The 10th Annual Bowman Symposium did not disappoint! World class presenters gathered to provide a top to bottom update on a variety of topics spanning from the nervous system to Genetics. After a day and a half of presentations though I was left with some concerning (scary) thoughts and it seemed Halloween was the perfect time to share them with you!
How Much Oxygen is Just Right?
Dr. Ola Saugstad provided a wonderful history of the use of oxygen in Neonatology. After his talk it was clear that oxygen is most definitely a drug with its most concerning side effect being the production of oxygen free radicals in the body. If we are too restrictive aiming for saturations of 85 – 89% we spare our infants ROP but put them at greater risk of death. Too high at 91 – 95% and they may survive but with more ROP (BOOST and SUPPORT). If we resuscitate with 100% oxygen that is associated with worse outcomes but so too is 21% in our newborns < 28 weeks. The NRP would advise us to use 21 – 30% to start in this group for resuscitating but he recommends 30%. Certainly the recent publication by Jack Rabi out of Calgary suggests room air may in fact be harmful in this group as a starting point! After 50 years of research we still don’t know what to give newborns to help them start their life outside the womb. Scary.
It’s All In The Name
Next up is Dr. Aviva Goldberg who raised a very important point that I had not considered before. In every researchers quest to come up with a catchy name for their study that people will remember, the connotation is equally important. The SUPPORT study came under heavy fire (commentary here) after a surprising increase in mortality was found in the arm randomized to 85 – 89% saturations. Families sued the investigators and in their complaints they were angry about being misled. How could a study that was named the SUPPORT study do anything other than help their children? The title in and of itself they argued misled them as they never would have thought increased mortality could be a risk. Researchers make sure you test out your clever names with parents before finalizing your studies. The decision otherwise could come back to haunt you…
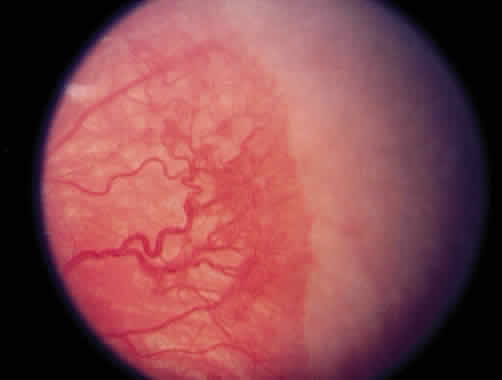
Jury Still Out on Bevicizumab (Avastin) for ROP
Dr. Ian Clark provided an overvue of the current state of thinking on treating ROP. For central disease in Zone 1 Avastin is preferred but for more peripheral disease laser seems to still be recommended due to its decisiveness in eliminating the disease without affecting future vision. Concerns continue though with respect to potential systemic effects of putting an anti-VEGF medication in the eye. Can it leak out and cause disruption to angiogenesis in other organs and in particular the brain? A recent poster at the CPS meeting in Toronto entitled Neurodevelopmental outcomes of extremely preterm infants treated with bevacizumab for severe retinopathy of prematurity indicates that there may be greater impairment in those receiving injections. There are several flaws in this paper though including greater numbers of males (we always do worse), more sepsis and worse SNAP-II scores in the injection group but the results have been making it into discussions leaving Ophthalmologists wondering if they are doing the right thing…very scary.
Cow’s Milk Human Milk Fortifier Is Safe For Premature Infants… Or is it?
Next up was Dr. Bill Diehl Jones who presented in vitro data on the effect of these supplements with respect to their contribution to oxidative stress. Such stress has been associated with BPD, NEC and ROP to name a few disorders in preemies. A paper published this week in which intestinal cells were exposed to human milk with HMF experienced significantly increased intracellular oxidation, cell damage, and cell death compared to those exposed to just breast milk. A paper from 2013 indicates that premature infants fed HMF experience increasing levels of urinary isoprostanes (a measure of oxidative stress). We know that infants receiving these products experience better growth and bone density than those without exposure but is there a cost? Will further research in this area drive us towards exclusive human milk based diets? The seed that has been planted in my head now questioning the safety of this product I use every day…a little frightening.
