The importance of collaborating in a respectful manner cannot be overemphasized, as a calm and well prepared team can handle just about anything thrown their way. This past week I finally had the opportunity to take the 7th ed NRP instructor course. What struck me most about the new version of the course was not the approach to the actual resuscitation but the preparation that was emphasized before you even start! It only takes 30 seconds to establish who is doing what in a resuscitation and while it would seem logical to divide up the roles each will take on it is something that has not been consistently done (at least in our institution). When a baby is born and responds to PPV quickly, this may not seem that important but in a situation where a team is performing chest compressions, placing an emergency UVC and moving on to epinephrine administration it certainly is nice to know in advance who is doing what.
The Golden Hour
We and many other centres have adopted this approach to resuscitation and at least here developed a checklist to ensure that everyone is prepared for a high risk delivery. While teams may think they have all the bases covered, when heart rates are racing it may surprise you to see how many times crucial bits of information or planning is missed. As I told you in another post I will be releasing a series of videos that I hope others will find useful. The video in this case is of a team readying itself for the delivery of a preterm infant that they anticipate will have respiratory distress. Ask yourself as you watch the film whether your team is preparing to this degree or not. Preparing in such a fashion certainly reduces the risk of errors caused by assumptions about who is doing what or what risk factors are present.
As you can tell I am a big fan of simulation in helping to create high functioning teams! More of these videos can be accessed on my Youtube channel at
Positive pressure ventilation puts infants at risk of developing chronic lung disease (CLD). Chronic lung disease in turn has been linked many times over, as a risk for long term impacts on development. So if one could reduce the amount of positive pressure breaths administered to a neonate over the course of their hospital stay, that should reduce the risk of CLD and by extension developmental impairment. At least that is the theory. Around the start of my career in Neonatology one publication that carried a lot of weight in academic circles was the Randomized Trial of Permissive Hypercapnia in Preterm Infants which randomized 49 surfactant treated infants to either a low (35-45) or high (45-55) PCO2 target with the thought being that allowing for a higher pCO2 should mean that lower settings can be used. Lower settings on a ventilator would lead to less lung damage and therefore less CLD and in turn better outcomes. The study in question did show that the primary outcome was indeed different with almost a 75% reduction in days of ventilation and with that the era of permissive hypercapnia was born.
The Cochrane Weigh in
In 2001 a systematic review including this and another study concluded that there was insufficient evidence to support the strategy in terms of a benefit to death or chronic lung disease. Despite this lack of evidence and a recommendation from the Cochrane group that permissive hypercapnia be used only in the context of well designed trials the practice persisted and does so to this day in many places. A little lost in this discussion is that while the end point above was not different there may still be a benefit of shorter term ventilation.
A modern cohort
It would be unwise to ignore at this point that the babies of the late 90s are different that the ones in the current era. Surfactant and antenatal steroid use are much more prevalent now. Ventilation strategies have shifted to volume as opposed to pressure modes in many centres with a shift to early use of modalities such as high frequency ventilation to spare infants the potential harm of either baro or volutrauma. Back in 2015 the results of the PHELBI trial were reported Permissive hypercapnia in extremely low birthweight infants (PHELBI): a randomised controlled multicentre trial. This large trial of 359 patients randomized to a high or low target pCO2 again failed to show any difference in outcomes in terms of the big ones “death or BPD, mortality alone, ROP, or severe IVH”. What was interesting about this study was that they did not pick one unified target for pCO2 but rather set different targets as time went on reflecting that with time HCO3 rises so what matters more is maintaining a minimum pH rather than targeting a pCO2 alone which als0 reflects at least our own centre’s practice. There is a fly in the ointment here though and that is that the control group has a fault (at least in my eyes)
Day of life
Low Target
High Target
1-3
40-50
55-65
4-6
45-55
60-70
7-14
50-60
65-75
In the original studies of permissive hypercapnia the comparison was of a persistent attempt to keep normal pCO2 vs allowing the pCO2 to drift higher. Although I may get some argument on this point, what was done in this study was to compare two permissive hypercapnia ranges to each other. If it is generally accepted that a normal pCO2 is 35-45 mmHg then none of these ranges in the low target were that at all.
How did these babies do in the long run?
