by All Things Neonatal | Jul 9, 2015 | Neonatology, nutrition
Will that be q2h, q3h or q4h feeding? When I started my residency in Pediatrics that was the question I needed to ask before writing an order to start oral feeding in a preterm infant. At the time it seemed perfectly reasonable but I have to admit the question for me was “What if they aren’t ready?”. Does a baby who won’t take the breast or bottle at the 3 hour mark clearly show they aren’t able to feed or that they really are just not ready to feed? We commonly say that children are not small adults. Hospitalized adults commonly will utter the words “I’m not hungry” when their food tray is brought to them. This may be a reflection of what has been put before them rather than whether hunger exists or not but they seem to be able to be ready to eat so why not children and by extension preterm infants in the NICU.
My approach to feeding premature infants was fairly consistent until about 10 years ago when nurses in Edmonton, Alberta (in a level II unit) introduced me to “semi-demand” feeding. What I find interesting about this, is the paucity of evidence that existed on the subject. At the time, the evidence really centred around one paper but the impact of the approach was undeniable. In 2001 McCain et al published the randomized controlled trial involving 81 infants A feeding protocol for healthy preterm infants shortens time to oral feeding. The concept of semi-demand feeding was to assess each infant (once preterms reached 32-34 weeks CGA) before a feed for signs “of feeding readiness”. This was accomplished through offering non-nutritive sucking every three hours before a scheduled feed. If the infant was found to be in a wakeful state, the oral feeding was commenced but otherwise the infant was left for 30 minutes with NNS attempted again. If the infant was still not ready then a gavage would be given. The key here is that the infants were monitored for signs of feeding readiness rather than insisting upon