Curtailing Antibiotic Use And The Coming Black Swan
John Baier spoke about practice variation between Neonatologists in terms of the decision to prolong antibiotics or not in the face of negative cultures. While we do have variation, the good news is that we overall have cut down our tendency to prolong past 48 hours in the face of negative cultures. If we practice long enough though, the Black Swan will eventually rear its ugly head. The Black Swan is an exceptionally unusual event but one that has dramatic impact. How will we respond when a patient becomes septic after 48 hours and the antibiotics were stopped? Will we panic and change our practice entirely to avoid the internal pain again of feeling like we made a mistake or remember that we have saved countless infants from the long-term effects of indiscriminate use such as NEC, atopic disease and obesity in childhood just to name a few. It is this nagging doubt I have about how we will react that gives me cause to worry!
Finishing With a Miracle
It doesn’t seem right to end on a down note so I thought it would be worth celebrating that a cure has been found for something very scary. Hypophosphatasia is a rare disorder of the bone which was previously lethal in many cases. Thanks to research that our own Dr. Cheryl Greenberg led here in Canada we are able to successfully treat these children now. The Bowman symposium showed us incredible videos of such treated children and to end this post I found this video from Youtube of Gideon who was one of these patients treated with FDA Okays Asfotase Alfa (Strensiq). If you would like to leave this post with a smile on your face until next Halloween have a look at the video!
Elon Musk, a name synonymous with technology in our time (as the brains behind the all-electric Tesla automobile), had this to say about the “Good Old Days”
“If anyone thinks they’d rather be in a different part of history, they’re probably not a very good student of history. Life sucked in the old days. People knew very little, and you were likely to die at a young age of some horrible disease…”
I wonder what he would say though about Sister J Ward who worked in the premature unit at Rochford General Hospital, Essex in the 1950s. It was during this time that she took a baby outside with her to enjoy a warm afternoon. Upon returning to the unit and taking off the sheet that accompanied the child she noticed a discrepancy between the yellow colour which remained under the covered skin and that which had been exposed to sunlight. Her observation led her to conclude that the sunlight had in fact been responsible for the change (and she was right!) but her conclusion was largely ignored.
Soon thereafter a tube of blood provided the convincing evidence that the sun was in fact directly responsible for such a change. This tube which had been left on the windowsill in the sun was tested for a bilirubin level and found to be low. As the care providers felt the test was inaccurate a repeat sample was drawn and the fresh tube contained a much higher level. A repeat sample of the blood that was again left in the sun showed an even lower level than previously seen inspiring researchers to seek out the effect of light on bilirubin. This ushered in the age of phototherapy lamps that are used around the world today. The design of such lamps has undergone many changes with the current models mostly focusing on the generation of light in the blue spectrum. Mostly gone in the developed world are the long phototherapy bright light tubes that were ubiquitous when I was in residency. It didn’t start off that way though. All you needed was a little golden sun!
A Randomized Trial of Sunlight to….
This month in the New England Journal of Medicine a non-inferiority study has been published comparing conventional phototherapy with BiliBlankets to you guessed it…sunlight. The study took place in Nigeria where such a study is both practical and possible. Conducting the study in Winnipeg for example would yield a treatment that could be used for 3-4 months a year at best but in a more temperate part of the world it indeed is a reasonable question to ask. The infants randomized to sunlight were placed under filtered light using either a canopy made of an Air Blue 80 film on overcast days or when sunny, in a Gila Titanium film. These films have been shown to essentially block all UV light while allowing light in the blue spectrum through. Aside from Sister Ward demonstrating that sunlight was an effective treatment for jaundice over 60 years ago, a significant motivation for determining if sunlight could be employed is the cost difference of the two strategies. A BiliBlanket will cost between 2-3000 dollars each while these canopies can be made for $0.55 and $1.50 per square foot of film type respectively and $44 and $120 for a canopy for six to eight mother–infant pairs with Titanium and Air Blue 80 films. In countries where resources are scarce one can see the compelling reason to try such a strategy.
