I recall the shock waves through the neonatal community when ILCOR changed its recommendation to stop routine intubation of non-vigorous infants born through meconium. The rationale again was that for most practitioners it would be better to give bag valve mask ventilation and establish a functional residual capacity than try and intubate and start with a collapsed lung.
Oommen VI et al wrote a brief report on their experience in the UK with the change as recommended for these infants. Their brief publication has a large cohort that is looked at and one result in particular I found interesting enough to share with you today. The publication is Resuscitation of non-vigorous neonates born through meconium-stained amniotic fluid: post policy change impact analysis. The authors looked prospectively at the “new approach” group from October 2016-September 2017 and compared their outcomes to the retrospecitve cohort in the same hospital from August 2015-July 2016 as the “old approach” group.
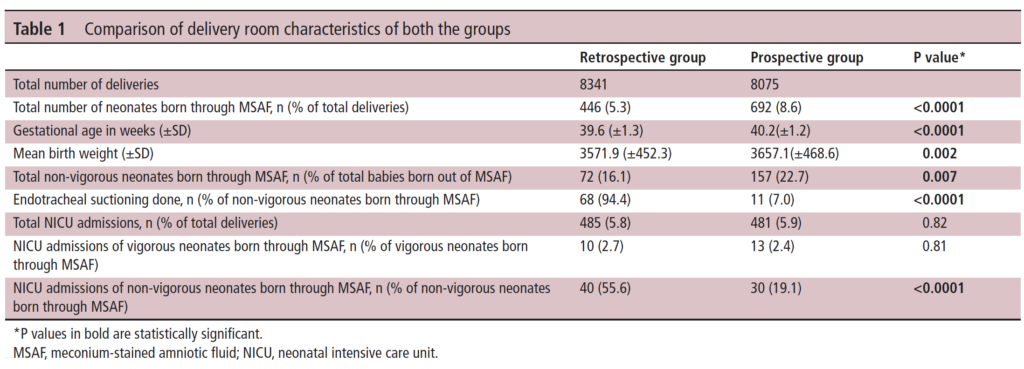
As you can see in Table 1 they saw a lot of deliveries during this time that were complicated by meconium. This gives us a good before and after comparison and while not all prospective and ensuring that practices were otherwise the same it is a pretty decent sample to look at. I like seeing that 7% of the group in the new approach still received endotracheal suctioning. It is worth remembering that what the recommendation says is to not do this routinely but if the resuscitation is not going well and the baby not responding to ventilation it is reasonable to apply suctioning as they would have done to see if there is any obstructive material in the airway.
It is the last comparison in Table 1 though that drew my attention. Over 50% of the non-vigorous babies needing routine suctioning in the retrospective arm needed NICU admission compared to 19.1% of the new approach group which was quite significant. More on this later.
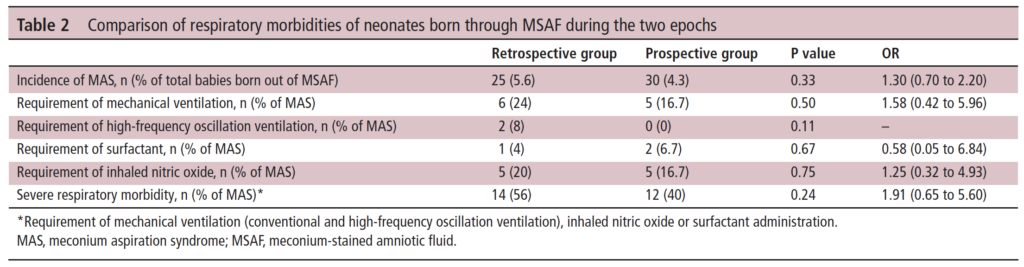
In Table 2 the authors compare the respiratory morbidities showing no difference in rates of ventilation, HFOV, surfactant or iNO. What they are demonstrating is that to the best of their abilities the babies were similar in terms of respiratory morbidiites in a binary sense. What I mean here is that when you ask the question did they need any of these aforementioned things it is a yes or no. What is not easy to pick up from the table is the quality of the respiratory disease. In the table they make it clear that severe respiratory disease was the same at 56% pre and 40% post and of course all of these babies would have needed admission. What we don’t know is what happened to the mild to moderate group.