an arbitrary time for their next feed. The study findings were a halving of the time it took to reach full feeds (10 days in control vs. 5 days in semi-demand) with no difference in weight gain observed between groups. The latter point is worth emphasizing, as the concern with semi-demand has been from some that in a worst case scenario where feeds took place every 3.5 hours a baby would miss one feed compared to another infant on a q3h schedule. This fear though does not bear out in the study.
The experience in the centre I currently work at has been so positive that it is hard to find a patient that is not fed in such a way whether a physician orders the approach or not! What is truly fascinating to me is how effective the approach seemingly is and has been adopted again with very little evidence compared to that traditionally needed to change a practice in the neonatal world. Interestingly, although we can’t say for sure we have noticed year over year declines in length of stay for infants born with a birthweight of 1500 – 2000g since the introduction of semi-demand feeding. This could be a coincidence as this has not been the only practice change in our units but it certainly is interesting.
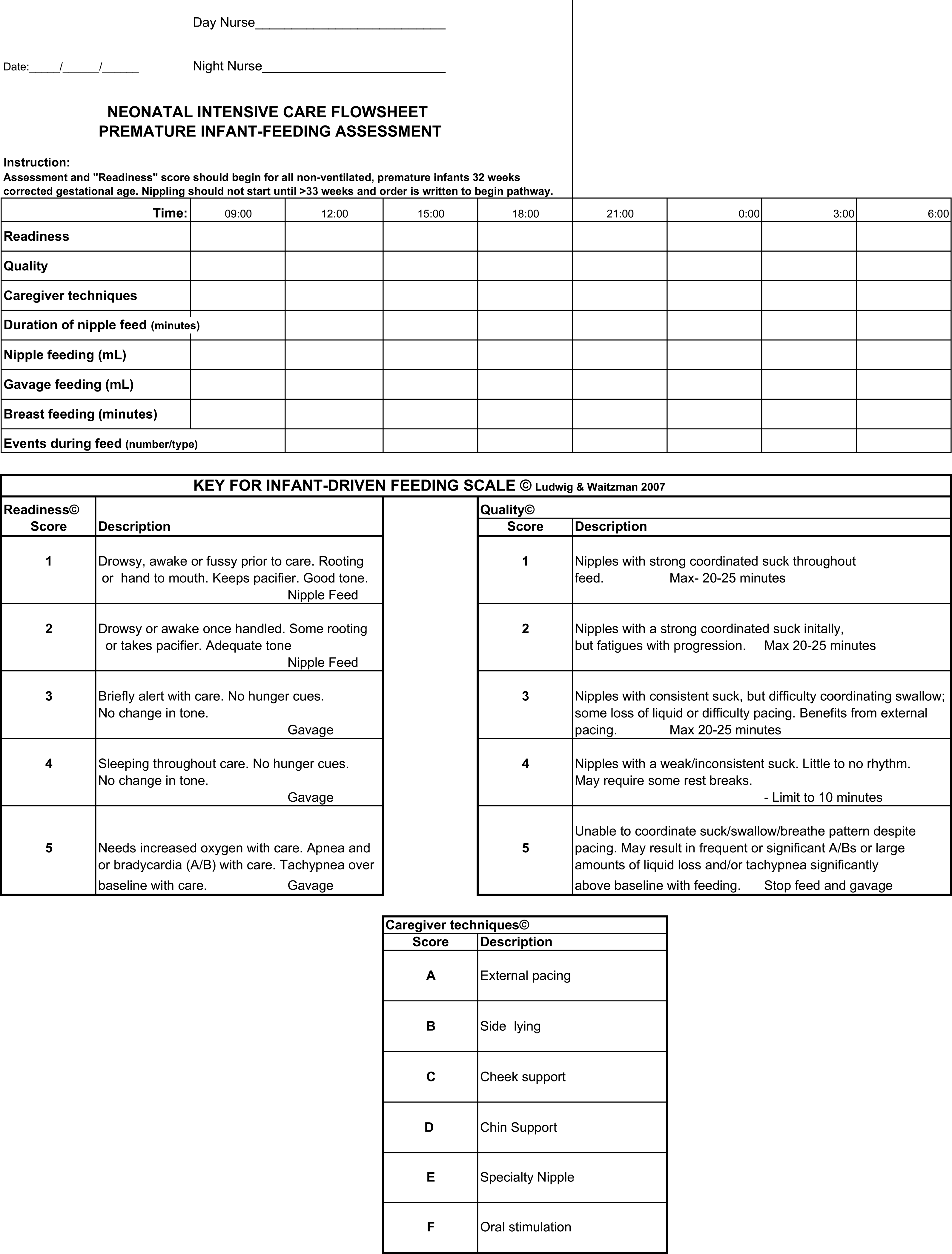
I was delighted to see a paper published this week on the topic by Wellington and Perlman. This was a Quality Improvement project entitled Infant Driven Feeding in Premature Infants: A Quality Improvement Project. This study compared three periods. The first was one in which physicians set the feeding schedule (PDF), the second a training period for a new system and the last the infant driven period (IDP). In the PDF phase, the physicians would order one oral feed a day, then two, three and so on when the full feed was attained at each prescribed level. In the IDF period an assessment sheet for feeding readiness would be completed before each attempt and the decision to offer an oral feed based on the perceived ability to feed at that time.