The Results
The criteria for efficacy were twofold. The first outcome was achieving a rate of increase in total serum bilirubin of less than 0.2 mg per deciliter per hour for infants up to 72 hours of age or secondly a decrease in total serum bilirubin for infants older than 72 hours of age who were receiving at least 5 hours of phototherapy. After comparing 250 courses using sunlight to 311, five hour exposures to BiliBlankets, sunlight was found to be equally effective. Interestingly, the spectral irradiance (measure of the intensity of the light source) however was significantly higher in the group receiving sunlight 40 vs. 17 μW per square centimeter per nanometer, P<0.001. Additionally, the total area covered was greater under the canopy which may help to explain why in a secondary analysis the rate of decline in bilirubin was found to be faster with sunlight.
But is it safe?
Putting babies under the sun for 5 hours would seem to go against everything we have been taught but remember this was filtered light so sunburn was not a concern. Temperatures were monitored for all children and if necessary they were moved into the shade to cool off or in other cases on quite hot days prophylactic cool towels were applied intermittently. In the end though only one baby recorded a short-lived temperature over 39 degrees, no babies became dehydrated and in only one case was a doctor called to see a child.
Final Thoughts
We are blessed to live in a country where we have ready access to phototherapy blankets, overhead lights that are either independent free units or integrated into expensive neonatal beds. This is not always the case in the developing world. I find it simply amazing that a discovery over 50 years ago that led to the development of an entire industry would one day be simplified back to where it all began. We must not forget that while bilirubin encephalopathy leading to kernicterus is rare in the developed world, in places without access to phototherapy it is a real and present danger. We now know that the most naturopathic treatment of all; the sun which is free and readily available is just as effective and possibly more than our high-tech devices.
Elon Musk may be one of the most brilliant inventors of the modern era but with respect to caring for babies with yellowing of the skin, Sister Ward had a leg up on him.
On occasion two articles will be published in short succession and have discrepant findings. This appears to be one of those times. Hishikawa K in Japan published a paper in September entitled Pulmonary air leak associated with CPAP at term birth resuscitation while Calebi MY from Turkey published Impact of Prophylactic Continuous Positive Airway Pressure on Transient Tachypnea of the Newborn and Neonatal Intensive Care Admission in Newborns Delivered by Elective Cesarean Section in August of this year.
The findings as we will discuss were quite discrepant which on the surface leaves the practitioner in a quandry. How do I best treat my patients? The key difference between the two studies was the finding of an increased rate of pneumothorax in the study by Hishikawa when CPAP was used in term infants with respiratory distress after delivery. Curiously prophylactic CPAP of +5 was used in both studies but the populations under study were quite different. The study by Calebi targeted infants between 34 0/7 weeks and 38/6/7 weeks vs term infants in the study from the Japanese group.
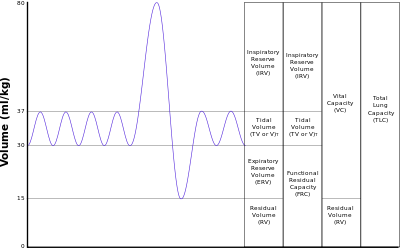
Another important difference is the utilization of CPAP which in the study by Calebi involved prophylactic administration within twenty minutes of birth and in the Japanese cohort the indication was the development of symptoms. Thinking about this for a moment, these two groups are actually quite different. A newborn with TTN has an increased amount of interstitial fluid that has not made it’s way to the hilum for reabsorption in the lymphatic system. The lungs of these infants are heavier with fluid than comparable infants without such pathology and therefore are also less compliant. Non compliant lungs are prone to microatelectasis as the infants progressively experience alveolar collapse. The longer the clinician waits to start supportive CPAP the more the lungs collapse and greater negative pressure is required to open these closing alveoli. Furthermore if there is fluid in the airway itself there is the potential for a ball valve mechanism to come into effect whereby air is able to pass through the dilated airways during inspiration but on expiration the collapse leads to air trapping. Such trapping places the infant at risk for air leak. CPAP is used to establish an adequate functional residual capacity (FRC) as indicated in this picture. Failure to do so results in atelectasis.
