

Given that today is world prematurity day it seems fitting to talk about prematurity at the absolute extreme of it.
It has been some time since as a regional program we came to accept that we would offer resuscitation to preterm infants born as early as 23 weeks gestational age. This is perhaps a little later in the game that other centers but it took time to digest the idea that the rate of intact survival was high enough to warrant a trial of resuscitation. This of course is not a unilateral decision but rather a decision arrived at after consultation with the family and interprofessional team. To be sure it is not an easy one. Other centers have argued that resuscitation should be offered to those infants as young as 22 weeks gestational age and data now exists due to enough centres doing so to provide families with some guidance as to expected survival rates and importantly the likelihood of disability. This topic has been covered previously in /2015/09/25/winnipeg-hospital-about-to-start-resuscitating-infants-at-23-weeks/. Why cover this topic again? Well an article on CNN might have something to do with it.
Resuscitating Below 22 weeks
This week as I was perusing the news I came across a rather shocking article on CNN. Born before 22 weeks, ‘most premature’ baby is now thriving.  The article tells the tale of a baby delivered at 21 weeks and 4 days that now as a three year old is reaching appropriate milestones without any significant impairments. It is a story that is filled with inspiration and so I am not mistaken I am delighted for this child and their family that this outcome has occurred. When the lay press latches onto stories like this there is no doubt a great deal of sensationalism to them and in turn that gathers a lot of attention. This in turn is a great thing for media.
The article tells the tale of a baby delivered at 21 weeks and 4 days that now as a three year old is reaching appropriate milestones without any significant impairments. It is a story that is filled with inspiration and so I am not mistaken I am delighted for this child and their family that this outcome has occurred. When the lay press latches onto stories like this there is no doubt a great deal of sensationalism to them and in turn that gathers a lot of attention. This in turn is a great thing for media.
A Few Caveats Though
With the exception of pregnancies conceived through IVF the best dating we have is only good to about +/- 5 days when an early first trimester ultrasound is performed or the date of the last menstrual period is fairly certain. A baby though who is born at 21 weeks + 4 days may in fact be 22 +3 days or even more depending on when the dating was done (second trimester worse). Let’s not take away though from the outcome being this good even at 22 weeks. That is a pretty perfect outcome for this family but the point is that this baby may in fact be older than 21 weeks.
Secondly, there are millions of babies born each year in North America. Some of these infants are born at 22 weeks. How do they fare overall? From the paper by Rysavy et al from 2015 the results are as follows.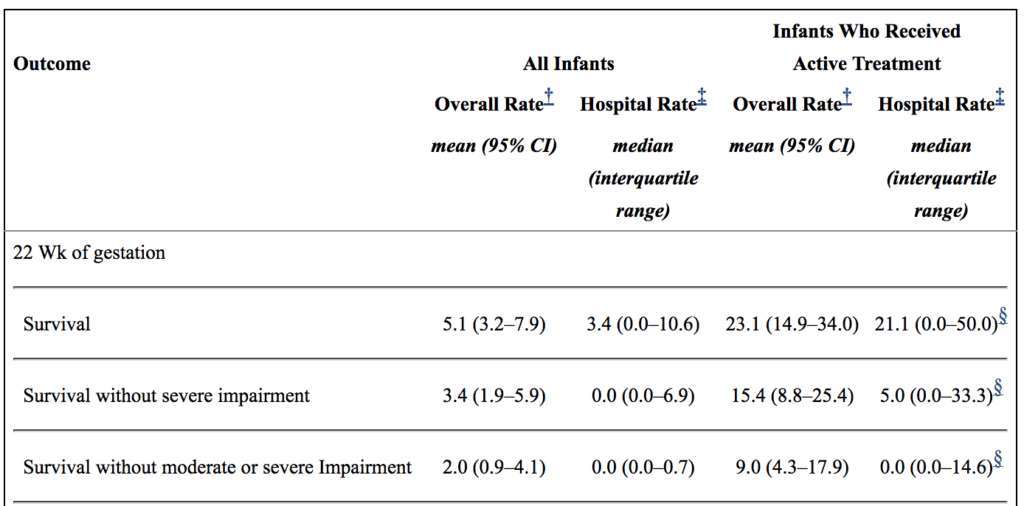
If you look at the overall rate of survival it is on an average of 5.1%. If you take a look though at those infants in whom resuscitation is provided that number increases to a mean of 23%. Intact survival is 9% overall. The odds aren’t great but they are there and I suspect the infant in the article is one of those babies. Flipping the argument though to the glass is half empty, 91% of infants born at 22 weeks by best estimate who are offered resuscitation will have a moderate or severe disability or die. I am not saying what one should do in this situation but depending on how a family processes the data they will either see the 110 chance of intact survival as a good thing or a 9/10 chance of death or disability as a very bad thing. What a family chooses though is anyone’s best guess.
