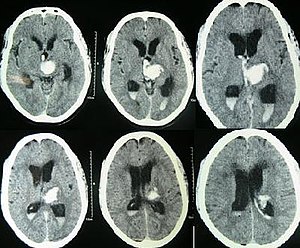
Sometime between a week to two weeks you will hear that an ultrasound of your baby’s brain has been ordered. What the team is looking for here is bleeding eithre within the fluid filled chambers of the ventricles (appear black in the picture below with blood that shows up as white). This early ultrasound is meant to pick up this type of injury while one done a few weeks later attempts to pick something else up.
Bleeding occurs due to the fragile naure of the brain tissue when born preterm. The more preterm an infant is the greater the risk of a signficant amount of bleeding. Bleeding tends to occur from an area of the brain just under the lining of the fluid filled ventricles that has a very rich blood supply. Anything that causes fluctuations in blood flow to this area of the brain can lead to injury and bleeding from this site. Blood in the ventricles of the brain is referred to as an Intraventricular hemorrhage or IVH for short.
Classically you will hear the team discuss the results of your baby’s head ultrasounds as having one of five possible categories.
No IVH
Grade 1 IVH – blood just under the lining of the ventricle
Grade 2 IVH – blood has gotten into the ventricle but is not causing it to get signiicantly enlarged
Grade 3 IVH – blood has entered the ventricle and is causing the chamber to grow as fluid that normally drains out is getting blocked by blood from leaving. As fluid (cerebral spinal fluid) continues to be produced, if it has trouble draining out it is like a kitchen sink with the tap turned on and something blocking the drain)
Grade 4 IVH – this is actually a bit different and is blood within the tissues of the brain outside of the ventricles. This is caused by blood flow in the veins of the brain being too slow and then causing vessels to rupture from lack of flow and oxygen.
A grade 3 IVH is shown below with the chambers swelling (black).
What can happen if the bleeding is significant?
It is the Grade 3 and 4 bleeds that we really worry about. The grade 1 bleeds tend to resolve on their own. When we see a bleed you can expect to see a new ultrasound be done in 1-2 weeks to folllow up and make sure it doesn’t get worse. If a grade 3 bleed continues to cause the ventricles to increase in size we worry with time that this may put pressure on the brain and affect the amount of blood flow the brain receives. If this is happening you may hear that we are asking Neurosurgery to see your infant. They will work with us to determine whether your baby needs a drain put into the ventricle to help get rid of the excess fluid. Many times the ventricles as we watch them with additional ultrasounds get smaller with time but some do not and will need this plastic drain put in to allow the brain to have this pressure relieved.
With the Grade 4 bleeds with time the body will absorb this damaged tissue and your baby may be left with a hole in the brain where the injured tissue was. While this sounds frightening the ability of our ultrasounds to predict eventual outcome is not great. Such infants though will generally be followed in a high risk follow up clinic and carefully monitored for their development. If they are found to have any deficits, depending on your location a variety of services may be offered to help optimize the best chance for a good outcome. Such services might include involvement of an occupational therapist or physiotherapist.
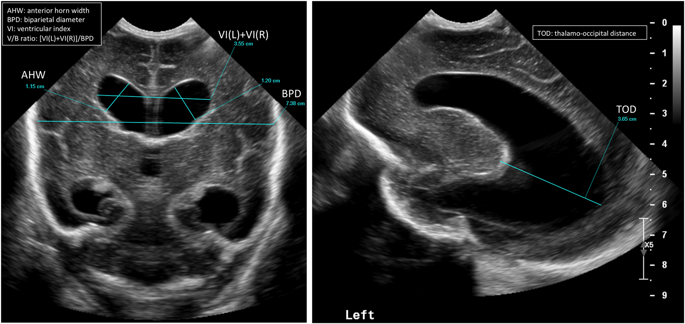
Late Ultrasounds
Sometime between about 4-6 weeks after birth or in some cases near discharge another ultrasound will be done. This time the team is looking for something different. The risk of fresh bleeding has passed but now we are looking for evidene of a lack of blood supply at some point from the arteries that provide blood supply to the brain. Many weeks after being born if there has been a period of significant impairment of blood flow to the brain we may see evidence of this. The brain has both white and gray matter (tissue). The gray matter is all along the surface of the brain. Underneath though and right next to the ventricles is the white mattter. This white matter is where the injury we are looking for may have occurrred. We call this injury periventricular leukomalacia. This means injury to the white matter. The white matter is where our neurological tissue for motor function travels so in these infants with such injury there can be problems with normal movement in the legs usually, moreso than the arms. Assessments in babies with such injury may find increases in the muscle tone in the NICU. In such cases, referral to a physiotherapist early to teach families how to do stretching exercises as an example will be done. Similarly, positioning devices from an occupational therapist may also be recommended.
