
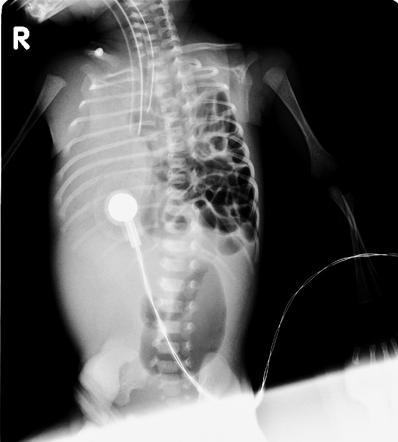
For as long as I can remember I was taught that there is a desperate need to intubate babies with congenital diaphragmatic hernia right after birth and place an NG to suction. The goal of this manouver was to minimize the amount of swallowed air into the GI tract and thereby give our best chance at ventilation. If there was a dogma in Neonatology this had to be one right near the top. In fact, attending the delivery of a baby with a known CDH has been ike watching a well trained SWAT team in action with everyone committed to their roles and importantly getting that ETT in as fast as possible being the first goal. Once the tube is in though we often have the problem of having a vigorous term infant who needs a fair bit of sedation to keep the tube in. Moreover, they don’t want to be intubated so keeping them settled may require significant doses of opiates and or benzodiazepines which in turn may wreak havoc with their hemodynamics and require pressor support. Not a great start to life.
Another Way?
There is a subset of patients with CDH who are said to have “mild CDH” Their characteristics are that they have an isolated leftsided CDH with an observed-to-expected lung to-head ratio (O/E LHR) greater than or equal to 50%, and
intraabdominal liver position. The survival for this group exceeds 95%.
Researchers from the Netherlands published last year Routine Intubation in Newborns With Congenital Diaphragmatic Hernia. In the paper they make the argument that there could be another way to handle such babies whcih they call the spontaneous breathing approach or SBA. Basically, a team approach with perinatology is used to identify these lower risk fetuses with CDH and then at birth the following approach is used as per the paper.
“The newborn is positioned on the resuscitation table and a Replogle tube (10F catheter) is inserted for continuous stomach decompression. In the case of planned SBA, the infant is supported with oxygen if necessary (Neopuff infant T-piece resuscitator; Fisher & Paykel Healthcare, Ltd, Auckland, New Zealand), aiming for preductal saturations .85%.4
Continuous positive airway pressure isallowed. The infant is intubated if insufflation breaths or ventilation are
needed because positive pressure ventilation via mask increases the air in the digestive tract, subsequently
compressing the lungs, resulting in hypoxia and PH.”
They Tried it Out
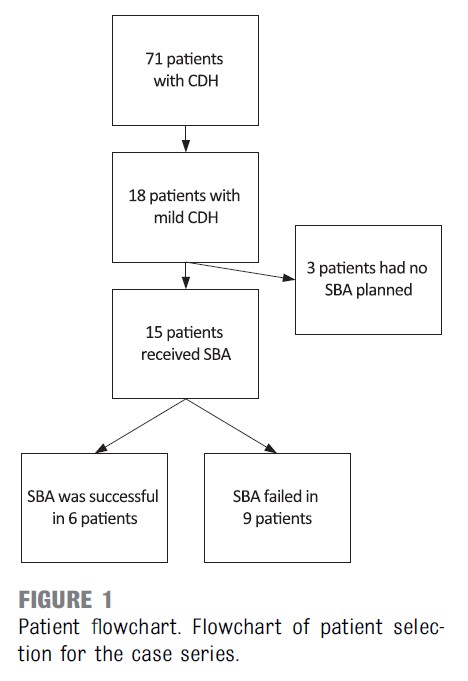
Armed with this approach the authors performed a retrospective study to determine whether the approach above is a reasonable one to take based on their own experience. Looking at the figure below over about a 5 year period they had 71 patients with CDH. Eighteen met their criteria for low risk and 15 of those had a planned SBA. Of the 15, SBA was successful (meaning they did not require intubation prior to surgery) in 6 or 40% while the other 60% did not tolerate the approach.