The two year follow-up for this study was published in the last month; Neurodevelopmental outcomes of extremely low birthweight infants randomised to different PCO2 targets: the PHELBI follow-up study. At the risk of sounding repetitive the results of Bayley III developmental testing found no benefit to developmental outcome. So what can we say? There is no difference between two strategies of permissive hypercapnia with one using a higher and the other a lower threshold for pCO2. It doesn’t however address the issue well of whether targeting a normal pCO2 is better or worse although the authors conclude that it is the short term outcomes of shorter number of days on ventilation that may matter the most.
The Truth is Out There
I want to believe that permissive hypercapnia makes a difference. I have been using the strategy for 15 or so years already and I would like to think it wasn’t poor strategy. I continue to think it makes sense but have to admit that the impact for the average baby is likely not what it once was. Except for the smallest of infants many babies these days born at 27 or more weeks of gestation due to the benefits of antenatal steroids, surfactant and modern ventilation techniques spend few hours to days on the ventilator. Meanwhile the number of factors such chorioamniotitis, early and late onset sepsis and genetic predisposition affect the risks for CLD to a great degree in the modern era. Not that they weren’t at play before but their influence in a period of more gentle ventilation may have a greater impact now. That so many factors contribute to the development of CLD the actual effect of permissive hypercapnia may in fact not be what it once was.
What is not disputed though is that the amount of time on a ventilator when needed is less when the strategy is used. Let us not discount the impact of that benefit as ask any parent if that outcome is of importance to them and you will have your answer.
So has permissive hypercapnia failed to deliver? The answer in terms of the long term outcomes that hospitals use to benchmark against one and other may be yes. The answer from the perspective of the baby and family and at least this Neonatologist is no.
A strange title perhaps but not when you consider that both are in much need of increasing muscle mass. Muscle takes protein to build and a global market exists in the adult world to achieve this goal. For the preterm infant human milk fortifiers provide added protein and when the amounts remain suboptimal there are either powdered or liquid protein fortifiers that can be added to the strategy to achieve growth. When it comes to the preterm infant we rely on nutritional science to guide us. How much is enough? The European Society For Pediatric Gastroenterology, Hepatology and Nutrition published recommendations in 2010 based on consensus and concluded:
“We therefore recommend aiming at 4.0 to 4.5 g/kg/day protein intake for infants up to 1000 g, and 3.5 to 4.0 g/kg/day for infants from 1000 to 1800 g that will meet the needs of most preterm infants. Protein intake can be reduced towards discharge if the infant’s growth pattern allows for this. The recommended range of protein intake is therefore 3.5 to 4.5 g/kg/day.”
These recommendations are from six years ago though and are based on evidence that preceded their working group so one would hope that the evidence still supports such practice. It may not be as concrete though as one would hope.
Let’s Jump To 2012
Miller et al published an RCT on the subject entitled Effect of increasing protein content of human milk fortifier on growth in preterm infants born at <31 wk gestation: a randomized controlled trial. This trial is quite relevant in that it involved 92 infants (mean GA 27-28 weeks and about 1000g on average at the start), 43 of whom received a standard amount of protein 3.6 g/kg/day vs 4.2 g/kg/d in the high protein group. This was commenced once fortification was started and carried through till discharge with energy intakes and volume of feeds being the same in both groups. The authors used a milk analyzer to ensure consistency in the total content of nutrition given the known variability in human milk nutritional content. The results didn’t show much to write home about. There were no differences in weight gain or any measurements but the weight at discharge was a little higher in the high protein group. The length of stay trended towards a higher number of days in the high protein group so that may account for some of the difference. All in all though 3.6 or 4.2 g/kg/d of protein didn’t seem to do much to enhance growth.