The Japanese study examines the impact of CPAP after a change in guidelines in 2010 suggesting that CPAP should be utilized in the delivery suite for those infants with ongoing respiratory distress. The study by Calebi really examines a different patient group being those who are near term patients with TTN who have early CPAP implemented. The early administration of CPAP may be the technique that prevents alveolar collapse as mentioned above and avoids the requirement by the infant to generate such high negative pressure with its inherent risk of air leak.
Is All CPAP The Same?
Another important distinction between the two papers is the way in which CPAP was administered. The Japanese utilized a flow inflating bag with a pressure valve and manometer while the study by Calebi employed a T-piece resuscitator. When it comes to maintaining CPAP there is no question having used both devices that I find the T-piece resuscitator much easier to use and over longer periods the reliability of the pressure delivered by the T-piece would be superior to that with the flow inflating bag. The Neopuff T-Piece Resuscitator possesses a pressure relief valve which could help during an instance when the patient is crying or breath holding. The constant flow without a relief valve could lead to airleak which is precisely the situation that may occur during the use of a flow inflating bag.
Yes there was over a three fold increase in airleak at near term gestational age in the Japanese cohort but this was not seen at all in the Turkish study in which CPAP was implemented early. So the message here is that if you start CPAP early enough you can prevent airleaks from occurring. This in and of itself is worth implementing.
Can CPAP Reduce Hospital Admission to NICU?
There is more to the story however. The Turkish group demonstrated a significant difference in admission rates to the NICU as shown in the following figure. The results here although just achieving significance should not be minimized. Avoiding progressive atelectasis decreases admission rates. The conclusion here is that there is little benefit in adopting a wait and see approach to those kids born by elective c-section. While it is true that you may be treating a significant number of healthy patients between 34 0/7 – 38 6/7 weeks with CPAP it is for a brief period and makes a significant difference in frequency of admission.
We live in an era of bed shortages and I would argue that anything we can do to reduce admissions and moreover keep babies with their parents is worth exploring. From my perspective treating these kids with the appropriate CPAP device for twenty minutes after birth is well worth it. Perhaps your unit should consider the same.
I often catch myself saying that Neonatology being a relatively young speciality has so much more to discover. Any Pediatric resident can attest to this when they scan their journals and see so many articles exploring uncharted territory. As we continue to march forward it gave me pause to realize that we had lost someone in August who quite literally put the intensive in Neonatal Intensive Care.
Dr. Forrest Bird was an inventor and a pilot who was inspired to create a device to deliver oxygen to pilots flying at high altitude. This was needed due to the inability of the allied airforce to fly as high as the German planes. He was able to reverse engineer of sorts a solution to the lack of oxygen the airforce experienced and thereby level the playing field. This technology became the backbone behind the Bird Respirator first produced in 1950. This device is considered to be the dawn of the ventilator and was soon to put the iron lung out of business.
In 1963, following the death of John F. Kennedy’s son Patrick at 34 weeks from RDS research in the field of Neonatology blossomed bringing something positive out of tragedy. Funding for research in the area uncovered the cause of RDS as surfactant deficiency by Dr. Avery and a great number of papers followed exploring the concepts of surface tension, atelectasis and the effects of pressure on expansion of the newborn lung. While I clearly was not working in the field back then I have no doubt the clear need for a device to help these newborns with collapsable lungs inspired Dr. Bird to search for a solution. In 1970 he produced the Baby Bird Ventilator which was essentially a smaller version of the original. Up until this point, there was little that could be done for such preemies and other children in respiratory failure. By some accounts the ability to ventilate a newborn with positive pressure led to a reduction in mortality from 70% to 10% due to respiratory distress.