Delayed cord clamping has been written about before on this blog. In fact between the blog and facebook posts I think it has been discussed many times. What hasn’t really been touched upon whether one type of cord management is superior to another. Is delayed cord clamping equivalent to cord milking or is one better than the other? The answer is a complicated one as you first need to define what both are. For delayed cord clamping it could be as short as 3 minutes and as long as 5 minutes or so as was seen in the post on physiological based cord clamping. For cord milking I suppose the definition is a little less broad but typically involves stripping of the cord after allowing the cord to fill with placental blood to enhance flow over a shorter time than DCC from the placenta to the newborn.
A Head to Head Comparison
Katheria A et al published Association of Umbilical Cord Milking vs Delayed Umbilical Cord Clamping With Death or Severe Intraventricular Hemorrhage Among Preterm Infants this past month in JAMA. The authors compared two well defined approaches to care after delivery. Delayed cord clamping was defined as being at least 60 seconds (mean time was about that) while cord milking was done by using 20 cm of the umbilical cord and milking for 2 seconds allowing refill, and then repeating 3 more times. The primary outcome under study was the incidence of death or severe IVH at 6 month’s corrected gestational age. The goal was to enroll 502 per group based on their power calculation. Furthermore the study design included randomization into two strata of 23 weeks 0 days to 27 weeks and 6 days and 28 weeks o days to 31 weeks 6 days. They managed to enroll 474 infants and in each arm there was good compliance with the allocated intervention (98% for cord milking and 93% for delayed cord clamping. What makes the study interesting though is that it was stopped by the data safety monitoring board after 236 were enrolled in the cord milking group and 238 in the delayed arm.
What happened?
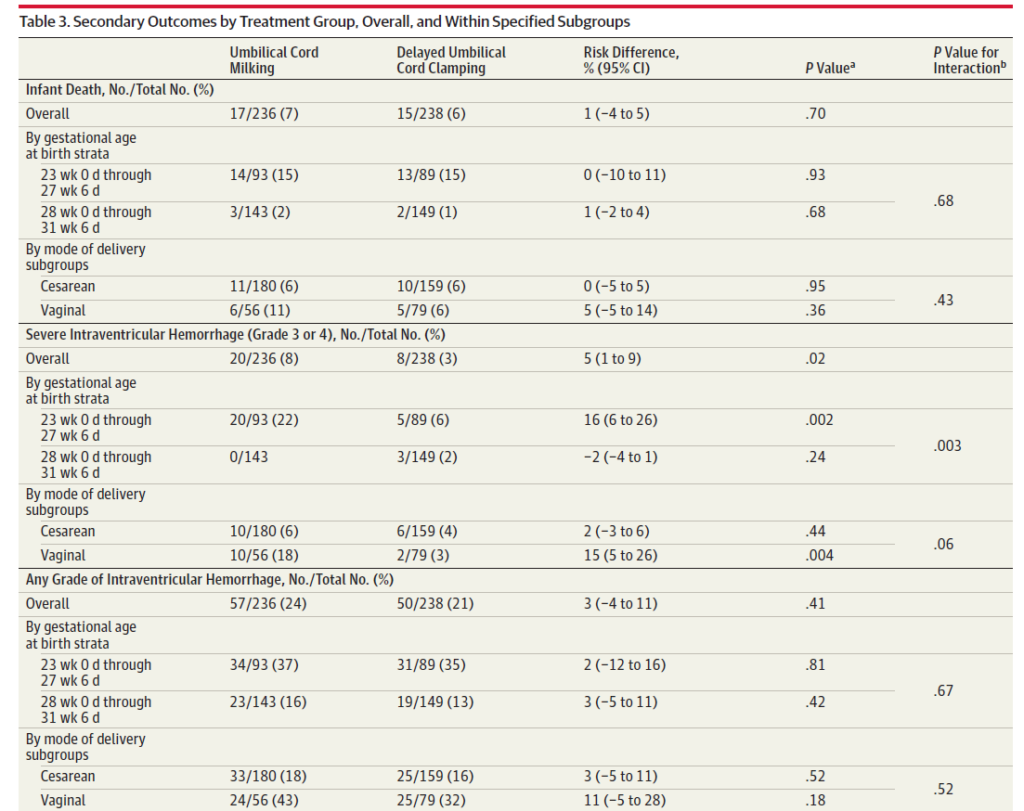
There were no significant differences between the maternal and neonatal demographics between groups. The mean time to clamping in the delayed group was 57.5 seconds compared to 22.8 seconds in the cord milking arm. The primary outcome at this point showed no difference between groups. What was concerning though was the pre-planned secondary outcome of severe intraventricular bleeding alone and is shown below.