Now let’s jump to 2016
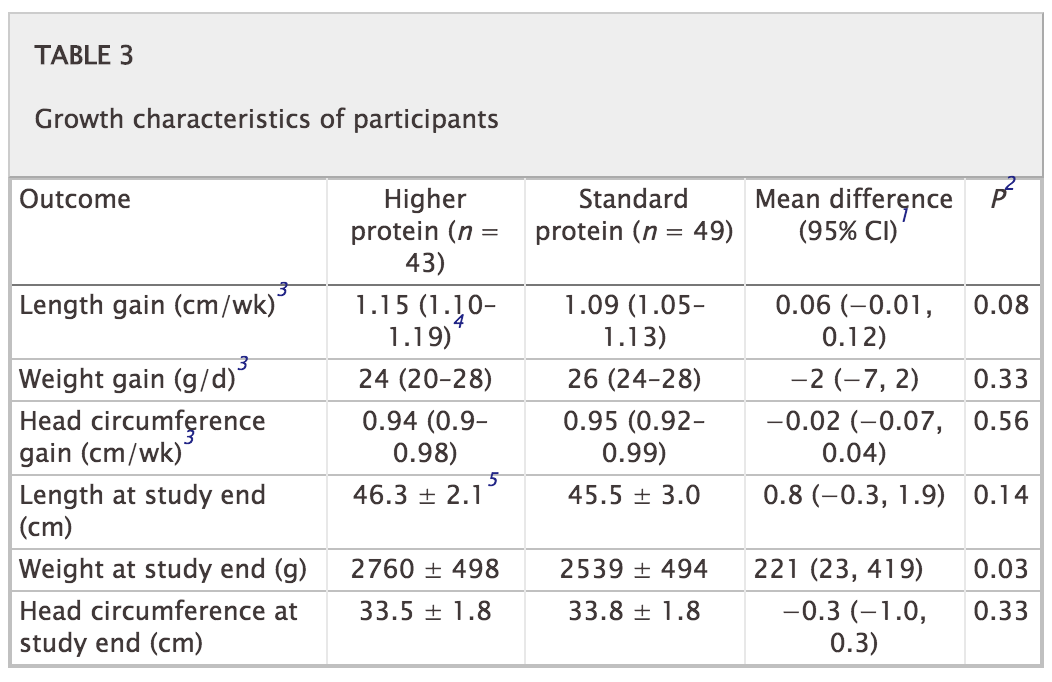
This past month Maas C et al published an interesting trial on protein supplementation entitled Effect of Increased Enteral Protein Intake on Growth in Human Milk-Fed Preterm Infants: A Randomized Clinical Trial. This modern day study had an interesting question to answer. How would growth compare if infants who were fed human milk were supplemented with one of three protein contents based on current recommendations. The first group of 30 infants all < 32 weeks received standard protein intake of 3.5 g/kg/d while the second group of 30 were given an average intake of 4.1 g/kg/d. The second group of 30 were divided though into an empiric group in which the protein content of maternal or donor milk was assumed to be a standard amount while the second 15 had their protein additive customized based on an analysis of the human milk being provided. Whether the higher intake group was estimated or customized resulted in no difference in protein intake on average although variability between infants in actual intake was reduced. Importantly, energy intake was no different between the high and low groups so if any difference in growth was found it would presumably be related to the added protein.
Does it make a difference?
The results of this study failed to show any benefit to head circumference, length or weight between the two groups. The authors in their discussion postulate that there is a ceiling effect when it comes to protein and I would tend to agree. There is no question that if one removes protein from the diet an infant cannot grow as they would begin to break down muscle to survive. At some point the minimum threshold is met and as one increases protein and energy intake desired growth rates ensue. What this study suggests though is that there comes a point where more protein does not equal more growth. It is possible to increase energy intakes further as well but then we run the risk of increasing adiposity in these patients.
I suppose it would be a good time to express what I am not saying! Protein is needed for the growing preterm infant so I am not jumping on the bandwagon of suggesting that we should question the use of protein fortification. I believe though that the “ceiling” for protein use lies somewhere between 3.5 – 4 g/kg/d of protein intake. We don’t really know if it is at 3.5, 3.7, 3.8 or 3.9 but it likely is sitting somewhere in those numbers. It seems reasonable to me to aim for this range but follow urea (something outside of renal failure I have personally not paid much attention to). If the urea begins rising at a higher protein intake approaching 4 g/kg/d perhaps that is the bodies way of saying enough!
Lastly this study also raises a question in my mind about the utility of milk analyzers. At least for protein content knowing precisely how much is in breastmilk may not be that important in the end. Then again that raises the whole question of the accuracy of such devices but I imagine that could be the source of a post for another day.
