If you work in Neonatology you no doubt have listened to people talk in rounds or at other educational sessions about the importance of opening the lung. Many units in the past were what you might call “peepaphobic” but over time and with improvements in technology many centers are adopting an attitude that you use enough PEEP to open the lung. There are some caveats to this of course such as there being upper limits to what units are comfortable and not just relying on PEEP but adding in surfactant when necessary to improve pulmonary compliance.
When we think about giving nitric oxide the importance of opening the lung can’t be stressed enough. I have heard it said many times when a baby has been found to be a “non responder” to inhaled nitric oxide that they may have been so because the lung wasn’t open. What we mean by this is that the distal alveoli are open. One can administer all the iNO in the world but if the majority of alveoli are collapsed the drug can’t get to the pulmonary vasculature and cause the pulmonary vasodilation that is so sorely needed in the presence of hypoxemic respiratory failure. Surfactant and inhaled nitric oxide in the presence of hypoxemic respiratory failure could be a great combo as one would help open the alveoli and then the iNO could address any pulmonary vasoconstriction which might be exacerbating the hypoxemic state.
Study Tests This Theory
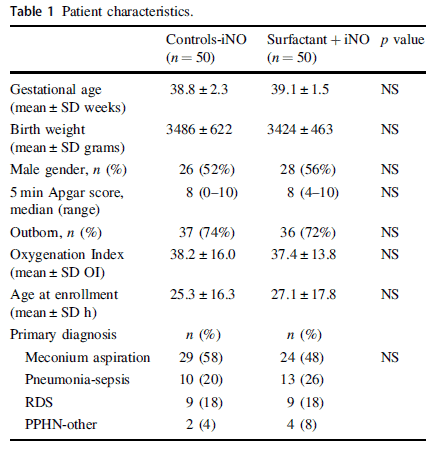
Researchers in Chile led by Gonzalez A published Early use of combined exogenous surfactant and inhaled nitric oxide reduces treatment failure in persistent pulmonary hypertension of the newborn: a randomized controlled trial in the Journal of Perinatology. The concept of this study was to compare in a double blind RCT for 100 patients (based on a power calculation looking for a 25% reduction in treatment failure) whether provision of surfactant as up to 2 doses and iNO would be better than just iNO alone. Included infants needed an oxygenation index (OI = MAPXFiO2/pO2) of 20 or more to qualify and treatment failure was an OI of 40 or more. The patients recruited were similar in common characteristics including types of conditions that would benefit from iNO. RDS, meconium aspiration syndrome and pneumonia certainly have been shown to benefit from surfactant before while in the PPHN category that is questionable. In order to ensure that it was not just the primary disease but pulmonary hypertension that was present as well, all patients required confirmation of pulmonary hypertension prior to enrollment via ECHO with either a TR jet indicating a pulmonary pressure at least 2/3 of systemic or right to left shunting at the ductal or atrial level.
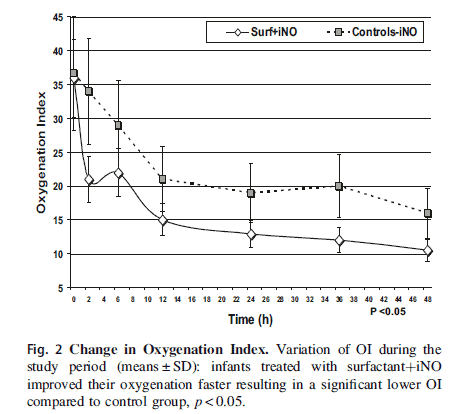
The results of the study demonstrated a clear difference in the primary outcome.