The incidence of death from the above table was no different but in the group of infants between 23+0 and 27 +6 weeks there was a finding of 22% with severe IVH compared to only 6% in the delayed cord clamping group. This finding was understandably enough to shut down the study from enrolling further patients.
Why could this have happened?
I suppose we don’t know for sure but one of the benefits of writing a blog is that I get to speculate! The cerebral vasculature of small infants is quite fragile and furthermore is very poor at autoregulating its circulation. With cord milking I imagine it is similar to small boluses of blood. In a small preterm infant it may be that the baby is unable to limit the flow of blood adequately into the cerebral circulation leading to acute bleeding. Contrast this with the slow trickle of blood that one gets over a minute while the cord is not clamped.
This study is going to be a tough one to get past I suspect for those centres grappling with whether cord milking or delayed cord clamping in the best strategy. The question I think really these days should not be between these two but rather as I have written about before, how long should a delay in clamping really be? One minute is likely far too short while 5 minutes probably too long for most to be comfortable. I suspect the 2-3 minute range is where things will settle out. Additionally, strategies to allow resuscitation with an intact cord can and should be explored as those who are most sick at birth are likely the ones who could most benefit from a delay in clamping. More research is needed and I suspect you will hear about some before long on this site!
If you have an infant in the NICU and they were born at less than 2500g you probably have noticed that we tend to feed these babies very slowly. As you descend into the very early gestational ages and see babies under 750g or 1250g we feed these babies even more slowly. You may have heard your nurse or doctor talk about MEF or minimal enteral feedings. Typically these feeds are about 1 ml/kg of body weight given every couple of hours. If you have a 1kg baby then that would be about 1 mL of milk every couple hours. This is done for about 3-5 days and really “feeding” is a bit of a misnomer as what you are really doing is trying to “prime the pump”. By exposing the newborn gut to small amounts of breastmilk this MEF is really designed to help the bowel adapt to what is coming which is larger volumes of milk. We prefer that this milk is from humans as opposed to cow’s as the bowel tolerates this type of nutrition far better.
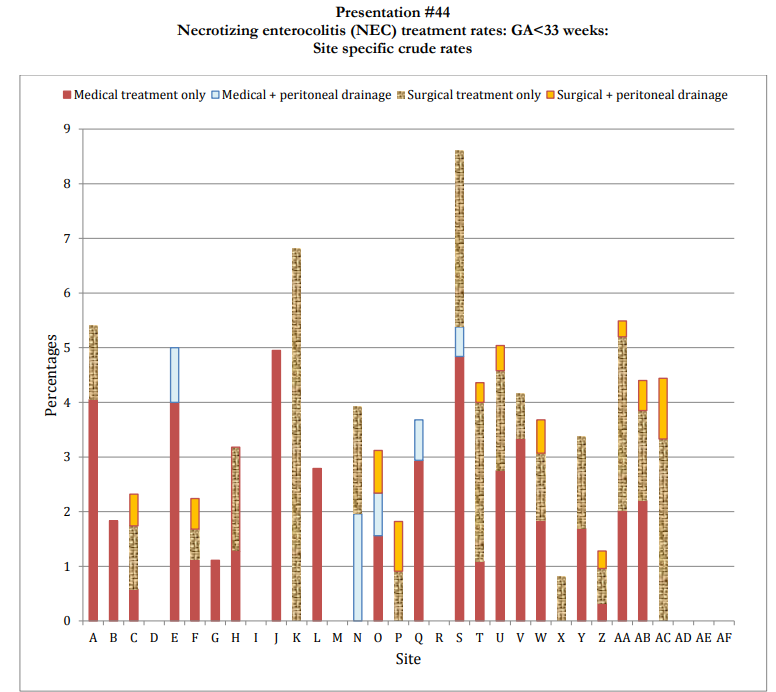
Once we start increasing feedings it may seem like it takes forever to get to what we call full feeds. We tend to increase the amount of oral feedings by anywhere from 20 – 30 mL/kg/day until we reach somewhere between 150-165 mL/kg/day of milk intake. During this time you may hear about us using TPN which stands for total parenteral nutrition. This is a combination of fats, sugars and protein plus important vitamins and minerals that we have in a liquid form (yellow and creamy white) that we give your baby so they get what they need while awaiting their feeds to reach the full point. While it may seem like a long time, it is not by accident. What we are trying to avoid is a condition called necrotizing enterocolitis (NEC). NEC is typically diagnosed on an x-ray but more recently people are using ultrasound to identify it. It can present clinically in a variety of ways but the one that usually triggers us to think about NEC as a possibility is blood in the diaper. This may be related to an intolerance to cow’s milk protein but if it is NEC we may also see other signs such as a distended belly, pain when we push on it or changes in vital signs such as temperature fluctuations and fast heart rates. Some babies may also present with failure to breathe and have pauses that may initially be thought to be just apnea of prematurity. NEC fortunately is less common than many years ago but it still occurs with varying frequency in babies under 33 weeks for the most part. The Canadian Neonatal Network is a group of 32 NICUs in Canada and tracks a number of conditions with NEC being one. Here is how the different sites compare across the country. What you can see from the graph is that the incidence varies but is generally abut 4-5% or about 1 in 20 babies in the NICU under 33 weeks.