It’s World Prematurity Day today and if you are a parent or are caring for a baby who has just entered this world before 37 weeks GA you are now part of a membership that counts 15 million new babies each year according to the WHO’s data. As I tell most new parents who have a baby admitted to our unit “It’s ok to take some time to adjust to this. You didn’t plan on being here”. That is true for most who go into spontaneous labour but of course those who are electively delivered due to maternal or fetal indications that have been followed closely often have time to prepare for the journey to the NICU. Many of these parents will have had the opportunity to visit the NICU or even connect with other parents before the anticipated birth of their child to at least get a glimpse into what life is like in the NICU. Much has been written about parental stress and methods to reduce it and I find that a piece that appeared in the Huffington Post offers some good pointers to helping parents manage the transition from pregnancy to NICU. The piece is entitled 5 Things Never To Say To Parents Of Preemies (And What To Say Instead).It is well worth a read but the one thing that stuck out in my mind is one very important thing to say.
Congratulations on the birth of your baby
There is no doubt that the family who gives birth to a preterm infant is experiencing stress. What may be lost in the first few days of surfactant, central lines and looking for sepsis among other things is that a new member of the 15 million strong has entered this world. They have a new child and just like anyone else should receive a congratulations. No one needs to tell them to be worried. They already are and likely view many of the possibilities more pessimistically than you do. Taking a moment to say congratulations though may go a long way to reminding them that amidst all this stress there is something to rejoice in and look to the future. If we aren’t supportive then I have no doubt the subconscious message is that they shouldn’t have hope either. I am not suggesting that we sugarcoat what is really going on but one can be honest about likely outcomes and still celebrate the arrival of a new baby. Much has also been written recently about a number of strategies to reduce stress in the NICU such as skin to skin care, integration of families more closely into the patient care team and forming parent support groups just to name a few. What else can be done to improve the quality of life for parents going through this journey?
Enrol Your Baby In A Research Study
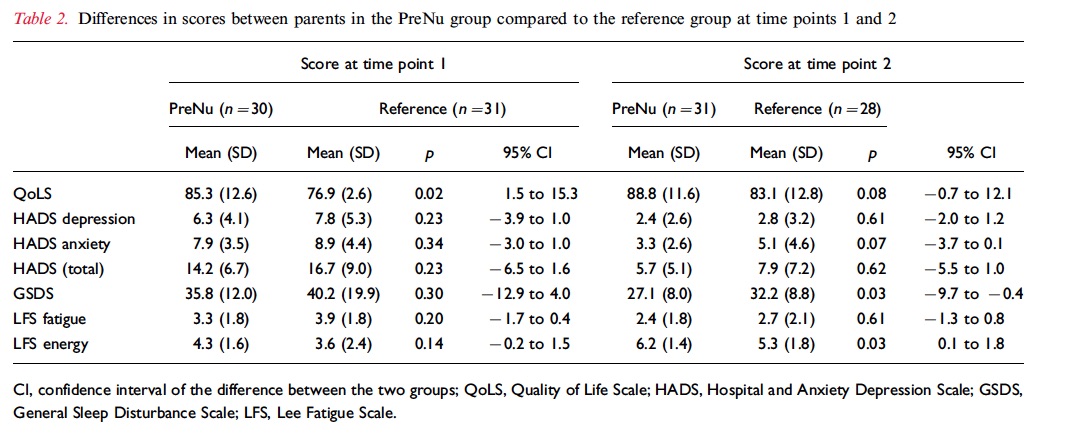
I work in an academic centre and given the volume of research projects at any given time there is a need to approach families and sometimes quite soon after delivery. interestingly, I have heard from time to time that individuals have been hesitant to approach families due to a feeling that they are overwhelmed and won’t be receptive to being approached in this fragile state. I am guilty of the same thoughts from time to time but maybe it is time I reconsider. Nordheim T et al just published an interesting study on this topic entitled Quality of life in parents of preterm infants in a randomized nutritional intervention trial. This study was actually a study of parents within a study that called the PreNu trial that involved an intervention of a energy and protein supplemental strategy to enhance weight at discharge. The trial was an RCT and unfortunately although well intentioned was stopped when the intervention group was found to have an unexpected increase in sepsis rates. Although this study did not ultimately find a positive outcome there were additional analyses performed of quality of life and parental stress at two time points the first being during the hospital stay and the second at 3.5 years of age. The patients were all treated the same aside from the nutritional intake and in the end 30 intervention parents and 31 single parents not enrolled in a study (many in couples) participated in the study. In followup a little less than 70% completed the stress measures at 3.5 years. The results are found below.