Should we resuscitate below 22 weeks if the family wishes?
I guess in the end this really depends on a couple things. First off, how certain are the dates? If there is any degree of uncertainty then perhaps the answer is yes. If the dates are firm then I at least believe there is a barrier at which futility is reached. Perhaps this isn’t at 21 weeks as some patients may indeed be older but think about what you would offer if a family presented at 20 weeks and wanted everything done. What if it were 19 weeks? I suspect the point of futility for all lies somewhere between 19-21 weeks.
As I prepare to attend the annual meeting in Ottawa tomorrow for the Fetus and Newborn Committee I think it is prudent to point out just how difficult all of this is. The current statement on Counselling and management for anticipated extremely preterm birth I think hits on many of these issues. The statement is the product on not only the think tank that exists on this committee but was the product of a national consultation. I know I may be biased since I sit on the committee but I do believe it really hits the mark.
Should we be thinking about resuscitating at 21 weeks? For me the answer is one clouded by a whole host of variables and not one that can be easily answered here. What I do think though is that the answer in the future may be a yes provided such infants can be put onto an artificial placenta.  Even getting a few more weeks of growth before aerating those lungs is necessary may make all the difference. The NICUs of tomorrow certainly may look quite different than they do now.
Even getting a few more weeks of growth before aerating those lungs is necessary may make all the difference. The NICUs of tomorrow certainly may look quite different than they do now.
You wrote that if a 22 week premie is offered resuscitation and survives, 91% of them will have a moderate to severe disability. I don’t think that’s entirely correct. The issue is the phrase “if they survive”.
If you take 100 of these babies, 23 will survive and of those survivors, 9 will be without a moderate to severe disability. So if you take all survivors, the chance of being intact is actually 9/23 = 39%. And the chance of being neurologically devastated IF you are a survivor is 1-0.39 = 61%, not 91%.
It’s a subtle distinction, but it’s important to be precise in our language. But it was an interesting and provocative read! Thanks!
This genuinely is concerning for me. It is not that I am against all the life saving measures taken everyday but I have to wonder is this just becoming “because we can”. I am in awe everyday and so incredibly grateful for many of these procedures if it wasn’t for them I wouldn’t have any of my children. But my first pregnancy ended at 26 and 3 and at the time they weren’t going to save them before the 26 mark and I was devastated but after losing one of my boys and then a 4 month stay for my son it was an incredibly rough time for us. So when my second pregnancy began to show complications and there was discussions of a 24 week delivery my husband was flat against it. I had the same feeling of not wanting to go through that again but these were my babies and I couldn’t say no if that was an option. It is something I would have not wanted and would have rather been told again there is nothing they could do. It’s not that I don’t fiercely love my children but nothing they told me or went over first time around even remotely prepared me for what happened. I am coming from this topic as an outsider and not educated in any of it so I don’t know what goes into all of these decisions but this it a scary thought for me.
This is a discussion that it is getting lots of attention. The above comments exemplify the present state of affairs of physician-parents in the decision making process, to intervene or not in fetuses to be born at the limit of periviability.
I just posted my thoughts on a similar topic discussion panel in Doximetry.
As the author states very well above, the accurate dates at this period of gestational age are very difficult (see above pic, the eye lids are not fused?). A few days off could carry a very different course of events and outcomes.
In my humble opinion, a very truthful pre delivery discussion between parents and obstetrician-neonatologist is of paramount importance. The likelihood of death and short-long term outcomes should be discussed and documented. The importance of this discussion should include the possible devastating infant outcomes including respiratory, gastrointestinal and neuro-developmental. These infants long term problems have tremendous repercussions on the infant an family and should be included.
Sometimes, there is only a final request from parents to give a trial of life, in these cases, we should include parameters of support withdrawal.
It takes 40 weeks to make a human brain. Until the long term outcomes not 2 year outcomes are discussed with parents not with terms of mild disabilities meaning an IQ of 50. That is not mild if your 13 year old is not speaking clearly, and still sleeps in pull-ups. 3rd grade outcomes are the important ones reading and writing and especially the social skills which preterms have lifelong issues with. Try finding any medical, developmental, OT, speech, PT, daycare, or school and babysitting for these children. We all know the name of that 1 miracle baby, but there are so many families living with with chronic sorrow that we created with that ETT and dose of surfactant. The bike that will never be ridden, spelling bee never studied for, DC patrol trip not taken. Tears of joy the first time words I love you at 9 years old because it took 6 hours a week of speech therapy, and answered so many prayers! 22 weeks is criminal and cruel it’s called a spontaneous abortion and there maybe a very good reason nature is being nature. Our job should be comforting parents.