated with iNO regardless of the indication.
So what to do with our next patient?
I can’t help but think back to the words of one of my mentors and ask myself what I would do if I was confronted with a patient who had CDH and was saturating poorly. I think what this study adds perhaps is that one should tread carefully with iNO in the setting of CDH. Maybe the overall message is that one should not jump to use iNO early in treatment. Optimizing ventilation, use of analgesics and sedation and even paralysis may be a better approach to controlling oxygenation than early iNO. When all those have been tried though and the patient is still not responding I think those wise words from long ago carry a lot of weight. “Are you prepared to let this baby die without even trying it?”
When mortality is already a strong possibility I believe at least for me the answer will remain no. I think it is important to keep iNO in your back pocket but to let a patient die without trying would leave me forever asking “what if”. That is a question I am certainly not comfortable asking at all.
This is a title that I hope caught your eye. In the nearly twenty years I have been in the field of Pediatrics the topic of parking being a barrier to parental visitation has come up again and again. A few years ago the concern about the cost of parking was so great that I was asked if I could find a pool of donors to purchase parking passes to offset the burden to the family. The theory of course is based on the idea that if parking were free in the NICU parents would visit more. If parents visit more they will be more involved in the care of their baby, more likely to breastfeed and with both of these situations in play the infant should be discharged earlier than other infants whose parents don’t visit. Try as I might it was a tough sell for donors who tend to prefer buying something more tangible that may bear their name or at least something they can look at and say “I bought that”. This is quite tough when it comes to a parking stall and as such I am still looking for that elusive donor. Having said that, is there any basis to believe that free parking is the solution that will deliver us from minimal visitation by some parents?
A Study May Help Answer The Question
Northrup TF et al published an article that was sent my way and to be honest I couldn’t wait to read it. A freeparking trial to increase visitation and improve extremely low birth weight infant outcomes. This is like the holy grail of studies. A study that gets right to the point and attempts to answer the exact question I and others have been asking for some time. The study took place in Houston, Texas and was set up as an RCT in which families were randomized into two groups. Inclusion criteria were birth weight ⩽1000 g, age 7 to 14 days and deemed likely to survive. Seventy two patients were enrolled in the free parking group while 66 were placed in the usual care. Interestingly the power calculation determined that they would need 140 to show a difference so while 138 is close it wasn’t enough to truly show a difference but let’s see what they found.
The Results
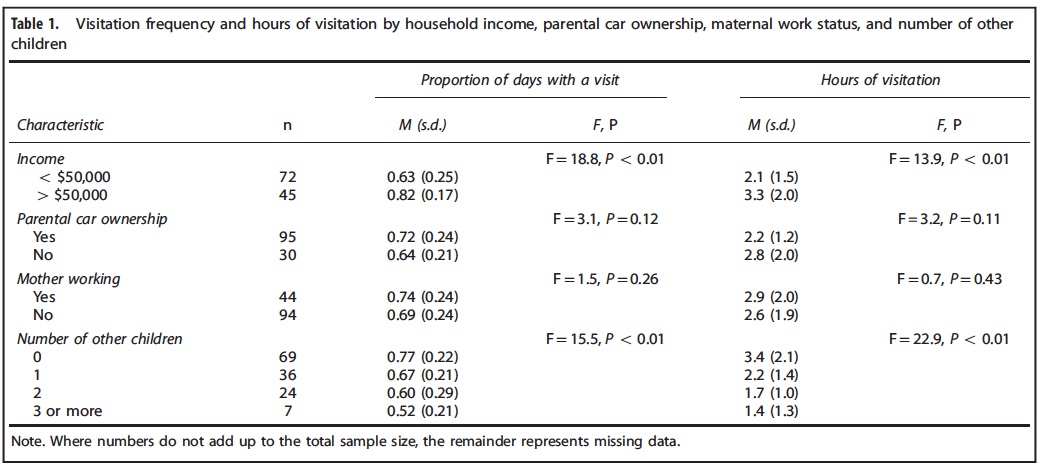
Free parking made absolutely no difference for the whole group. Specifically there was no difference in the primary outcome of length of stay or hours spent per visit. Some interesting information though that may not be that surprising was found to be of importance in the table below.
It may not seem like a surprise but the patients who were more affluent and those who had less children tended to visit more. The latter makes a lot of sense as what are many people to do when they have one or more other children to care for at home especially in the face of little support? Would free parking make one iota of difference if the barrier has nothing to do with the out of pocket cost?