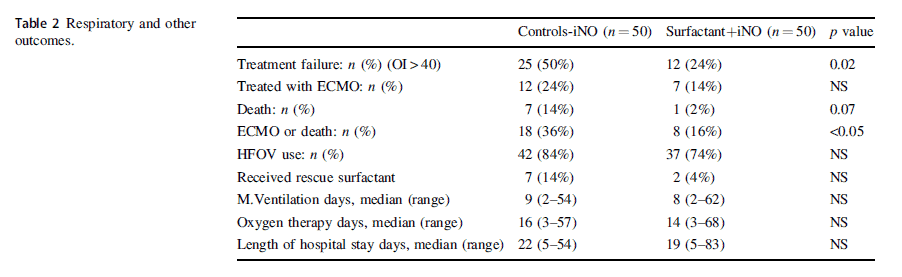
Patients receiving the combination of surfactant prior to starting iNO showed a faster reduction in OI than those receiving iNO alone. In fact the reduction in primary outcome of treatment failure was over 50% different while the power calculation had been based on only a 25% difference. That’s ok as this means there were more than enough patients to demonstrate a difference. As a secondary outcome the rate of ECMO or death was also different between the groups favouring use of surfactant.
It works so now what?
Who doesn’t like seeing a study that confirms what you have long believed. I feel that this study validates the teaching I received throughout the years about ensuring the lung is open before giving iNO. There are some caveats to this however. About 90% of the patients studied had conditions present (RDS, MAS, pneumonia) for which surfactant would have been indicated anyway. If this study had been done let’s say in patients with asphyxia induced pulmonary hypertension and clear lungs the surfactant may have made no difference as the lungs were already open. I mention this as I don’t think readers of this analysis need to jump to the conclusion that every time there is a patient with PPHN that you MUST give surfactant. What I think this illustrates though is the importance of first asking the question if iNO is being considered “Have I opened the lungs?”. The next time you encounter such a patient consider whether you are using enough PEEP and whether surfactant is indicated. The bottom line is if the lung isn’t open then all the iNO in the world isn’t going to make much difference!
The Canadian Pediatric Society has a statement on the use of premedication before non-emergent intubation which was written in 2011 and reaffirmed in 2018. After reviewing available medications for use the recommended strategy was atropine, fentanyl and succinylcholine. This combination does involve three different medications, the first being to prevent bradycardia, the second to sedate and the third to paralyze. With the use of three medications however there is always room for error so it is very alluring to try and use one medication to provide optimal conditions for intubation. As a matter of fact I once tried thiopental as a single agent as a fellow (unpublished) which never saw the light of day due to difficulties with recruitment. Nonetheless I was after a simpler solution to providing good conditions for intubation so it is not surprising that others are also looking at single agents as well.
Propofol Would Seem Like a Good Contender
Propofol has been used in the adult and Pediatric world for some time. It causes a decreased level of conciousness and amnesia surrounding the events for which it was given. It is short acting often wearing off within minutes which would seem perfect for procedural sedation. On the downside one of its side effects is hypotension so in a fragile neonate this might be something to be watch for.
Dose finding study
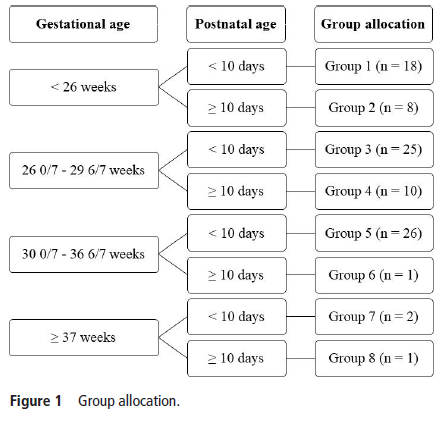
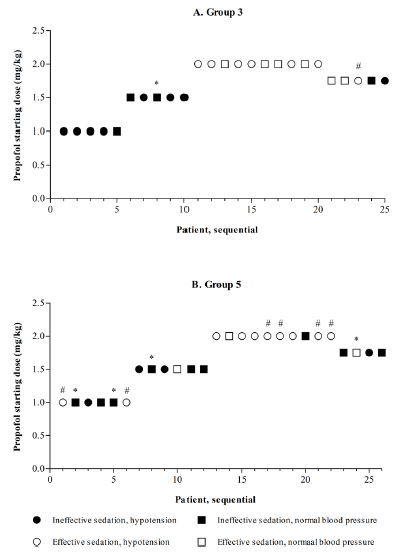
de Kort et al published Propofol for endotracheal intubation in neonates: a dose-finding trial this month. It is an interesting study design for those unfamiliar with dose finding studies. The goal was to begin with a low but starting dose for propofol at 1 mg/kg/dose and escalate by 0.5 mg/kg/dose until adequate sedation was reached WITHOUT signficant adverse side effects. Moreover the authors built on previous work in this area to attempt to break the patients into 8 groups as shown in this figure.