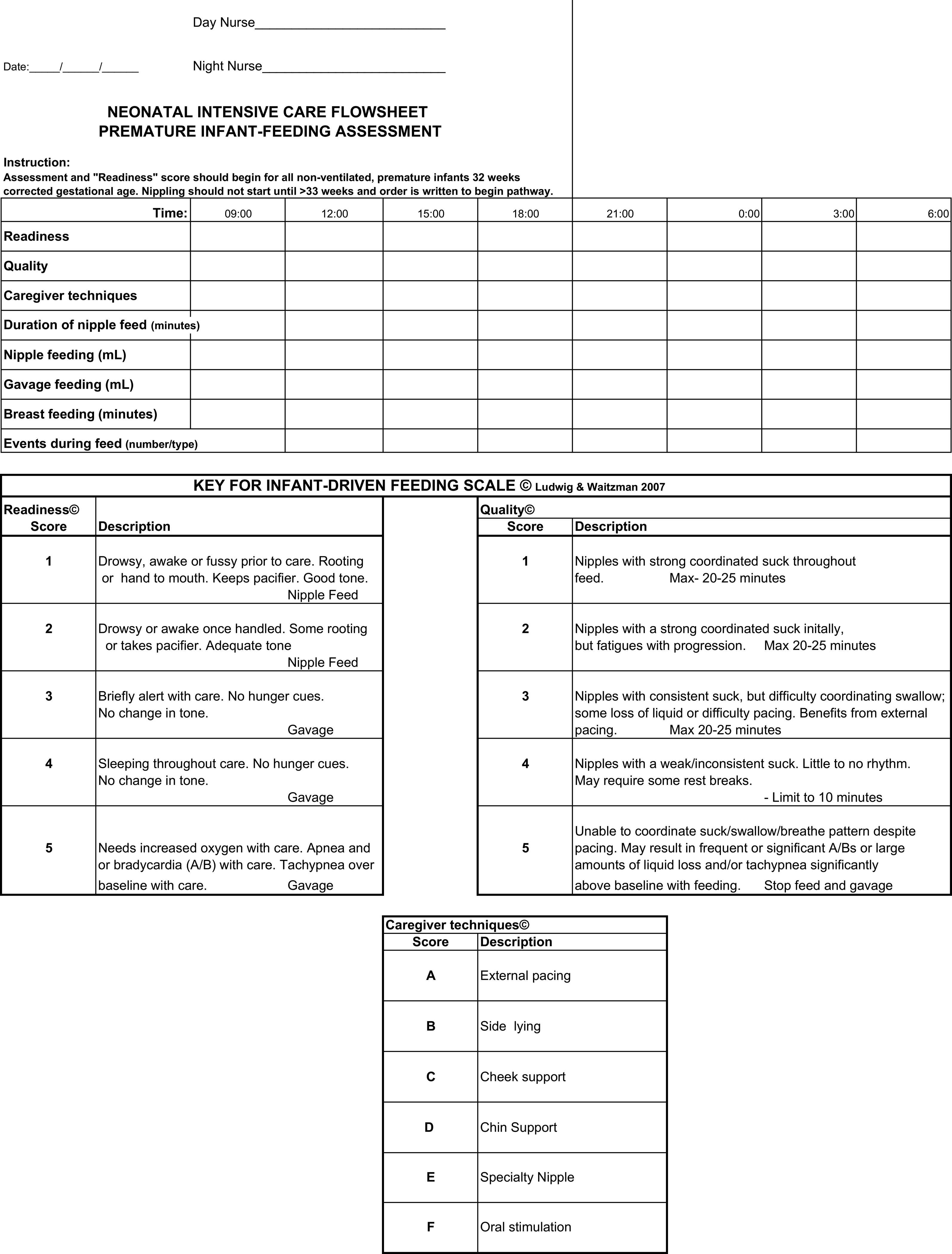
While this study was not an RCT it is a much larger group of patients than the study by McCain. This comparison was between 153 PDF vs 101 IDF patients. Feeding readiness assessments would start at 32 weeks CGA but feedings would not be offered by either approach until 33 weeks CGA similar to our own approach to feeding for the most part. The use of IDF made no difference to timing of first attempt at nipple feeding. The time to attain full nipple feeding was where significant differences in approach became apparent.
Time to reach full nipple feeding by gestational age at birth:
<28 weeks: IDF versus PDF group reached full NF 17 days sooner (374/7 vs 40 weeks; p=0.03)
28–316/7: IDF versus PDF group reached full NF 11 days sooner (35 4/7 vs 37 1/7 weeks; p<0.001)
≥32 weeks: IDF versus PDF group reached full NF 3 days sooner (354/7 vs 351/7 weeks; p=0.04).
