To say this has been a labour of love is an understatement. So many people have contributed to the new position statement for the Canadian Pediatric Society (CPS).
My co-author Dr. Seth Marks from Pediatric Endocrinology spent countless hours reviewing the evidence and fielding seemingly endless questions from reviewers and myself. The support from the CPS was also much appreciated as the back and forth from so many who expressed opinions would have been difficult to manage without their support. What I hope you will find as you read this is the best appraisal of the evidence and directions for care that we could come to in 2019. Where things will stand by the time we make it to the next revision will be interesting to see.
Big Accomplishment
For those who have used the Acute Care of At Risk Newborns (ACORN) program you will be pleased to know that the upcoming new version of this program is completely alligned with the approach outlined in the CPS statement. Given that the first version of ACORN and the CPS were not aligned and caused great discussion and distress at times, we feel this is a big accomplishment.
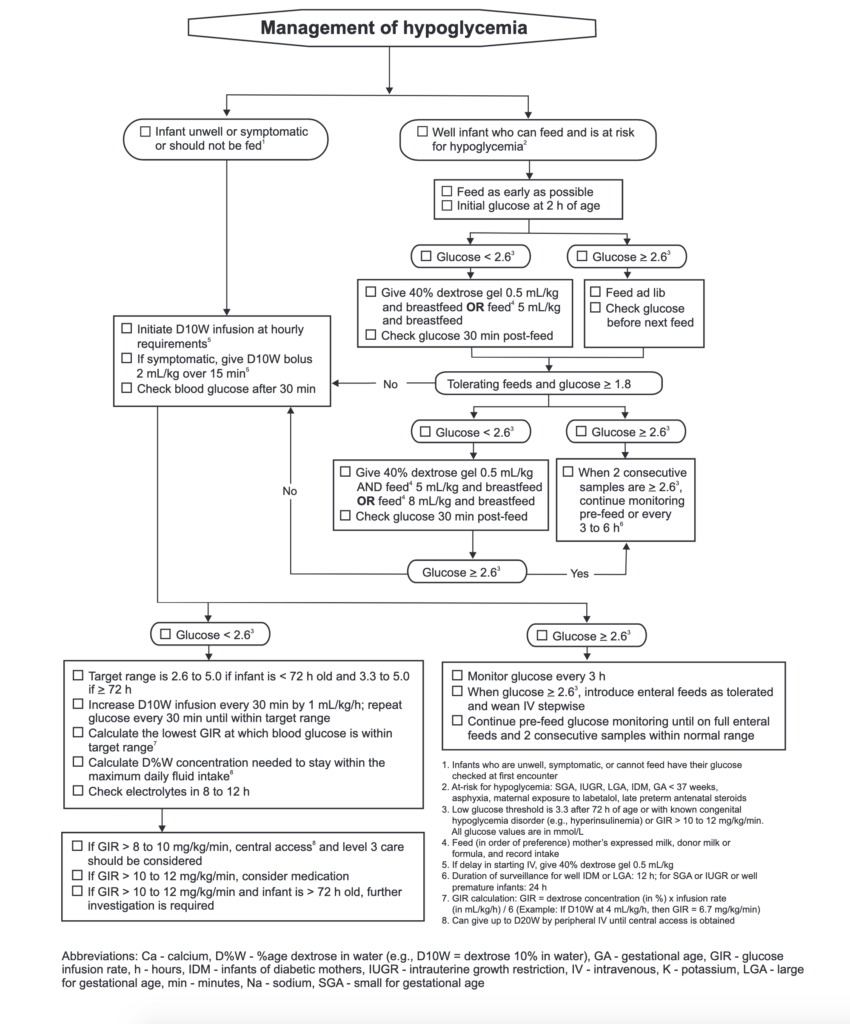
The algorithm for managing hypoglycemia is clean and easy to follow (I think) and we hope such clarity will greatly help with managing those infants at risk.
Main Questions for the Future
We remain a country divided (much like the recent election) with respect to dextrose gels usage. There are centres which are leary of using adult formulations of dextrose gel in newborns whereas others have adopted such treatments with success. The algorithm and statement address the approach to using dextrose gels or what to do if one wishes to avoid such use. With time, local products or a national brand designed specifically for newborn use may come to be and this will need to be addressed at some point.
Changing the threshold at 72 hours and beyond to require glucose levels of greater than or equal to 3.3 mmol/L may lead some to be worried about a ramp up in admissions but at least locally we have not seen this. In the end those with persistent causes of hypoglycemia will manifest one way or the other and whether it is before or after discharge from the hospital may be a reflection of what threshold you feel comfortable using.