All patients were less than 28 days so allocation was based on gestational age and whether a patient was greater or less than 10 days of age at dosing. Level of intubation readiness was evaluated using a standardized tool called the Intubation Readiness Score.
Side effects were hypotension, myoclonus, chest wall rigidity, persistent respiratory and/or circulatory failure and bronchospasm. Blood pressure was assessed via an indwelling catheter if available or by cuff if not available. Importantly any mean blood pressure after provision of propofol less than the gestational age met the criteria for declaring hypotension.
The Findings
The study was terminated early due to low inclusion in some groups after 91 total patients had been enrolled. In the end there were only enough patients in Groups 3 (26 – 29 weeks and <10 days) and 5 (30 – 36 weeks and < 10 days) enrolled to analyze fully. The results of the dose finding analysis are shown below.
Walking through group 3, there were 5 patients enrolled at the 1 mg/kg level and based on poor levels of sedation in all the dosing for next 5 were increased to 1.5 mg/kg. As intubating conditions improved, the authors found that at a dose of 2 mg/kg while conditions were optimal, hypotension became a significant problem with 59% being hypotensive. The management of hypotension included 54% needing volume resuscitation and inotropes in 10%. Curiously the hypotension often did not appear until 2 hours or more after drug delivery. When the authors did a step down to 1.75 mg/kg as a intubation dose they found it was inadequate for providing good conditions for intubation albeit with less hypotension.
Not the right drug
The goal of this study was to find the optimal dose that provided good intubation conditions without significant side effects. The strength of this study was that it included babies across a wide range of gestational ages from 26+0 to 36+6 weeks gestational age. While the authors were unable to recruit enough patients to fill each group the stoppage of the study made sense as it was clear that the goal of the study would not be met. Propofol would be a great single agent if it weren’t for the issues found in this study. This is not to say that the drug is a poor choice for Pediatrics but in the Neonatal world I just don’t think it has a place. I would welcome further testing on other single agent drugs but that of course is an analysis for another post!
To be sure there are fans of both HFNC and CPAP out there. I have often heard from other Neonatologists that they use HFNC and find positive results while other centres refuse to use it in favour of the tried and true CPAP. Turning to the literature you will find some conflicting results with some studies suggesting equity and others more recently favouring CPAP. There has been speculation as to why one would be superior to the other and now we appear to have some answers as to where the differences lie.
A Physiologic Study
Liew et al published Physiological effects of high-flow nasal cannula therapy in preterm infants this month in an elegant study of 40 infants. The study was fairly simple in design either randomizing infants <37 weeks to starting with nCPAP +6 and then transitioning to 8 l/min HFNC followed by stepwise reductions of 1 l/min until 2 l/min was reached or the reverse, starting with 2 l/min and working their way up and then transitioning to nCPAP+6. All infants were on one or the other modality at the start and were all at least 3 days old, they were randomized to one or the other arm regardless of where they started off. Physiologic measurements were taken at each step including the following:
Mv -Minute ventilation
pEEP – nasopharyngeal end-expiratory pressure
pEECO2 -nasopharyngeal end-expiratory CO2
RR – respiratory rate;
SpO2 – oxygen saturation
TCCO2 – transcutaneous CO2
Vt – tidal volume
A Fabian device was used to deliver either HFNC or CPAP at the different flows for all patients.
The Results
The authors certainly found some interesting results that I think shed some light on why comparisons of HFNC and CPAP have been so inconsistent.