Affect on discharge
<28 weeks GA, no difference between the IDF versus PDF group (41 3/7 vs 39 4/7 weeks; p=0.10).
28–316/7 weeks GA, IDF group were discharged 9 days earlier (366/7 vs 381/7 weeks; p<0.001).
≥32 weeks GA, the IDF group were discharged 3 days earlier (36 weeks vs 363/7 weeks;
p=0.048)
Although the findings are clear there does need to be the usual acknowledgement that this is not the gold standard RCT but the practice change in the unit was done pretty carefully. The concept is one that makes a great deal of sense regardless. The lack of difference in discharge for the smallest infants makes some sense as it may well be apnea of prematurity that is the last to resolve. There is no disputing however the benefit in earlier discharge for the 28 – 31 6/7 week group. They achieve feeding earlier and go home faster. From a family centred approach this is the best of both worlds. One should not write off the use of this technique in the smallest infants either as they will have their care normalized much earlier with the NG tube being removed and the parents getting to participate and practice feeding much earlier in their course. Although not measured in this study, it would be intriguing to look at the number of patients who were admitted to hospital post discharge with failure to thrive.
Imagine the impact as well on hospital length of stay data if you multiple the reductions in length of stay by the total number of patients seen in these gestational age categories each year. This almost certainly can represent over a year of patient days for many hospitals.
As I see it the direction is clear. We should not force our premature infants to follow a schedule that works for us. Rather use the cues that only they can provide to tell us when and how much milk they desire. Both the parents, infants and our hospitals will benefit.

by All Things Neonatal | Jul 4, 2015 | Breastmilk, LGBT
There is the potential for a very significant issue to arise in the NICU environment in the coming years. As I was preparing the last blog piece following the decision by SCOTUS to allow same-sex marriage in all 50 states I began to think about the so-called ripple effect. In other words, now that the law has been changed, what impacts could this have that might have been unforeseen. The first thought that crept into my mind was that as male same-sex parents they would read the same literature that promotes breast milk feeding in the NICU and no doubt want the best for their infant in the NICU or for that matter any baby. In many NICUs however there are weight or gestational age restrictions indicating who will receive donor breast milk if the mother is not able or not willing to produce her own. In our unit for example we given DBM to all babies currently under 1250g and those recovering from NEC or other bowel surgery. Might men in a same-sex marriage who have adopted a child or used a surrogate who is not willing to breastfeed demand the same?
In looking into this I came across a very strange story from 2013 in which a nurse in the UK offered to “rent her breasts” to gay parents. The story at the time caused a fairly big stir as it raised a number of questions as to safety and the morality of it all. In some ways it was ahead of its time as there have been a number of articles recently addressing the very issue of safety of milk (will be addressed further in the article obtained outside of HMBANA approved breast milk banks.
As same-sex couples increase and many then choose to have children of their own to raise what demands will be made of access to breast milk? There is no question “breast is best” and I have either written or posted to Facebook many articles suggesting decreased incidence of allergy, necrotizing enterocolitis, improvements in the microbiome and many other benefits as well. What do we do in the situation of the same-sex family who declares that they want to provide breast milk to their infant in hospital as it is the best source of nutrition for their infant. If we say for example that their 2 kg, 34 week infant is too big to qualify for DBM is this fair given that they have no option for producing their own milk in the setting of male same-sex partners? Could we as health care providers be labelled as discriminating?