A Theory
The whole point of giving PPV for the non-vigorous infant is to establish FRC. In the old approach it is conceivable that some of the infants could have lost volume during attempted intubation. The resultant delay in oxygenation could exacerabate any tendency to pulmonary hypertension. It could also turn a baby from one that could have had mild grunting to one that needed CPAP. Put another way it could have changed the outcome from a baby that needed observation and some prone positioning for a few hours to one that is committed to admission.
What these results show is basically what the intent of doing away with routine suctioning was supposed to do. The vast majority of severe disease in meconium aspiration syndrome is acquired in-utreo. Hypoxia and acidosis contribute to pulmonary hypertension while gasping respirations lead to inhalation of meconium deep into the airways. Suctioning after birth is not really going to help this cohort much. Providing positive pressure ventilation to the more mildly affected infants however may help open their lungs whereas delays in initiating would have the opposite effect.
In the end routine suctioning was a dogma that was in need of a challenge. The authors in the body of the paper go through other similar studies and in all but one the findings are similar. I commend the authors here for their humility as they do add at the end of the report all the potential shortcomings of the research. I for one don’t think it was necessary, as well designed research and thought went into taking down the dogma of routine suctioning. There is complete biological plausability for the findings presented here and I for one am glad to see that research in this case informed practice change that I believe was for the better.
As awful as COVID19 has been over the last year and a half one thing has continued to perplex myself and others. Why do babies whethe term or preterm so rarely acquire the virus? Numerous studies have been able to document placental changes and infection of these tissues. On rare occasions reports have come out with evidence of neonatal infection but fortunately most are mild.
These findings have in large part contributed to the Canadian Pediatric Society practice points on three topics.
In this post an argument was made that the reason these infants are resistant is due to low levels of ACE-2 receptors in the nasal mucosa of children. In this study children as young as 4 years of age were found to have very low levels of this receptor (portal of entry for SARS-CoV-2) into the host. I speculated at the time that if one carried forward the findings to younger children and infants you might find there were hardly any receptors at all.
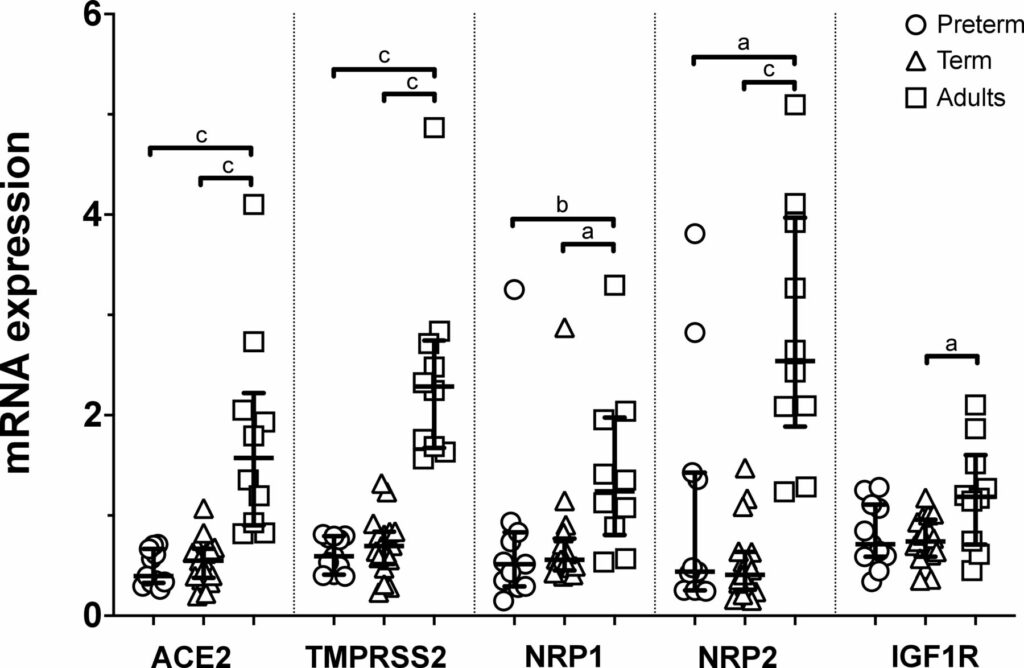
Well, someone finally did the study and confirmed what I suspected. The study report is entitled Nasal expression of SARS-CoV-2 entry receptors in newborns by Heinonen S et al. It’s not a big study but the results are consistent across 28 newborns (17 term and 11 preterm) and 10 adults. In each newborn whether term or preterm a nasal mucosal scraping was performed at 24 hours of age and used to measure by reverse-transcription quantitative PCR mRNA expression of ACE2, transmembrane serine protease 2 (TMPRSS2), neuropilin 1 (NRP1) and neuropilin 2 (NRP2) and insulin-like growth factor 1 receptor (IGF1R).