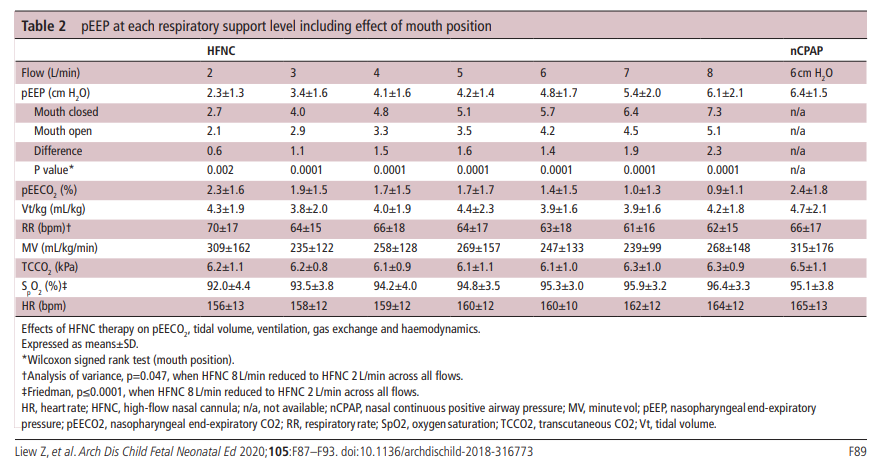
Table 2 contains the results of the study and I will point out the main findings below.
1. Flow matters – Compared to nCPAP+6 which is fairly consistent flows below 6 l/min deliver pEEP that is below 6 cm H2O.
2. Keep the mouth shut – With CPAP whether the mouth is open or closed the Fabian device delivers +6 cm H2O. As you can see from the table, when the mouth is open transmitted pressures drop off substantially. The infant put on a flow of even 6-8 l/min of HFNC sees pressures less than +6 consistently.
3. As flows increase end expiratory CO2 decreases. HFNC seems to help wash out CO2
4. Low flow rates on HFNC do not seem to help with ventilation as much as higher flow rates. In order to maintain Mv these infants at 2 l/min flow become tachypneic. The low pressures produced likely cause some atelectasis and hence tachypnea.
Size matters! Beware of excessive pressures.
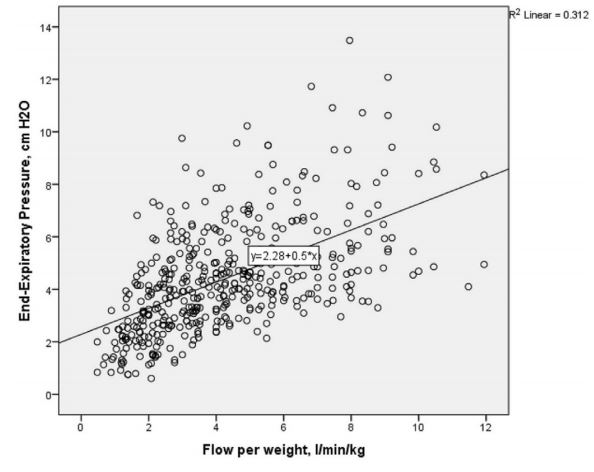
An additional finding of this study was that on “multiple linear regression, flow rate, mouth position, current weight and gestation but not prong-to-nares ratio significantly predicted pEEP and account for a significant amount of its variance (F(4431)=143.768, p<0.0001), R2=0.572, R2=adjusted 0.568).” Essentially, infants under 1000g in particular could see pEEP levels as high as 13 cm H2O with flows of 8 l/min. The variability in transmitted pressures with HFNC is shown nicely in this figure from the study.
As flows increase above 6 l/min the actual pressures delivered become less reliable.
Conclusions
Looking at this data, it becomes evident why HFNC may be failing in its attempt to dethrone nCPAP. In order to achieve higher pressures and provide comparable distending pressure to nCPAP you need higher flows. With higher flows though come the problem of greater variability in delivered pressure. While the average pressure delivered may be equivalent or even higher than a CPAP of +6, in some infants (especially those below 1000g) one may be delivering significantly higher pressures than intended which may help with oxygenation and preventing intubation but others may be seeing far less than needed.