One option is to allow such parents to bring in their own milk but then where do they source it from? Milk purchased online or from the community may be contaminated with bacteria, viruses or contain some cow’s milk as some recent publications have demonstrated. Can we knowingly allow families to bring such milk into the hospital to feed their infant? Perhaps, but only if we have medical legal safeguards in place that protect the hospital from knowingly allowing patients to bring in milk which could be contaminated. Waivers of liability would need to be in place in each hospital permitting such sourcing of milk. If however we strongly discourage such practice will we direct them to the milk bank supplying our local hospital. Herein lies the challenge though. If availability of volume was not an issue, we could provide to all infants in the unit but the reality is there is simply not enough to go around. Furthermore, the larger the infant, the more donor milk they utilize and the more depleted the supply becomes for those of our smallest infants who are most in need of avoiding formula. Finally, who should pay for this milk if the family cannot produce any as in this situation. This is not a case of a mother who could produce but chooses not to but rather a family who is desperate to use what they have read is best but physically is incapable of producing. The same of course could be said for those women who try and cannot or due to prior surgery are unable to produce milk. I believe this is an issue that will come up across the US and Canada and I will be interested to see how it plays out and what role Bioethics may play in helping to resolve some of these questions.
This will be a slippery slope. If male same-sex parents are provided with free access to donor milk I don’t see how donor milk will not be made available to all families who cannot provide their own. Why would the male parents who biologically be unable to provide milk be given this “liquid gold” while other mothers who are pumping round the clock, taking domperidone and seeing a lactation consultant and getting only drops be denied as their newborn is 1600g and above the weight cutoff. I hope you can see the issue of equity popping up in this discussion.
Finally why not allow those parents who are male same-sex partners to simply pay for the milk they need if they don’t qualify for “free” milk under a unit’s program? Sadly the issue then becomes one of equity again. Do we want to care for infants in an environment where the wealthy who can afford to pay for the donor milk from an HMBANA milk bank get it and the poor are only offered formula? I have to admit I realize there are health care systems where this is the case but in Canada where we have a socialized medical system this kind of two tiered system would cause many to become nauseated.
I fear that this issue will come up as the number of people marrying and choosing to have children in same-sex relationships increases. If it leads to a 100% human milk diet for infants in the NICU I would say that is a good thing but I think the road like Winnipeg will be paved with many potholes that we will have to do our best to navigate around.

by All Things Neonatal | Jul 1, 2015 | bioethics, LGBT, Neonatal
This is a lengthier piece than normal but the message at the end is critical to disseminate so I would encourage you to share this if you wish with others to prevent misinformation from being propagated in the media by the sensationalism of a claim by a group of Pediatricians.
My Facebook page became awash in rainbow overlaid posts on Friday. Very quickly I realized as did most of the developed world, that the US Supreme Court ruled in favour of same-sex marriage and just so no one thinks that this will turn into a homophobic piece, I celebrated the change along with many friends and fellow Social Media colleagues.
After the initial excitement began to wane I came across a press release that I found a little shocking given that I belong to the group of people (as a Pediatrician not a member of the organization) that released the statement shown below. The statement is from the American College of Pediatricians
by ADMIN3 on JUNE 27, 2015 in PRESS RELEASE
Dr. Michelle Cretella, President of the American College of Pediatricians in response to the SCOTUS decision today stated, “[T]his is a tragic day for America’s children. The SCOTUS has just undermined the single greatest pro-child institution in the history of mankind: the natural family. Just as it did in the joint Roe v Wade and Doe v Bolton decisions, the SCOTUS has elevated and enshrined the wants of adults over the needs of children.“
Although it is disappointing only 4 of the 9 justices heeded the scientific findings in the
College Brief, the College will continue to proclaim the important unique contributions of both mothers and fathers to the optimal nurturing of all children.
As I went to their website and read about this organization it became clear that this group is mixing Church and State so to speak. Their mission statement states:
Mission of the College
The Mission of the American College of Pediatricians is to enable all children to reach their optimal physical and emotional health and well-being. To this end, we recognize the basic father-mother family unit, within the context of marriage, to be the optimal setting for childhood development, but pledge our support to all children, regardless of their circumstances.