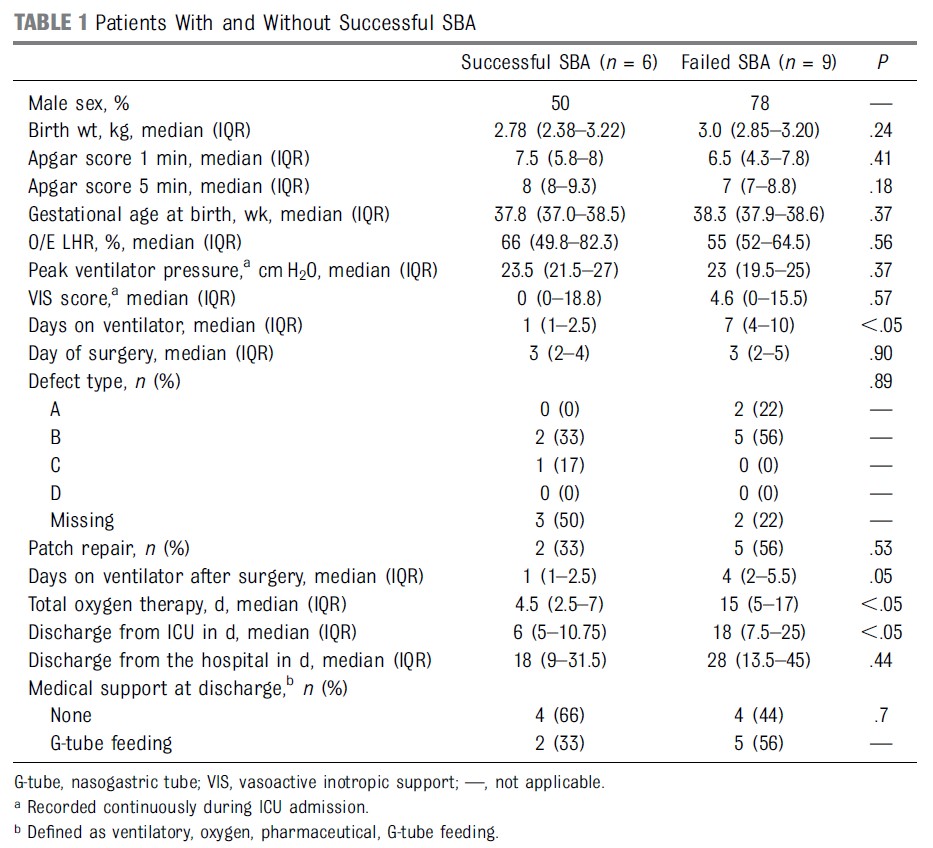
Looking at characteristics of those who were successful vs not was presented in table 1 below. There were no baseline characteristics that stood out to indicate higher or lower likelihood of success but it is clear that not having success has an impact. Those who did not tolerate the SBA had longer durations of ventilation and length of stay. This is an association but I would imagine the increased durations have more to do with the fact that the infants were sicker than expected rather than anything else.
What Can We Say About It?
I think there are a number of interesting aspects to this approach. The first is that the old dogma of saying that all these infants need to be intubated to prevent intestinal distension is incorrect. Secondly, the use of CPAP as long as there was gastric suction did not impact these infants to any signicant degree. The survival of this group regardless of tolerance or failure of the SBA was 100% and only one patient needed iNO therapy with an LHR of 57%. Of course the numbers here are small so I am not suggesting for a moment that this clearly is the way to go. It does provide strong support though for a prospective trial that I understand is in the works. In the meantime what do we do with the babies that are to come? For the most part I think units need to decide as a group what approach they are willing to take with these low risk patients. It will cause great confusion for staff if one week a baby is put on CPAP and the next with a similar risk profile a baby is urgently intubated. Lastly let me say that I love that something I was taught 25 years ago to ALWAYS do is now being questioned. What’s next?