What it comes down to is that nCPAP is better at delivering a consistent amount of pressure. Studies using lower flows of HFNC likely failed to show superiority to CPAP as they just didn’t deliver enough pressure. An example of this was the study by Roberts CT et al Nasal High-Flow Therapy for Primary Respiratory Support in Preterm Infants, in which flows of 6-8 l/min were used. Other studies using higher pressures could have been problematic due to open mouths, or larger babies not receiving as much benefit.
I am not saying that we should throw out HFNC entirely however. Depending on the unit you practice in you might not be able to use CPAP but HFNC may be allowed. If you had to choose between no support or HFNC I would likely go with the HFNC. For me at least, if I want to delivery reliable pressures in my tertiary care NICU I will be calling for the CPAP.
I have written about non-traditional methods of providing surfactant to newborns previously. The practice of intubating a preterm infant to administer surfactant and leaving the endotracheal tube in with a slow wean of ventilation is mostly a thing of the past (at least in my units). Strategies have evolved and have seen the development of the INSURE technique, LISA methods, use of an LMA to delivery surfactant and even simple deposition into the pharynx all with variable success.
Poractant alfa at 200 mg/kg was used in this study and delivered via aerosolization using a vibrating membrane called the eFlow. The authors chose to look at infants from 29 0/7 to 33 6/7 weeks at birth and stratified them into two groups of 29 0/7 to 31 6/7 and 32 0/7 to 33 6/7 weeks. They estimated a need for 70 babies based on an anticipated failure rate of 30% in the control group vs 5% in the treatment group. Unfortunately, due to several reasons the study was only able to recruit 64 babies for randomization before being stopped due to the recruitment issues. The design of the study included adequate blinding with a sham procedure and there were predefined “failure criteria” necessitating intubation at the outset of the study. These criteria are acceptable to me as they are similar enough to my own practice and were:
1. FiO2 >0.35 over more than 30 min OR FiO2 >0.45 at
anytime.
2. More than four apnoeas/hour OR two apnoeas requiring bag
and mask ventilation.
3. Two capillary blood gas samples with a pH <7.2 and partial pressure of carbon dioxide >65 mm Hg (or partial pressure
of carbon dioxide in arterial blood (PaCO2) >60 mm Hg if
arterial blood gas sample).
4. Intubation deemed necessary by the attending physician.
What did they find?
The primary outcome CPAP failure within 72 hours of birth was indeed different in the two groups.
CPAP failure by 72 hours
CPAP + surfactant
11/32 (34%)
CPAP
22/32 (69%)
(RR (95% CI)=0.526 (0.292 to 0.950))
Clearly the event rates were quite off from what they expected in the power calculation but given that they found a difference as opposed to no difference at all the fact that they didn’t recruit the numbers they planned is of less importance.
However, what is interesting is when they looked at the planned analysis by stratification an interesting finding emerged.