The simplest way to think of it is that the lining of the bowel on its innermost surface absorbs nutrition but also has a dual role of keeping bacteria in the gut space and not allowing any to get into the tissues of the bowel. If the lining breaks down and allows bacteria to get into the tissues then we have the start of NEC. If this progresses we can ultimately see gas being produced in the bowel wall on x-ray and sometimes this gas escapes into the circulation of the liver and you will hear someone talk about “portal venous gas”.
NEC is a serious condition that if caught early may heal up but even in those cases on occasion the tissue damage can be permanent and lead to dead (necrotic) bowel being removed. When this happens the healthy bowel is typically brought up to the surface of the skin and a plastic pouch applied to the skin to catch the intestinal contents. This allows for the portion of bowel in the belly to heal and at some point many weeks later the bowel will be reconnected.
By now if you have a preterm infant in particular who has been born before 36 weeks you will have heard people talking about chronic lung disease (CLD). Sometimes they may also refer to it as bronchopulmonary dysplasia (BPD). The terms are really for all intents and purposes the same from a parent’s point of view. If you google CLD or BPD you may find stories of very cystic and damaged lungs with babies needing tracheostomies due to long term need for ventilation. While this can still happen, thankfully this new type of CLD we see is not like the one of old but rather is a newer entity that is more uniform and has less of a cystic nature. The “New BPD” is really more of a lung that has less air sacs (alveoli) than usual but the lung is less damaged than the BPD of old.
When your infant was born they may have had immature lungs without enough surfactant. Surfactant is kind of like the engine oil of a car. It helps to make the lungs less sticky and allows breathing to be a lot easier. Some babies are treated with CPAP while others need intubation and ventilation. While this positive pressure can be lifesaving, it also exacts a cost. We humans prefer to breathe using negative pressure meaning that we suck air into the lungs rather than have it pushed in. With each delivered breath the lungs of these fragile infants can be injured leading to the type of picture shown above.
This becomes a concern at 36 weeks. You may hear doctors talking about 36 weeks as if it is scary deadline that is on the horizon. We tend to obsess about that date. The big reason for this obsession is that units compare themselves across Canada and in other countries using the need for oxygen, nasal prongs, CPAP or ventilation at this time point. If your unit has a rate of CLD of 10% and another has 20% it tells the higher one that they better do something with their medical practice to lessen the incidence. In other words the 36 weeks is a marker.
As I have written about in another blog post, in 2020, 40 weeks may be the more relevant number as written in the post “The New BPD That Matters” the reality is that your baby is more likely to stay in hospital due to inability to feed orally or from apnea of prematurity. I am not saying that we as a team should not try and reduce the risk as much as possible for CLD but in case you were wondering what we are talking about when we talk about this condition this is it.