How Big An Impact Did It Have?
According to the World Health Organization approximately 15 Million babies are born before 37 weeks each year in the world. In the US alone about 1 in 9 babies are born at these gestational ages which translates to about 450000 babies per year. If we take a conservative estimate that 50% will have some degree of respiratory distress and need ventilation or CPAP that translates into 7.5 million babies every year helped by technology that Dr. Bird brought into this world. While true that the Baby Bird would be replaced by more advanced technology as years passed and ventilators of today bear little resemblance to the original design, every device owes a nod to the its ancestor the Baby Bird.
It has been 45 years since the Baby Bird came to market and there are few people working in the field today who would remember using this particular ventilator. Its inventor both directly and indirectly is responsible for saving the lives of millions of babies over a 45 year span. How many of us working in the field today can say that we know someone who has made such an impact in recent memory. Dr. Bird was a hero in Medicine and in particular Neonatology and for that reason in received the National Medal of Technology and Innovation from President Obama in 2009.
I hope that this piece helps to educate even a few people about this modern day hero. It also serves to remind me as we begin to lose the pioneers in our field that perhaps we aren’t such an young specialty anymore after all.
There is no question that adequate weight gain is a necessity in the NICU. We commonly strive for 15-20 g/kg/d in our centre but sadly our smallest infants often struggle to achieve such increases in mass. If you have worked with me you will often hear me state that after the acute issues are dealt with in a ELBW infant the most important thing we need to focus on is nutrition if we want to help these infants come off respiratory support. They simply need stronger bones, more muscle mass and adequate well balanced nutrition to heal some of the damage that unfortunately occurs while they are receiving positive pressure ventilation.
Does weight gain right after birth matter?
In the past few years however several papers have challenged this belief of mine in suggesting that the time shortly after birth is equally important in particular with reference to retinopathy of prematurity. Associations between poor weight gain in the first 2-6 weeks of age and worse ROP have been noted. The challenge as always with such retrospective or even prospective studies is the presence of confounders. Does the finding of worse ROP indicate that the lack of weight gain is in fact causative or is it reflective of other factors at work? When we are looking at retrospective studies the authors typically will try and control for such known factors but there may be other factors that have been unaccounted for. In particular, is the lack of weight gain attributable to a unit that pays poor attention to nutrition or a result of inflammatory states such as sepsis causing a catabolic rather than anabolic state in the child? Add to this that lipoprotein lipase tends to become less active in the presence of such inflammation and a rising triglyceride level will often dictate that lipids be reduced or stopped altogether further compromising nutrition.
The Evidence
A Swedish paper by Stoltz Sjöström et al published in 2015 examined 498 infants born between 22 0/7 – 26 6/7 weeks of age and sought to determine if poor weight gain and energy intake were responsible for increased rates of ROP in NICUs in Sweden. This retrospective study included infants with an overall rate of Grade III-V ROP of 34.5%. When looking at the differences in a number of variables including weight gain and energy intake in the first four weeks of life there appears to be a cutoff of 100 Kcal/kg/d as an average intake that predicts the risk of ROP. That is if the caloric intake on average over four weeks is less than 100 Kcal/kg/d then the risk of severe ROP increases. When controlling for all variables none of the constituents of nutrition appeared to be significant (protein, fat, carbohydrate) but rather the energy intake. Importantly two additional factors that bore out significance were prolonged ventilation and number of blood transfusions.
While this was a fairly good sized study there are a number of confounders here that again raise the question of what truly is causing the higher rate of ROP. ROP is known to be affected by oxygen use. The current state of thinking is that higher oxygen saturations (Support trial) as well as wide swings in oxygenation may predispose to worse ROP. Given that two important factors increasing the risk of severe ROP in this cohort were prolonged ventilation and need for blood increased numbers of blood transfusions these may well be a proxy for labile oxygenation. I can’t resist the speculation additionally that the lower energy intake may have delayed the building of adequate muscle and bony framework to assist these infants in coming off the ventilator. Sicker infants need more transfusions as well as the bone marrow takes on a quiescent state. It may well be that lower energy intakes are associated with worse ROP but as with other papers looking at this factor it may not be causative (at least directly).