Will local guidelines be affected by adopting the changes outlined in this statement? I suspect so and would welcome feedback before the next version of this document is worked on to determine what if any ramifications (positve or negative) such approaches have had.
No doubt with many changes compared to the previous version of the statement there may be some surprises. Keep an open mind and look at the evidence presented. In other cases the lack of evidence has motivated a change in position. Either way we believe this is the best approach to care for at risk newborns given what we know today.
Last week marked a changing of the guard at the Canadian Paediatric Society, as Dr. Thierry Lacaze stepped down as the chair of the Fetus and Newborn Committee. We produced many important position statements and practice points under his leadership and I hope to continue this trend.
The aim of this committee is to provide guidance across disciplines to all those who care for newborns. Topics we examine include everything from surfactant treatment, to approaches to the infant with jaundice and hypoglycemia, to how to manage infants born to opioid-dependent mothers.
I plan on using all the channels at my disposal, including digital and social media communications, to proactively inform and seek input from interested health care providers about the sorts of topics on the committee’s agenda.
It’s not uncommon for those outside of the organization to approach my colleagues and me with their feedback. “You should really work on this or that,” is a phrase I’ve grown accustomed to hearing. We are often doing just that, and I think it’s important for our colleagues to know.
As different locations across the country seek to put in place local guidelines based on CPS research, I think it would be helpful to know if there’s something new on the horizon that will impact their work. Why spend a lot of time developing a guideline based on a statement or practice point that is about to change?
My pledge to you
In my new role as chair, I promise to keep you apprised and informed about the topics on the committee’s agenda. When a document is likely to significantly affect the approach to patient care, I will do my best to alert you. If you have topics that you believe are in need of a national position or guideline, please send me an e-mail at [email protected] for consideration by the committee.
This practice point focuses on circumstances that are likely to involve paediatric health professionals. Recommendations are provided for compassionate communication, bereavement, sibling care and counselling to support families.
This practice point focuses on the effects of opioid withdrawal and current management strategies in the care of infants born to mothers with opioid dependency.
Upcoming publications (in no particular order)
Hypothermia for newborns with hypoxic ischemic encephalopathy (revision)
Brigitte Lemyre, Vann Chau
This document reviews indications, contra-indications, discusses the requirements, in terms of expertise and specialized equipment, of units where hypothermia should take place. Additionally, the timing of the first MRI and when to do a follow-up MRI are clearly delineated.
Guidelines for vitamin K prophylaxis in newborns Eugene Ng, Amanda Loewy
Clear recommendations are provided for provision of vitamin K dosing via the intramuscular route. The evidence for oral vitamin K is reviewed and a clear position is taken on its use in newborn care.
Facilitating discharge home of the healthy infant (revision)
Brigitte Lemyre, A. Jerfferies, P. O’Flaherty
This statement provides guidance for health care providers to ensure the safe discharge of health term infants who are born in hospital and who are ≥ 37 weeks’ gestational age.
Imaging of the term neonatal brain
Ann Jefferies, S. Sorokan, Steven Miller, Ken Poskitt
This position statement describes the principles, roles and limitations of three imaging modalities and makes recommendations for appropriate use in term neonates.
It has been almost a year since the CPS released the new statement on car seat testing prior to discharge. As both the author and a person with a personal bias I am deeply curious what impact the change in position has had on the community out there. My question to you the reader is whether the statement had any influence on your local practice. Now if you are in the US I know the answer already should be a resounding no as you are still likely to follow the recommendation of the AAP. What about the rest and in particular those that read the CPS guidelines.
In 2017 is the test still relevant?
Original post below…
The day has finally come that the CPS has released a new statement on Infant Car Seat Testing. While I am the author of the statement and this may sound like self promotion, I am putting it here as there are many followers across Canada and elsewhere who may see this change in position here but not through the CPS distribution network.
This is an important statement not because I wrote it but due to the state of testing in Canada. Through personal communications it is apparent that the test has fallen out of favour in some jurisdictions in Canada while others have been steadfast in a pass of the test as a criterion for discharge.
As you will see, the Fetus and Newborn Committee have created a clear recommendation on this test which represents a significant departure from the previous position.
How will your centre respond to this change? I would welcome feedback on this from readers and am interested to see if the AAP will follow suit sometime in the future.