How Do We Interpret This
The parents in this study who were part of the intervention group were about 3 years older so perhaps with more life experience may have developed some better coping strategies but during the hospital stay those who participated in research had better measures of quality of life and at three years better reports of sleep and energy levels. The study is quite small so we need to take all of this with a grain of salt with respect to the 3.5 year outcomes as there are so many variables that could happen along the way to explain this difference but I think it may be fair to acknowledge the quality of life measure during the stay. Why might parents report these findings? The finding of better quality of life is especially interesting given that more patients in this study had sepsis which one would think would make for a worse result. Here are a few thoughts.
Involvement in research may have increased their knowledge base as they learned about nutrition and expected weight gain in the NICU.
Frequent interaction with researchers may have given them more attention and with it more education.
Some parents may have simply felt better about knowing they were helping others who would come after them. I have heard this comment myself many times and suspect that it would be attributable at least to a certain extent.
A better understanding of the issues facing their infants through education may have reduced stress levels due to avoiding “fear of the unknown”.
Regardless of the exact reason behind the findings what stands out in my mind is that participation in research likely provides comfort for parents who are in the midst of tremendous stress. Is it the altruistic desire to help others or being able to find something good in the face of a guarded outlook? I don’t know but I do believe that what this study tells us is that we shouldn’t be afraid to approach families.
After first congratulating them give them a little time to absorb their new reality and then offer them the chance to improve the care for the next 15 million that will come this time next year for World Prematurity Day 2017.
This is a title that I hope caught your eye. In the nearly twenty years I have been in the field of Pediatrics the topic of parking being a barrier to parental visitation has come up again and again. A few years ago the concern about the cost of parking was so great that I was asked if I could find a pool of donors to purchase parking passes to offset the burden to the family. The theory of course is based on the idea that if parking were free in the NICU parents would visit more. If parents visit more they will be more involved in the care of their baby, more likely to breastfeed and with both of these situations in play the infant should be discharged earlier than other infants whose parents don’t visit. Try as I might it was a tough sell for donors who tend to prefer buying something more tangible that may bear their name or at least something they can look at and say “I bought that”. This is quite tough when it comes to a parking stall and as such I am still looking for that elusive donor. Having said that, is there any basis to believe that free parking is the solution that will deliver us from minimal visitation by some parents?
A Study May Help Answer The Question
Northrup TF et al published an article that was sent my way and to be honest I couldn’t wait to read it. A freeparking trial to increase visitation and improve extremely low birth weight infant outcomes. This is like the holy grail of studies. A study that gets right to the point and attempts to answer the exact question I and others have been asking for some time. The study took place in Houston, Texas and was set up as an RCT in which families were randomized into two groups. Inclusion criteria were birth weight ⩽1000 g, age 7 to 14 days and deemed likely to survive. Seventy two patients were enrolled in the free parking group while 66 were placed in the usual care. Interestingly the power calculation determined that they would need 140 to show a difference so while 138 is close it wasn’t enough to truly show a difference but let’s see what they found.
The Results
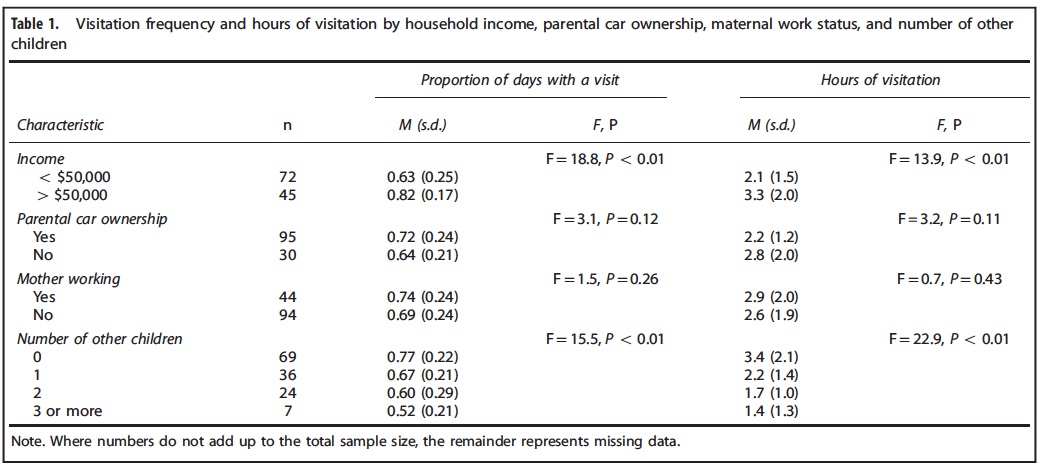
Free parking made absolutely no difference for the whole group. Specifically there was no difference in the primary outcome of length of stay or hours spent per visit. Some interesting information though that may not be that surprising was found to be of importance in the table below.