The other thing to bear in mind is that this study is a retrospective analysis of a study originally published in 2009 called the Express Study. Much has changed in the realm of Neonatal Nutrition. When maternal breast milk is unavailable many units have access to donor milk. Early and more aggressive TPN has become the norm since that time with many infants receiving a starter solution on day 1 and TPN late on day 1 or certainly on day 2. Lastly, many centres are now changing from what had been the standard soy based lipid emulsion to one such as SMOF that contains omega-3 fatty acids with inherent anti-inflammatory effects. Given all these changes it would be interesting to see if many infants these days are receiving such low caloric delivery and even if so if their rates of severe ROP are indeed higher.
Conclusion
My take on this therefore is that while we should all strive for better nutrition in our infants I do not believe that the evidence is there yet that an average caloric delivery in the first 4 weeks of age of less than 100 Kcal/kg/d is causing worse ROP in our infants. We will never have a randomized controlled trial to determine such a causative relationship so these sorts of studies are the best we can do. Fortunately, even if there were a cause and effect relationship we are already striving to keep our goal calories above the threshold which seems to be associated with worse outcome.
In essence let’s all keep our eye on the energy being provided and with time all should be well provided we continue to be extremely vigilant with minimizing oxygen exposure in these vulnerable infants.



 It was during this time that she took a baby outside with her to enjoy a warm afternoon. Upon returning to the unit and taking off the sheet that accompanied the child she noticed a discrepancy between the yellow colour which remained under the covered skin and that which had been exposed to sunlight. Her observation led her to conclude that the sunlight had in fact been responsible for the change (and she was right!) but her conclusion was largely ignored.
It was during this time that she took a baby outside with her to enjoy a warm afternoon. Upon returning to the unit and taking off the sheet that accompanied the child she noticed a discrepancy between the yellow colour which remained under the covered skin and that which had been exposed to sunlight. Her observation led her to conclude that the sunlight had in fact been responsible for the change (and she was right!) but her conclusion was largely ignored.


 Failure to do so results in atelectasis.
Failure to do so results in atelectasis.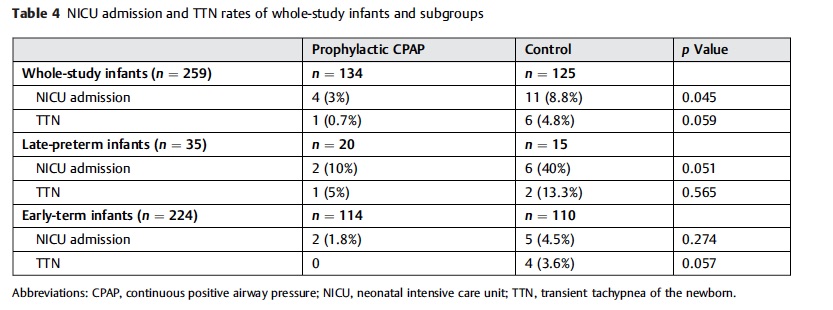 figure. The results here although just achieving significance should not be minimized. Avoiding progressive atelectasis decreases admission rates. The conclusion here is that there is little benefit in adopting a wait and see approach to those kids born by elective c-section. While it is true that you may be treating a significant number of healthy patients between 34 0/7 – 38 6/7 weeks with CPAP it is for a brief period and makes a significant difference in frequency of admission.
figure. The results here although just achieving significance should not be minimized. Avoiding progressive atelectasis decreases admission rates. The conclusion here is that there is little benefit in adopting a wait and see approach to those kids born by elective c-section. While it is true that you may be treating a significant number of healthy patients between 34 0/7 – 38 6/7 weeks with CPAP it is for a brief period and makes a significant difference in frequency of admission.