Group 1 (29 0/7 to 31 6/7)
CPAP failure by 72 hours
CPAP + surfactant
12/21 (57%)
CPAP
12/19 (63%)
(RR (95% CI)=0.860 (0.389 to 1.90))
Group 2 (32 0/7 to 33 6/7
CPAP failure by 72 hours
CPAP + surfactant
1/11 (9%)
CPAP
10/13 (77%)
(RR (95% CI)=0.254 (0.089 to 0.727))
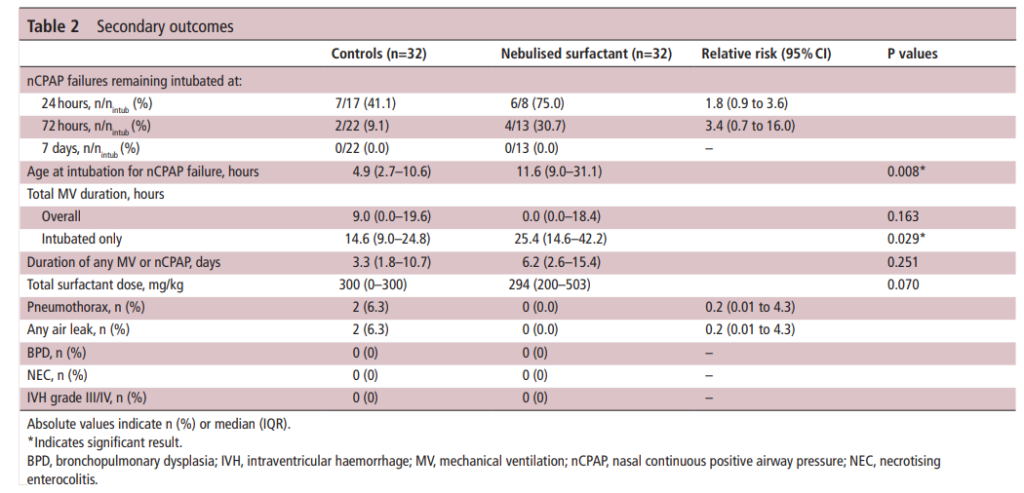
There were a number of secondary outcomes looked at as well which may be of interest to you but as the numbers here are quite small I will not comment other than to say there was no increased incidence of complications with surfactant administration in this fashion. Also for those who ultimately failed CPAP the time when they did so was quite delayed compared to CPAP alone. Age at intubation for nCPAP failure, hours 4.9 (2.7–10.6) 11.6 (9.0–31.1) 0.008*
What can we take from this?
I believe these results are encouraging even if the study is a small one. The message I take from this study is that aerosolization of surfactant delivers some amount of product to the lungs. Those with more significant RDS or smaller lungs (those in the 29 0/7 to 31 6/7 group) may not get enough surfactant to treat their RDS sufficiently to avoid intubation. Those with less significant RDS or a larger number of alveoli get “enough” of a dose delivered to the alveoli to make a difference and avoid intubation. It is worth stressing that there can be no specific comment about using this strategy in even more immature infants as they weren’t tested. If I had to guess though, I would expect no difference given the findings in the smaller group.
As a physician responsible for transport though I am interested in the potential benefits to those born in non-tertiary centres. Many centres lack individuals with the confidence and skill to regularly place endotracheal tubes. For these centres it may be that providing nebulized surfactant could delay the time to treatment failure, allowing more time for a trained transport team to arrive. Training of course would be needed in these centres on how to administer surfactant in this way but it is an interesting concept to consider. With a near tripling of the average time to treatment failure the extra hours on CPAP would be much appreciated when weather delays or difficulty securing air assets means long delays in transport team arrivals.
To be sure this isn’t the last study of this kind but it certainly is an interesting start and one that will no doubt produce questions that will help formulate the next study design.
A real change is coming and with this post you will get a glimpse into where the next big thing in Neonatology is likely to be. A catchy title for sure and also an exaggeration as I don’t see us abandoning the endotracheal tube just yet. There has been a lot of talk about less invasive means of giving surfactant and the last few years have seen several papers relating to giving surfactant via a catheter placed in the trachea (MIST or LISA techniques as examples). There may be a new kid on the block so to speak and that is aerosolized surfactant. This has been talked about for some time as well but the challenge had been figuring out how to aerosolize the fluid in such a way that a significant amount of the surfactant would actually enter the trachea. This was really a dream of many Neonatologists and based on a recently published paper the time may be now for this technique to take off.