Who are these people and why are they speaking out in such contrast to the American Academy of Pediatrics who in 2013 published their technical report in support of same-sex couple raising children. The AAP which has about 64000 members dwarfs the membership of possibly 200 Pediatricians that comprise the American College of Pediatricians. The smaller group was formed when a group of Pediatricians became upset in 2002 of the AAPs position that endorsed same-sex couples adopting children. The trouble of course with an organization such as this is that their name implies some degree of credibility but in looking at their track record on this issue they have little to none. They are a group that seems to ignore the literature discussed below in favour of quasi-scientific religious literature suggesting harm from such family units. The support of the AAP, the dominant organization in the field was made clear June 26th with this statement. I particularly like the quote from the president of the AAP.
“Every child needs stable, nurturing relationships to thrive, and marriage is one way to support and recognize those relationships,” said Sandra G. Hassink, MD, FAAP, AAP president. “Today’s historic decision by the U.S. Supreme Court supports children in families with same-gender parents. If a child has two loving and capable parents who choose to create a permanent bond, it’s in the best interest of their children that legal institutions allow them to do so.”
Putting aside my natural suspicion of the American College of Pediatricians, it did lead me to ask an important question. Are kids truly better off being raised in a heterosexual marriage? Perhaps there is evidence to show that indeed this is something that we as Pediatricians should be promoting. Looking at the evidence though would suggest otherwise or at least that there is no difference. In 2014 the largest study to date was published by Australian researcher Crouch et al involving 315 parents representing 500 children from same-sex marriages (complete study here). The study involved a questionnaire that would then be compared against population data to see if differences exist between parental units. A little over two-thirds of the parental units were Lesbian. The results demonstrated that in virtually all measures of child health the parental units were equivalent. Curiously, sense of stronger family cohesion was present with the same-sex groups. Possible reasons for this may be related to the way in which children are brought into this world in the two parental unit types. Given that people of the same-sex must plan (there are exceptions no doubt) to procreate there is little chance of the unexpected pregnancy occurring. These are almost all “wanted or chosen” children as opposed to the situation encountered in many pregnancies that are not planned. That is not to say that these children can’t or won’t be loved but the likelihood seems much lower in a LGBT parenting situation due to the planning that is generally required. While the research did not go on to elaborate on why the cohesion might be enhanced this is just my speculation.
Adding to this piece of evidence that these children are likely to have equivalent health to the traditional family rearing model is a well-timed report that surfaced the same week as the Supreme Court Ruling. The report from the Huffington Post challenges that after reviewing 19000 studies on same-sex parenting there can be no conclusion that the children of such families are worse off in any measure of health. Where the above group derives their mission statement from then is certainly not based on science but rather perception.
Back to the American College of Pediatricians (ACOP). I mentioned earlier that I was suspicious of the ACOP and what they portray as advocating for a child’s best health. As a writer of a blog I firmly believe that the buck stops at me with respect to content. If I have a guest writer I am responsible for their content as well as my own. I took the liberty of reviewing a recent piece from their blog and what I saw both shocked me and left me with the certainty that this group is not so much advocating for the health of children as condemning those lifestyles that they do not believe fit the mother-father mold. On June 5th the group released the following piece entitled “P” is for Pedophile. Please click on the link if you have the stomach for it but to give you a taste of what they are talking about here is the quote from the first line of the entry.
“Driving in this morning I began to wonder. Why isn’t the movement of LGBT not the PGBT movement: “P” for pedophile?”
If this group had any credibility by having a professional sounding name, my hope is that this post will spread wide and far to help discredit this organization. The evidence suggests that members of the LGBT community raise just as healthy kids as any of us and any attempts to smear people simply for who they happen to bond with for life amounts to hate and there should be no room in Pediatrics or any other field of medicine for that.