It may not seem like a surprise but the patients who were more affluent and those who had less children tended to visit more. The latter makes a lot of sense as what are many people to do when they have one or more other children to care for at home especially in the face of little support? Would free parking make one iota of difference if the barrier has nothing to do with the out of pocket cost?
The conclusion was that the strategy didn’t work that well but as you may have picked up I think the study was flawed. By applying the strategy to all they were perhaps affected by choosing the wrong inclusion criteria. Taken to an extreme, would a 50 million dollar Powerball winner care one bit about parking vouchers? It wouldn’t make any difference to whether they were going to come or not. Similarly a single mother with 5 other kids who lives below the poverty line and has little support is not going to come more frequently whether they have a voucher or not.
What if the study were redone?
I see a need to redo this study again but with different parameters. What if you randomized people with a car or access to one who lived below a certain income level and had a committed support person who could assure that team that they could care for any other children the family had when called upon? Or one could look at families with no other children and see if offering free parking led to more frequent visitation and then from there higher rates of Kangaroo Care and breastfeeding. I for one haven’t given up on the idea and while I was truly excited to be sent this article and sadly initially dismayed on first read, I am hopeful that this story has not seen it’s end.
It is intuitive to me that for some parents parking is a barrier to visiting. Finding the right population to prove this though is the key to providing the evidence to arm our teams with evidence to gain support from hospital administrations. Without it we truly face an uphill battle to get this type of support for families. Stay tuned…
I had a chance recently to drive a Tesla Model S with autopilot. Taking the car out on a fairly deserted road near my home I flicked the lever twice to activate the autopilot feature and put my hands behind my head while the vehicle took me where I wanted to go. As I cruised down the road with the wheel automatically turning with the curves in the road and the car speeding up or slowing down based on traffic and speed limit notices I couldn’t help but think of how such technology could be applied to medicine. How far away could the self driving ventilator or CPAP device be from development?
I have written about automatic saturation adjustments in a previous post but this referred to those patients on mechanical ventilation. Automatic adjustments of FiO2. Ready for prime time? Why is this goal so important to attain? The reasoning lies in the current design trends in modern NICUs. We are in the middle of a large movement towards single patient room NICUs which have many benefits such as privacy which may lead to enhanced breastfeeding rates and increased parental visitation. The downside, having spoken to people in centres where such designs are already in place is the challenge nursing faces when given multiple assignments of babies on O2. If you have to go from room to room and a baby is known to be labile in their O2 saturations it is human nature to turn the O2 up a little more than you otherwise would to give yourself a “cushion” while you are out of the room. I really don’t fault people in this circumstance but it does pose the question as to whether in a few years we will see a rise in oxygen related tissue injury such as CLD or ROP from such practice. In the previous post I wrote about babies who are ventilated but these infants will often be one to one nursed so the tendency to overshoot the O2 requirements may be less than the baby on non- invasive ventilation.
A System For Controlling O2 Automatically For Infants on Non-Invasive Ventilation
The study was really a proof of concept with 20 preterm infants (mean GA 27.5 weeks, 8 days of age on average) included who each underwent two hours of manual control by nursing to keep saturations between 90-94% and then 4 hours of automated control (sats 91 – 95%) then back to manual for two hours. The slightly shifted ranges were required due to the way in which midpoint saturations are calculated. The essential setup was a computer equipped with an algorithm to make adjustments in FiO2 using an output to a motor that would adjust the O2 blender and then feedback from an O2 saturation monitor back to the computer. The system was equipped with an override to allow nursing to adjust in the event of poor signal or lack of response to the automatic adjustment.