What the results show you is that babies are not just small adults. They are different yet preterm do not seem to be that different than term infants in terms of receptors. While ACE2 has garnered most of the attention when it comes to receptors for SARS-CoV-2 the others also play a role and are in general expressed to a lesser degree in neonates than adults.
Conclusions
In the previous post I argued what was in your nose makes a difference to your risk of contracting SARS-CoV-2. Really the point is what is not in your nose. Thankfully neonates do not have good expression of these receptors and that may be the biggest reason for the general protection they have from this pandemic. It has certainly a good time to be in the “have not” group!
A couple years back at the Canadian Pediatric Society annual meeting a discussion broke out about extubating infants to higher levels of CPAP. Conventional thinking had been to use levels between 5 – 8 cm H2O typically. I shared with the group the experience we had in Winnipeg (unpublished) of using higher levels from 9 -12 cm H2O with some degree of success in allowing earlier extubation. The group thought it was interesting but pointed out the lack of robust research in the area so were not so keen to “try it out”. Non-invasive positive pressure ventilation (NIPPV) has been used for some time in the neonatal world and has been compared to CPAP for extubation success and found to be superior as in this review Comparison of Complications and Efficacy of NIPPV and Nasal CPAP in Preterm Infants With RDS. In this review though as in others more typical CPAP levels are used so the question is whether the same efficacy would be seen with high level CPAP vs NIPPV.
Canadian Study to the Rescue
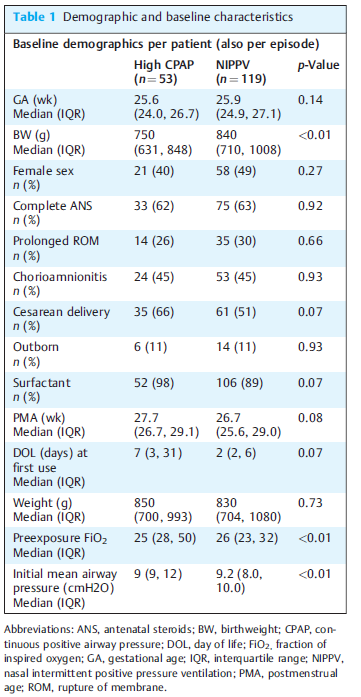
The study here is by Ahmad HA et al Comparison of High CPAP versus NIPPV in Preterm Neonates: A Retrospective Cohort Study and seeks to answer this question albeit in a retrospective fashion. The study is not well controlled since it is retrospective but it may be the best we have for now. Over a 3 year period the authors examined the outcomes for babies trialed on high CPAP (hCPAP of at least 9 cm H20) vs NIPPV. In each case they looked at the first episode of use. The modalities could have been used for extubation or as a primary means of support. The primary outcome was failure of the modality as defined by either intubation or change to the other strategy within 7 days. A total of 53 infants received hCPAP vs 119 NIPPV. Why the big difference? Since this was retrospective and not randomized it was up to the individual practioner which modality they wanted to try. If the majority of the unit favoured NIPPV this is why there would be such a difference. Herein lies the benefit of the primary outcome as if “conventional wisdom” was wrong and the other modality would be better then we should see a greater movement to the other strategy or more intubations in one group suggesting superiority of one vs the other.