by All Things Neonatal | Jul 1, 2015 | neurology, Parents Corner
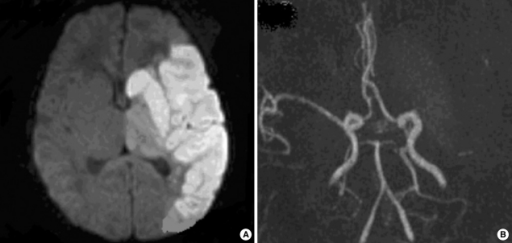
Those are the first words that a parent given the diagnosis of stroke says after hearing the news. It is perhaps one of the worst nightmares a new parent can have. A baby is carried to full term and is born after a seemingly uneventful delivery with normal apgar scores. The family spends the first day together getting to know each other and planning for life outside the hospital. Then sometime between the first and third day of life the parents note their infant shaking an arm or leg repeatedly and call the nurse for assistance. A physician arrives and informs the parents that she believes their newborn is having a seizure and orders phenobarbital, which the parents have never heard of. Shortly afterwards, the family is told that their child needs an MRI and an hour later when the report comes in their world is shattered as they are informed that their infant has a stroke.
At this point their minds flood with memories of elderly relatives or assisted living homes where they met people with strokes and with that their world and dreams are vanishing in front of their wyes.. Lost is the sense that they will have a normal child when they go home but is this what they should expect or is the experience of the family in the following video what is more likely to occur. Such a story told through the experience of a family in this TED talk so well captures the essence of these feelings that I urge you to watch it before moving on.
Shocking as it may be to hear that a newborn has had a seizure, the reality is that the frequency of such events is no different than in adults. Moreover the newborn period has the highest rate of stroke than any other time in childhood. The overall incidence of neonatal seizures is between 1:2000-3000 live births.
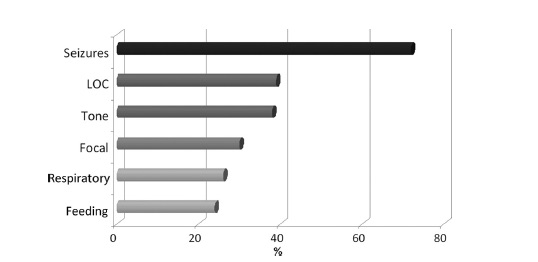
Stroke in a newborn is frightening and from the International Pediatric Stroke Study we have the following figure that provides information as to what these children present with. The symptoms usually present as they did in the case above sometime after 24 hours and consist of the following.
How do they do in the long run?
We are fortunate that the group from Hammersmith has been following a group of neonates since their diagnosis of a middle cerebral artery infarction 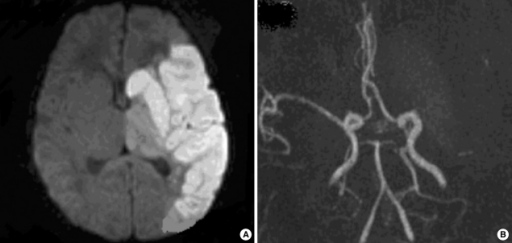 more than 15 years ago and intermittently reported on their neurological outcomes. In the most recent report at age 9 years published in 2008 the results indicated that of the original cohort of 31 patients about 30% had hemiplegia. Interestingly with respect to cognitive outcome the results were just as promising or perhaps even better in that 21/27 assessed at 9 years had normal intelligence. Of the six children who had an IQ below normal, the lower results may have been explained by something other than a neonatal stroke. Two patients were dysmorphic but without a specific diagnosis, one child had autism, one was too shy to be tested so perhaps had normal intelligence and the last child had signs on the original MRI of significant ischemic damage to the brain stem suggesting an additional insult over and above the arterial stroke.
more than 15 years ago and intermittently reported on their neurological outcomes. In the most recent report at age 9 years published in 2008 the results indicated that of the original cohort of 31 patients about 30% had hemiplegia. Interestingly with respect to cognitive outcome the results were just as promising or perhaps even better in that 21/27 assessed at 9 years had normal intelligence. Of the six children who had an IQ below normal, the lower results may have been explained by something other than a neonatal stroke. Two patients were dysmorphic but without a specific diagnosis, one child had autism, one was too shy to be tested so perhaps had normal intelligence and the last child had signs on the original MRI of significant ischemic damage to the brain stem suggesting an additional insult over and above the arterial stroke.