The conclusion was that the strategy didn’t work that well but as you may have picked up I think the study was flawed. By applying the strategy to all they were perhaps affected by choosing the wrong inclusion criteria. Taken to an extreme, would a 50 million dollar Powerball winner care one bit about parking vouchers? It wouldn’t make any difference to whether they were going to come or not. Similarly a single mother with 5 other kids who lives below the poverty line and has little support is not going to come more frequently whether they have a voucher or not.
What if the study were redone?
I see a need to redo this study again but with different parameters. What if you randomized people with a car or access to one who lived below a certain income level and had a committed support person who could assure that team that they could care for any other children the family had when called upon? Or one could look at families with no other children and see if offering free parking led to more frequent visitation and then from there higher rates of Kangaroo Care and breastfeeding. I for one haven’t given up on the idea and while I was truly excited to be sent this article and sadly initially dismayed on first read, I am hopeful that this story has not seen it’s end.
It is intuitive to me that for some parents parking is a barrier to visiting. Finding the right population to prove this though is the key to providing the evidence to arm our teams with evidence to gain support from hospital administrations. Without it we truly face an uphill battle to get this type of support for families. Stay tuned…
This is a posting of an article in Pediatrics. Always wondered whether this little venture of mine would be studied. Not this blog in particular but the whole concept in general! The credit of course for this post is not mine but Dr. Moreno who wrote the piece but as the link wouldn’t work well on the Facebook page independently here you go.
Mastering the Media: Physician bloggers identify benefits, barriers to using social media
Megan A.Moreno, M.D., M.S.Ed., M.P.H., FAAP
Dr. Moreno
A growing number of physicians use social media as a professional platform for health communication. This trend is not lost on medical students and residents, who are among the demographic described as “most connected” via social media.In 2014, a medical student asked me to serve as her mentor for a public health research project. The student, Lauren Campbell, was interested in studying how physician bloggers see themselves and their role as bloggers, as well as the benefits and risks of blogging as a doctor. Given the newness of physician blogging, the purpose of the study was to understand the perspectives and experiences of physicians who could be considered early adopters of using social media to distribute health information.
We recruited physicians to take part in the study through website searches for physician bloggers, and in-depth telephone interviews were conducted with those who agreed to participate. At the end of the interview, participants were asked if they could recommend other physician bloggers, a technique known as “snowball sampling.”
Seventeen physicians participated in the study, which recently was published in BMC Medical Informatics and Decision Making (http://bit.ly/2bFtno9). About one-third were female and 76% were pediatricians.
Transcripts were analyzed for common themes mentioned across interviews.
Participants identified multiple perceived benefits and barriers to social media use by physicians. Benefits included forwarding career endeavors, keeping up with medical literature and increasing public exposure for their practice. Barriers included time, administrative hurdles to get permission from their institution to blog and fear of saying the wrong thing.
In addition, four major themes were commonly discussed across interviews. First, participants often saw themselves as “rugged individualists” who set their own rules for social media health communications, like cowboys taming the Wild West.
Second, participants expressed uncertainty about boundaries and strategies for social media use. They identified many gray areas such as what to post, how to post and how to set boundaries.
Third, an interesting and unexpected finding was that most of the physician bloggers described using social media much like traditional media, as a one-way communication platform or “soapbox” rather than as an interactive forum.
Finally, participants had disparate views regarding the time involved in social media use; some felt they could fit blogging into their day, while others saw it as an impediment to patient care.
From this study, we concluded that much uncertainty remains regarding roles and responsibilities of physicians providing medical content within social media, and opportunities exist for providers to use social media platforms interactively and to their full potential.
It’s worth considering how the AAP Council on Communications and Media or the Academy could develop best practices to address some of this uncertainty and provide physicians with training or tools to use social media for its true interactive purpose. The hope is that future studies will investigate these key topics so the “Wild West” of physician blogging will become an integrated metropolis.
Dr. Moreno is a member of the AAP Council on Communications and Media Executive Committee.





 The study found a positive association between centres using iNO and mortality. Moreover as the number of centres increased over time that used iNO so did the overall mortality in the study cohort. Beyond just looking at the trend in mortality with increasing use the authors took this one step further and used the statistical technique of propensity scoring to determine the attributable risk to mortality of using iNO in patients with CDH.
The study found a positive association between centres using iNO and mortality. Moreover as the number of centres increased over time that used iNO so did the overall mortality in the study cohort. Beyond just looking at the trend in mortality with increasing use the authors took this one step further and used the statistical technique of propensity scoring to determine the attributable risk to mortality of using iNO in patients with CDH.