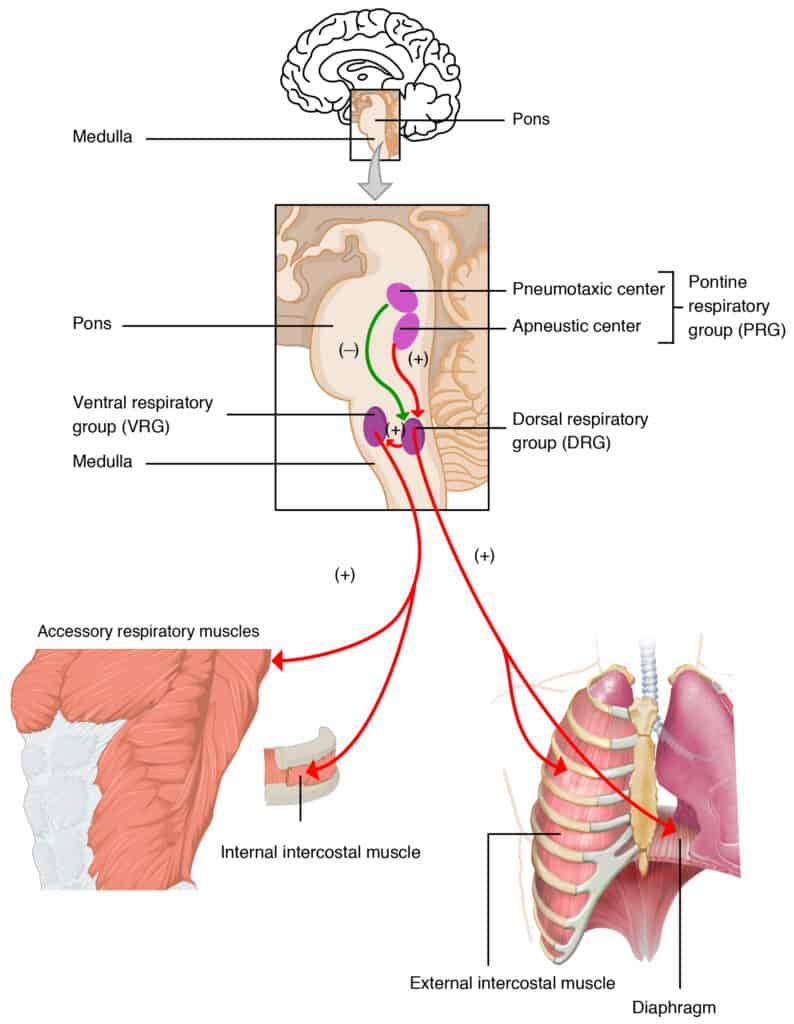
Our ability to breathe regularly is something most of us take for granted. We owe this function to a tiny area in the brain located in the medulla oblongata.
This area of the brain sends signals via nerves to the lung telling it to breathe in and out on a regular basis. For a preterm infant or even term baby this means there should be about 40-60 breaths per minute. Preterm infants are at risk for these events due to being neurologically premature but also due to a difference in the responsiveness of such infants to carbon dioxide levels in the bloodstream. In term infants and throughout life we are very responsive to higher levels of carbon dioxide. We like to keep it pretty tightly controlled which is why if you hold your breath and your carbon dioxide levels rise you feel like you need to take a breath. In preterm infants this response is blunted.
Pauses in breathing are called apnea and when they occur in a preterm infant they are known as apnea of prematurity. These are usually defined as stoppage of breathing for 20 seconds or longer or if shorter there is bradycardia (<100 heart beats per minute), cyanosis (bluish color to the skin), or pallor. They are so common under 37 weeks that I consider them a normal part of the preterm journey. You can see how common it is in the figure below. We also know that they are far more common as gestational age decreases so that a 24 week gestation preterm infant will be far more prone to apnea than the 35 week counterpart.
Parents
often wonder if these drops in oxygen or heart rate are harmful. If the
events are called spontaneous it means that your infant recovers quickly from
these events without anyone stimulating your baby and so they are brief.
We tend not to worry about these types of events as they brain is not
likely to be affected. When events are happening more than a few times a
day and require your nurse to either stimulate your infant or require support
with a bag and mask to help your baby breathe this is where we become more concerned.
Even then the presence of bradycardia during these events is more
concerning than the oxygen levels as the poor heart rate means less blood is
going to the brain. It is hard though to determine exactly how many
events a day are actually harmful but intuitively if they are happening more
than a few times a day and needing support to recover this is where we usually
think about treatment.
The treatment of choice is caffeine. The same drug that is present in your soft drinks or coffee. It works by stimulating that centre in the brain that I talked about above. There are different dosing levels but you will see doses anywhere form 2.5 mg/g/d to sometimes 8 mg/kg/d for those babies with very resistant apnea. Some of those kids may need CPAP (mask on the nose) or intubation and a ventilator if they just won’t breathe. The good news is that they will grow out.
Most of our babies have their caffeine stopped sometime after they have reached the equivalent of 33 weeks (eg. born at 26 weeks this would be 7 weeks later). On rare occasion babies right up to term will have apnea as shown in the graph and for those kids if they are feeding well and otherwise ready for discharge we may choose to send you home on caffeine. Those kids though will need a follow-up study called a sleep study that will typically be done about 4 weeks later and require your child to come back for the appointment.