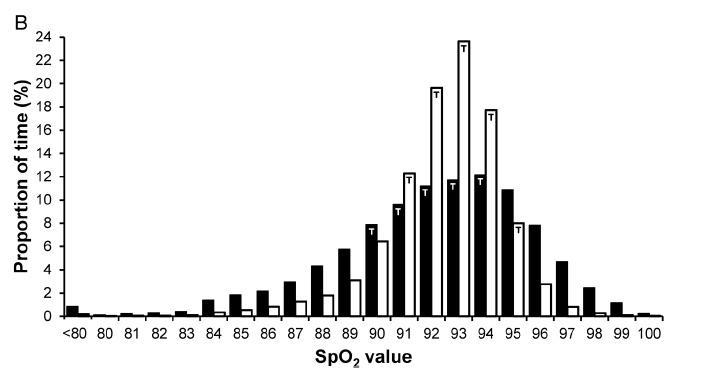
The results though demonstrate that the system works and moreover does a very good job! The average percentage of time that the saturations were in the target range were significantly better with automated control (81% automated, 56% manual). As well as depicted in the following figure the amount of time spent in both hypoxic and hyperoxic ranges was considerable with manual control but non-existent on either tail with automated control (defined as < 85% or > 98% where black bars are manual control and white automatic).
From the figure you can see that the amount of time the patients are in target range are much higher with automatic control but is this simply because in addition to automatic control, nurses are “grabbing the wheel” and augmenting the system here? Not at all.
“During manual control epochs, FiO2 adjustments of at least 1% were made 2.3 (1.3–3.4) times/hour by bedside staff. During automated control, the minimum alteration to FiO2 of 0.5% was being actuated by the servomotor frequently (9.9 alterations/min overall), and changes to measured FiO2 of at least 1% occurred at a frequency of 64 (49–98) /hour. When in automated control, a total of 18 manual adjustments were made in all 20 recordings (0.24 adjustments/hour), a reduction by 90% from the rate of manual adjustments observed during manual control (2.3/hour).”
From the above quote from the paper it is clear that automated control works to keep the saturation goal through roughly 7 X the number of adjustments than nursing makes per hour. It is hard to keep up with that pace when you have multiple assignments but that is what you need I suppose! The use of the auto setting here reduced the amount of nursing interventions to adjust FiO2 by 90% and yields tighter control of O2 saturations.
Dare to Dream
Self driving oxygen administration is coming and this proof of concept needs to be developed and soon into a commercial solution. The risk of O2 damage to developing tissues is too great not to bring this technology forward to the masses. As we prepare to move into a new institution I sincerely hope that this solution arrives in time but regardless I know our nurses and RRTs will do their best as they always do until such a device comes along. When it does imagine all of the time that could be devoted to other areas of care once you were able to move away from the non-invasive device!

 The importance of collaborating in a respectful manner cannot be overemphasized, as a calm and well prepared team can handle just about anything thrown their way. This past week I finally had the opportunity to take the 7th ed NRP instructor course. What struck me most about the new version of the course was not the approach to the actual resuscitation but the preparation that was emphasized before you even start! It only takes 30 seconds to establish who is doing what in a resuscitation and while it would seem logical to divide up the roles each will take on it is something that has not been consistently done (at least in our institution). When a baby is born and responds to PPV quickly, this may not seem that important but in a situation where a team is performing chest compressions, placing an emergency UVC and moving on to epinephrine administration it certainly is nice to know in advance who is doing what.
The importance of collaborating in a respectful manner cannot be overemphasized, as a calm and well prepared team can handle just about anything thrown their way. This past week I finally had the opportunity to take the 7th ed NRP instructor course. What struck me most about the new version of the course was not the approach to the actual resuscitation but the preparation that was emphasized before you even start! It only takes 30 seconds to establish who is doing what in a resuscitation and while it would seem logical to divide up the roles each will take on it is something that has not been consistently done (at least in our institution). When a baby is born and responds to PPV quickly, this may not seem that important but in a situation where a team is performing chest compressions, placing an emergency UVC and moving on to epinephrine administration it certainly is nice to know in advance who is doing what.




 As I cruised down the road with the wheel automatically turning with the curves in the road and the car speeding up or slowing down based on traffic and speed limit notices I couldn’t help but think of how such technology could be applied to medicine. How far away could the self driving ventilator or CPAP device be from development?
As I cruised down the road with the wheel automatically turning with the curves in the road and the car speeding up or slowing down based on traffic and speed limit notices I couldn’t help but think of how such technology could be applied to medicine. How far away could the self driving ventilator or CPAP device be from development?