The groups however aren’t entirely equivalent at baseline. The babies in the hCPAP group are quite a bit smaller on the one hand which would favour the NIPPV group. On the other hand there is almost a significant difference in surfactant provision for the hCPAP arm which might favour the hCPAP group. The other thing also nearing statistical significance is when the intervention was trialed. The median time is 2 days for teh NIPPV group and 7 for hCPAP suggesting one may have been used more prophylactically and the other post extubation. Different strategies might make a difference to outcome? Also no infants received MIST or INSURE and all were started on traditional lower levels of CPAP prior to surfactant.
Results
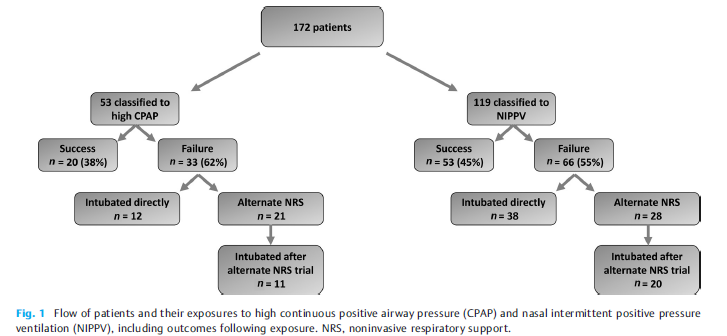
The results tell an interesting story (I think) with the primary outcome being no different 62% in the hCPAP vs 55% with NIPPV. Looking at the patient outcomes in the figure from the paper one gets a little more detail and can surmise how people viewed the two modalities as a strategy and can see they were a bit different.
There seems to have more confidence in the unit with NIPPV as a way to prevent intubation. For those that failed hCPAP 12/33 were intubated as the next step (about a third) while the other 2/3 were trialed on NIPPV. Looking at those started out on NIPPV, 38/66 were intubated directly 58% or almost 2/3 while 28/66 were trialed on hCPAP. Of the ones trialed on hCPAP 20/28 or 71% were still intubated. Comparatively of those who were changed from nCPAP to NIPPV 11/21 were intubated or about 50%.
The authors find no difference in the primary outcome which is true. The problem of course with this analysis though is that there was no standardization with determining when one would choose to intubate. This issue can really play with the results. Let’s say for example that one Neonatologist really believes for the most part that NIPPV is the mode that can really prevent intubation more than hCPAP. It is conceivable that the reason in crossover intubations are less with NIPPV is that people were willing to tolerate a slightly higher pCO2 or a couple more apneas since they believe the modality is best and the infant will “get better soon”. On the other hand, infants already on NIPPV who are deteriorating might be intubated more readily as the attending might think “this hCPAP is a bunch of malarky”
It is worth mentioning that the incidence of air leak was no different between the two, nor was NEC or feeding intolerance from exposing the babies to such high pressures.
Conclusions
The study doesn’t “prove” anything. I don’t see it as a complete waste though as it does a number of things. It does show that small infants can be managed with hCPAP in NICU without any significant increase in complications. It also sets the stage for a couple future prospective trials I can see. Firstly, a trial of traditional CPAP vs hCPAP is needed as some units don’t have access to NIPPV or simply don’t use. The second is a prospective trial with clear parameters for failure between hCPAP and NIPPV. Lastly, the authors ran the NIPPV and CPAP off ventilators in the units. The work of breathing would be potentially different with the use of devices solely designed for CPAP with fluidic flips. It would be important to use optimal devices for both modalities in such a trial and I for one can’t wait to see them.
In medicine we learn a lot through feedback from our learners. The same prinicple I think can apply here on this blog. When I post a new blog post there are a few ways that it is shared. If you subscribe to this blog then you get a direct email about it. Others see the posts advertised on Facebook and Twitter or Linkedin and access the content from there. When you come through the latter route I am able to see that data and get a sense of whether a topic is of more or less interest to the readers as wordpress provides helpful statistics in this regard such as this from today.
When you access the post by reading the email version this view is not counted in the statistics. As of today there are 1745 of you registered to receive emails with each new post! What I am looking for today is for you to take this very quick poll and help me better understand where views are coming from.
My goal on the blog of course is to try and find interesting concepts and studies to share with you and it would be very helpful to know in particular about email readership.
Thanks in advance and I hope you continue to enjoy the content!