In the Hammersmith cohort almost all patients suffered a left MCA infarct which for reasons that remain unknown is the most common territory affected. The next most common location is the posterior circulation and was the subject of a paper by L de Vries on outcome at a mean age of 36 months.
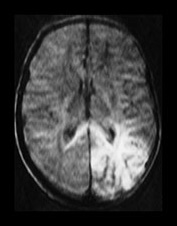 Out of the 17 patients followed, 5 had a global delay with 9 having visual defects. The presence of visual defects is not surprising given the finding that the infarct in the posterior circulation caused injury to the periventricular white matter. This area of the brain of course is where the optic radiations pass through leading to such a disability. Interestingly only one of the 17 that were followed had a hemiplegia.
Out of the 17 patients followed, 5 had a global delay with 9 having visual defects. The presence of visual defects is not surprising given the finding that the infarct in the posterior circulation caused injury to the periventricular white matter. This area of the brain of course is where the optic radiations pass through leading to such a disability. Interestingly only one of the 17 that were followed had a hemiplegia.
As you can see the likelihood in the newborn with a stroke is that they will recover their motor function a great deal and unlike the adult with a similar stroke they are capable of a “rewiring” that provides hope for those parents after the initial devastation of hearing the word “stroke” for the first time.
What features provide a high likelihood of later impairment?
As was shown by Mercuri et al in 1999 the existence of a stroke involving the basal ganglia, internal capsule and hemisphere is predictive of motor impairment. The basal ganglia and other structures mentioned are comprised of several different areas that are labelled in the picture of the brain and are comprised of the putamen, caudate, globus pallidus, the substantia nigra, nucleus accumbens and subthalamic nucleus (the last three not labelled below). Injury to any of these structures along with the internal capsule and other area of the hemisphere would not have a probable good outcome.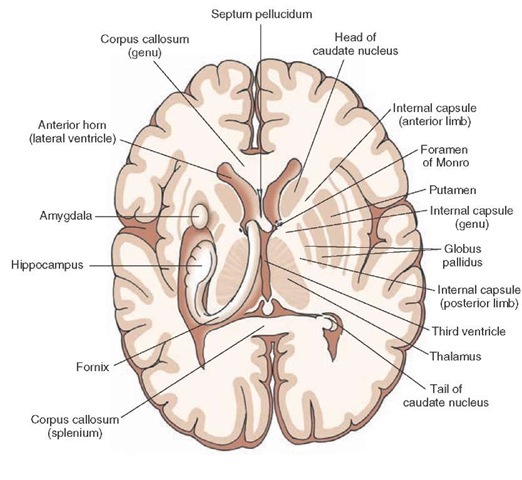
Additional work done by the International Pediatric Stroke Study in 2011 indicated that the following features were predictive of adverse outcome.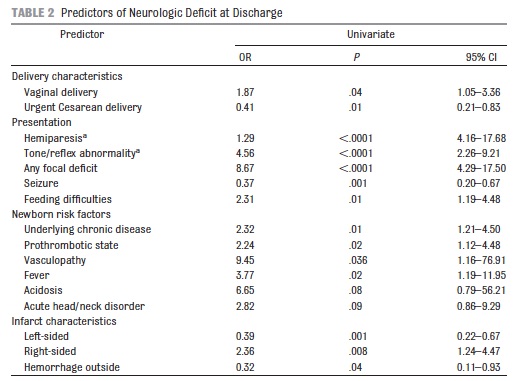
It is important to note that this was outcome at discharge for 250 neonates with stroke. It will be interesting to see if the 50% motor impairment at discharge in this cohort diminishes over time as in the Hammersmith group.
So when we look back at the video that is featured in this post I question whether this family was given good information at the outset. Maybe if someone had put together a post like this to share with them (and to put it into slightly more lay terminology) they would have had fear replaced by cautious optimism.
Who knows maybe this post will reach someone and spare them some of the anguish that I imagine this family must have faced?