A Randomized Trial of Aerosolized Surfacant
Minocchieri et al as part of the CureNeb study team published Nebulised surfactant to reduce severity of respiratory distress: a blinded, parallel, randomised controlled trial. This trial set out to obtain a sample size of 70 patients between 29 0/7 to 33 6/7 weeks to demonstrate a difference in need for intubation from 30% down to 5% in patients treated with CPAP (30% was based on the historical average). The authors recognizing that the babies in this GA bracket might behave differently, further stratified the randomization into two groups being 29 0/7 – 31 6/7 weeks and 32 0/7 to 33 6/7 weeks. Those babies who were on CPAP and met the following criteria for intubation were either intubated in the control group and given surfactant (curosurf) using the same protocol as those nebulized or had surfactant delivered via nebulisation (200 mg/kg: poractant alfa) using a customised vibrating membrane nebuliser (eFlow neonatal). Surfactant nebulisation(100 mg/kg) was repeated after 12 hours if oxygen was still required. The primary dichotomous outcome was the need for intubation within 72 hours of life, and the primary continuous outcome was the mean duration of mechanical ventilation at 72 hours of age.
Criteria for intubation
1. FiO2 >0.35 over more than 30 min OR FiO2 >0.45 at
anytime.
2. More than four apnea/hour OR two apnea requiring BVM
3. Two cap gases with pH <7.2 and PaCO2 >65 mm Hg (or) >60 mm Hg if arterial blood gas sample).
4. Intubation deemed necessary by the attending physician.
Did It Work?
Eureka! It seemed to work as 11 of 32 infants were intubated in the surfactant nebulisation group within 72 hours of birth vs.22 out of 32 infants receiving CPAP alone (RR (95% CI)=0.526 (0.292 to 0.950)). The reduction though was accounted for by the bigger babies in the 32 0/7 to 33 6/7 weeks group as only 1 of 11 was intubated when given nebulized surfactant compared to 10 of 13 managed with CPAP. The duration of ventilation in the first 72 hours was not different between the groups: the median (range) 0 (0–62) hour for the nebulization group and 9 (0–64) hours for the control group (p=0.220). It is important in seeing these results that the clinicians deciding whether infants should be intubated for surfactant administration were blind to the arm the infants were in. All administration of curosurf via nebulization or sham procedures were done behind a screen.
The total number of infants randomized were 66 so they did fall shy of the necessary recruitment but since they did find a difference the results seem valid. Importantly, there were no differences in complications although I can’t be totally confident there really is no risk as this study was grossly underpowered to look at rarer outcomes.
Breaking down the results
This study has me excited as what it shows is that “it kind of works“. Why would larger babies be the ones to benefit the most? My guess is that some but not a lot of surfactant administered via nebulization reaches the alveoli. Infants with lesser degrees of surfactant deficiency (32 0/7 to 33 6/7) weeks might get just enough to manage without an endotracheal tube. Those infants (in particular less than 32 0/7 weeks) who have more significant surfactant deficiency don’t get enough and therefore are intubated. Supporting this notion is the overall delay in time to intubation in those who were intubated despite nebulization (11.6 hours in the nebulization group vs 4.9 hours in the control arm). They likely received some deposition in the distal alveoli but not enough to completely stave off an endotracheal tube.
One concerning point from the study though had to do with the group of infants who were intubated despite nebulization of surfactant. When you look at total duration of ventilation (hours) it was 14.6 (9.0–24.8) in the control arm vs 25.4 (14.6–42.2) p= 0.029*. In other words infants who were intubated in the end spent about twice as long intubated as those who were intubated straight away. Not a huge concern if you are born at 32 weeks or more but those additional thousands of positive pressure breaths are more worrisome as a risk for CLD down the road.
As it stands, if you had an infant who was 33 weeks and grunting with an FiO2 of 35% might you try this if you could get your hands on the nebulizer? It appears to work so the only question is whether you are confident enough that the risk of such things as pneumothorax or IVH isn’t higher if intubation is delayed. It will be interesting to see if this gets adopted at this point.
The future no doubt will see a refinement of the nebulizer and an attempt to see how well this technique works in infants below 29 weeks. It is in this group though that prolonging time intubated would be more worrisome. I don’t want to dismiss this outright as I see this as a pilot study that will lead the way for future work that will refine this technique. If we get this right this would be really transformative to Neonatology and just might be the next big leap.